Article Text

Abstract
Objectives Recent evidence suggests that occupational physical activity (OPA) is associated with adverse cardiovascular health, whereas leisure time physical activity is protective. This study explored explanatory physiological mechanisms.
Methods Nineteen males (68% white, age=46.6±7.9 years, body mass index=27.9±5.1 kg/m2) with high self-reported OPA wore activity (ActiGraph and activPAL) and heart rate (HR) monitors for 7 days and an ambulatory blood pressure (BP) monitor on one workday and one non-workday. Mixed effects models compared cardiovascular variables (24-hour, nocturnal, waking and non-work time HR and BP) and nocturnal HR variability (HRV) on workdays versus non-workdays. Additional models examined associations of daily activity (steps, light physical activity (LPA) and moderate-to-vigorous physical activity (MVPA)) with cardiovascular variables. Workday by daily activity interactions were examined.
Results 24-hour and waking HR and diastolic BP as well as non-work diastolic BP were significantly higher on workdays versus non-workdays (p<0.05 for all). However, no difference in systolic BP or nocturnal HR or BP was observed between work and non-workdays (p>0.05 for all). Low-frequency and high-frequency power indices of nocturnal HRV were lower on workdays (p<0.05 for both). Daily steps and LPA were positively associated with 24-hour and waking HR on work and non-workdays. Significant interactions suggested MVPA increases HR and lowers nocturnal HRV during workdays, with the opposite effect on non-workdays.
Conclusions Cardiovascular load was higher on workdays versus non-workdays with no compensatory hypotensive response following workdays. Daily MVPA may differentially affect ambulatory cardiovascular load and nocturnal HRV on workdays versus non-workdays, supporting the physical activity health paradox hypothesis.
- workload
- occupational Health
- physical exertion
- exercise
- health promotion
Data availability statement
Data are available on reasonable request.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The proposed physical activity health paradox suggests that leisure-time physical activity and occupational physical activity may have opposing cardiovascular health effects.
Some mechanistic pathways have been hypothesised to explain these paradoxical associations; however, little confirmatory research has been completed.
What are the new findings?
A 24-hour cardiovascular load on workdays with high amounts of occupational physical activity is significantly higher than on non-workdays.
Cardiovascular load may remain elevated following workdays compared with non-workdays, suggesting inadequate recovery.
Preliminary evidence suggests lower parasympathetic activity following workdays compared with non-workdays.
Daily moderate-to-vigorous physical activity may be differentially associated with 24-hour cardiovascular load and nocturnal heart rate variability on workdays versus non-workdays.
How might this impact on policy or clinical practice in the foreseeable future?
If the paradox hypothesis is indeed true, as our results preliminarily support, physical activity recommendations may need to consider occupational and leisure-time physical activity separately due to opposing health implications.
Introduction
Leisure-time physical activity (LTPA) is known to promote cardiovascular health,1 while accumulating data suggest occupational physical activity (OPA) may have opposing effects.2–4 Specifically, moderate-to-high amounts of self-reported OPA have been associated with increased risk for cardiovascular disease and all-cause mortality in most3 5–7 but not all8 9 studies. The conflicting OPA and LTPA effects have been coined the physical activity health paradox.10
High OPA jobs may have different activity patterns which could adversely affect cardiovascular health.10 11 While acute LTPA increases heart rate (HR) and blood pressure (BP) during exercise, 24-hour cardiovascular load decreases due to compensatory hypotensive responses.12 In contrast, it is hypothesised that low-intensity, long duration OPA with little recovery would elevate 24-hour HR and BP, increasing cardiovascular disease risk and all-cause mortality.10 13 Furthermore, autonomic dysfunction, being closely related to poor cardiovascular regulation and risk, has been proposed to result from high OPA.10 14 Though these mechanisms could help explain the paradox, they remain speculative with limited confirmatory research.
Thus, the current study aimed to address this knowledge gap by leveraging a within-subject design, objective physical activity assessment and field-based cardiovascular monitoring to expand understanding of the biological plausibility behind the physical activity health paradox.2–4 7 10 14 15 Consistent with the proposed mechanisms, we hypothesised that 24-hour cardiovascular load would be greater and autonomic function would be lower on workdays versus non-workdays. Further, we hypothesised that cardiovascular responses to physical activity would be different between work (OPA) and leisure (LTPA) contexts.
Methods
This within-subject, observational study compared cardiovascular responses on workdays versus non-workdays among nineteen middle-aged men working in the food service, material moving, healthcare or maintenance industries which are known to have high amounts of light-intensity OPA.16 Participants were recruited via flyers and emails distributed to targeted occupational groups in the Pittsburgh region. Eligible participants were male, aged 35–59 years, working full-time (≥30 hours/week) and self-reporting predominantly light-intensity job tasks (≥75% walking, light movement or standing), had no known cardiovascular disease, and not currently taking medications affecting cardiovascular responses (eg, beta-blockers, ACE inhibitors). Those who reported mobility limitations, had high resting BP (ie, systolic ≥150 mm Hg or diastolic ≥95 mm Hg), reported working overnight shifts, reported working a second job, or were not ‘low risk’ on the Physical Activity Readiness Questionnaire (PAR-Q)17 were excluded. Women were excluded to limit the influence of previously demonstrated sex differences in the association between OPA and cardiovascular health.8 9 16 All procedures were registered on ClinicalTrials.gov (#NCT04075279). Participants provided written informed consent prior to enrolment.
Participants completed a baseline laboratory assessment followed by a 7-day free-living assessment protocol. Participants verbally confirmed abstention from food, caffeine, exercise and nicotine for ≥1 hour before the visit. After informed consent, the following measurements were obtained: (1) PAR-Q,17 medical history and demographics; (2) resting HR and BP on the non-dominant arm using a validated oscillometric device (HEM-705CPN, Omron, Lake Forest, Illinois, USA); and (3) height and weight using a digital scale and wall-mounted stadiometer. Then, each participant meeting criteria completed a submaximal treadmill exercise test using a modified Balke protocol up to 80% of their age-predicted maximal HR to estimate cardiorespiratory fitness.18 Fifty-eight participants were initially screened; 22 were screened as ineligible due to age (n=4), insufficient OPA (n=6), working overnight shifts (n=2), working a second job (n=3) or being determined to be greater than low risk on the PAR-Q (n=7). Fourteen participants were screened as eligible but did not schedule or report for a baseline assessment. As such, 22 eligible participants reported for an assessment visit, during which three became ineligible (n=2 had high resting BP and n=1 had an abnormal cardiovascular response to exercise), leaving a total of 19 participants enrolled.
Following baseline measurements, physical activity was objectively monitored for seven free-living days using validated methods: thigh-worn inclinometer/accelerometer (activPAL3 micro, PAL Technologies, Glasgow) and waist-worn tri-axial accelerometer (GT3X-BT, ActiGraph, Pensacola, Florida, USA).19 Each participant completed a paper diary of work, sleep and monitor wear times which were used to characterise activity time as work, non-work or sleep. Daily activPAL data were considered valid with ≥10 hours/day of valid, waking wear time.20 Data were exported in 15 s epochs and further integrated into 60 s epochs before analyses to align with ActiGraph data. Data were classified as sedentary behaviour (SED), stepping or standing using manufacturer-provided software.20 ActiGraph data were integrated as 1 min epochs using ActiLife software (ActiGraph) and considered valid with ≥10 hours/day of valid wear time during the waking time interval identified using the activPAL data and participant diary.21 Epochs spent in moderate and vigorous physical activity were identified using Freedson cutpoints.22 Using both activPAL and ActiGraph data, daily number of steps, time spent in light intensity physical activity (LPA), moderate-intensity physical activity and vigorous-intensity activity were calculated. Total moderate-to-vigorous intensity activity (MVPA) was calculated as moderate + (vigorous × 2).23 Daily steps, LPA and MVPA were used in analyses to represent a wide spectrum of activity profile metrics.
HR and HR variability measurement
A chest HR monitor (H10 Bluetooth, Polar) continuously measured HR and HR variability (HRV) for 7 days. Participants only removed it during bathing or water activities and recorded any removal in their diary. The HR monitor was paired via Bluetooth with the ActiGraph on initialisation which stored the HR data continuously at a 1 millisecond beat-to-beat resolution. Two ActiGraph monitors were worn continuously and the monitors were timed to switch data collection automatically after 4 days to ensure battery life. HR data were downloaded as interbeat R-R intervals using ActiLife software. After removing erroneous HR measurements (ie, HR=0 beats/min), average 24-hour HR was calculated for all wear days, workdays and non-workdays where the beginning of each 24-hour day was defined as the participant reported wake-up time. Due to the variation in wake time and monitor non-wear, the duration of all 24-hour calculations were not necessarily 24 hours in duration (mean=22.7 hours, SD=3.0 hours, range=13.4–29.5 hours).
Nocturnal HR was measured every night of the monitoring period with the chest HR monitor and used to determine HRV parameters with Kubios HRV software (Kubios HRV Premium V.3.2, Kubios).24 After dropping all 5 min periods with erroneous HR values, each 5 min period throughout the self-reported sleep bout for each night was processed separately to estimate all HRV parameters. Then the mean of each HRV parameter across all 5 min periods within the night was calculated to standardise the recording duration, limiting the potential influence of sleep duration.25 Mean beat-to-beat interval (RR), root mean square successive difference (RMSSD), SD of normal to normal intervals (SDNN), low-frequency power (0.04–0.15 Hz; LF), high-frequency power (0.15–0.4 Hz; HF) and LF/HF ratio were calculated for each night using automated protocols in Kubios.26 Automatic artefact correction was applied by using a time series consisting of differences between successive R-R intervals to separate normal and ectopic beats.27 The HRV variables of RMSSD, LF, and HF had non-normal distributions and were log-transformed for analyses. Lastly, mean nocturnal HRV values were calculated across all nights, nights following workdays and nights following non-workdays.
Ambulatory BP measurement
Each participant wore an ambulatory BP monitor (ABPM; Oscar 2, SunTech Medical, Morrisville, North Carolina, USA) on their non-dominant arm for 24 hours on one workday and one non-workday during the monitoring period. ABPM wear days did not start until at least 24 hours following the assessment visit to limit influence from the fitness test. Following the assessment visit, participants were given the ABPM, instructed on proper wear, and given standardised instructions on how and when to wear the monitor.28 BP was measured every 30 min during the day and every 60 min during the participant’s self-reported typical sleep times.28 ABPM data were downloaded using Accuwin Pro software (Suntech Medical) and notable errors (eg, artefacts or erratic oscillometric signals) were removed.28 All BP measurements were weighted by the amount of time they represent during the day due to variability in the duration between measurements. Daily averages were computed as 24-hour, waking, nocturnal, work and non-work time based on the participant diary.
Analytical approach
Descriptive statistics summarised demographic factors and fitness. Mixed effects models with a random effect by participant (accounting for within-subject correlations across daily repeated measures) and an unstructured covariance structure compared all daily cardiovascular outcomes (eg, 24-hour, nocturnal, waking, and non-work time HR, BP and nocturnal HRV) on workdays versus non-workdays. The magnitude of effect across day type (work vs non-workday) was calculated as f2; values of f2 ≥0.02, f2 ≥0.15 and f2 ≥0.35 can be interpreted as small:, medium, and large, respectively.29 Similarly, mixed effects models examined the association between continuous daily activity levels with all cardiovascular outcomes. Interaction terms (type of day (work or non-work) by continuous daily activity level) were included in these models to examine the potential differences in associations across work and non-workdays. A significant interaction term, where the association between higher activity level and worse cardiovascular load and autonomic function is stronger during workdays versus non-workdays, would be supportive of the proposed mechanism for the physical activity health paradox. Effect sizes (f2) were also calculated for the interaction terms. Steps, LPA and MVPA time were scaled in all models to reflect clinically relevant differences in the associated activities (1000 steps/day, 120 min of LPA and 10 min of MVPA).
All models were adjusted for age, body mass index, smoking status, fitness and the resting value of the outcome of interest (HR, systolic BP or diastolic BP). MVPA and LPA were included in the same model to mutually adjust for each other. All analyses were performed in Stata V.16 (StataCorp) with alpha=0.05.
Using that effect size=0.4 for systolic BP,30 with power=0.80, an alpha=0.05, and a modest within-subject correlation=0.50, it was determined that 18 participants were needed to detect a difference in systolic BP between days. To account for potential incomplete data, we recruited 19 participants.
Results
Table 1 provides baseline sample characteristics (n=19). Table 2 compares 24-hour, waking, nocturnal and non-work cardiovascular load and nocturnal HRV on workdays and non-workdays. Twenty-four hours and waking HR were significantly higher on workdays versus non-workdays with medium effect sizes. Systolic BP did not differ during any time interval between workdays and non-workdays. However, 24-hour, waking and non-work time diastolic BP was significantly higher on workdays versus non-workdays with medium to large effect sizes. Nocturnal diastolic BP was not different across day types. The average nocturnal RR interval, RMSSD, and SDNN were non-significantly lower following workdays versus non-workdays with small effect sizes. Nocturnal LF and HF were significantly lower following workdays versus non-workdays with small effect sizes, though the LF/HF ratio was similar.
Participant characteristics (n=19)
Comparison of cardiovascular load and nocturnal HRV on work and non-workdays (n=19)
Table 3 presents the associations of steps with cardiovascular load. On average, participants had more steps on workdays than non-workdays (12 772 vs 7923 steps, p<0.001). On workdays, greater steps/day were associated with higher 24-hour HR, waking HR and nocturnal HR. Greater steps/day were similarly associated with higher 24-hour HR and waking HR on non-workdays, though not nocturnal HR. Steps/day were not associated with systolic or diastolic BP during any time interval on either day type (p>0.05 for all). No significant interactions in the association between steps per day and cardiovascular load across work versus non-workdays were observed, indicating a similar effect of total volume of activity across work and non-work domains (p>0.05 and small effect sizes for all).
Associations of daily steps and cardiovascular load (n=19)
Table 4 presents the associations of LPA and MVPA minutes/day with cardiovascular load across work and non-workdays. On average, participants had more LPA and MVPA minutes on workdays than non-workdays (391.5 vs 285.2 min and 72.4 vs 41.5 min respectively, p<0.001 for both). Like daily steps, greater LPA was associated with higher 24-hour HR and waking HR on workdays and non-workdays. Additionally, greater LPA was positively associated with 24-hour and waking diastolic BP on workdays but not on non-workdays, however the interaction term was non-significant with a small effect size. On workdays, greater MVPA was significantly associated with higher 24-hour, waking, and nocturnal HR; however, no associations were observed on non-workdays. As such, the workday by HR interaction terms for 24-hour, waking and nocturnal HR were all significant (p<0.05) with small effect sizes. Waking diastolic BP was positively associated with MVPA on non-workdays; however, no other significant associations or interactions were found between MVPA and systolic or diastolic BP across days with all interactions having small to medium effect sizes.
Associations of daily light and moderate-to-vigorous physical activity (LPA/MVPA) minutes with cardiovascular load (n=19)
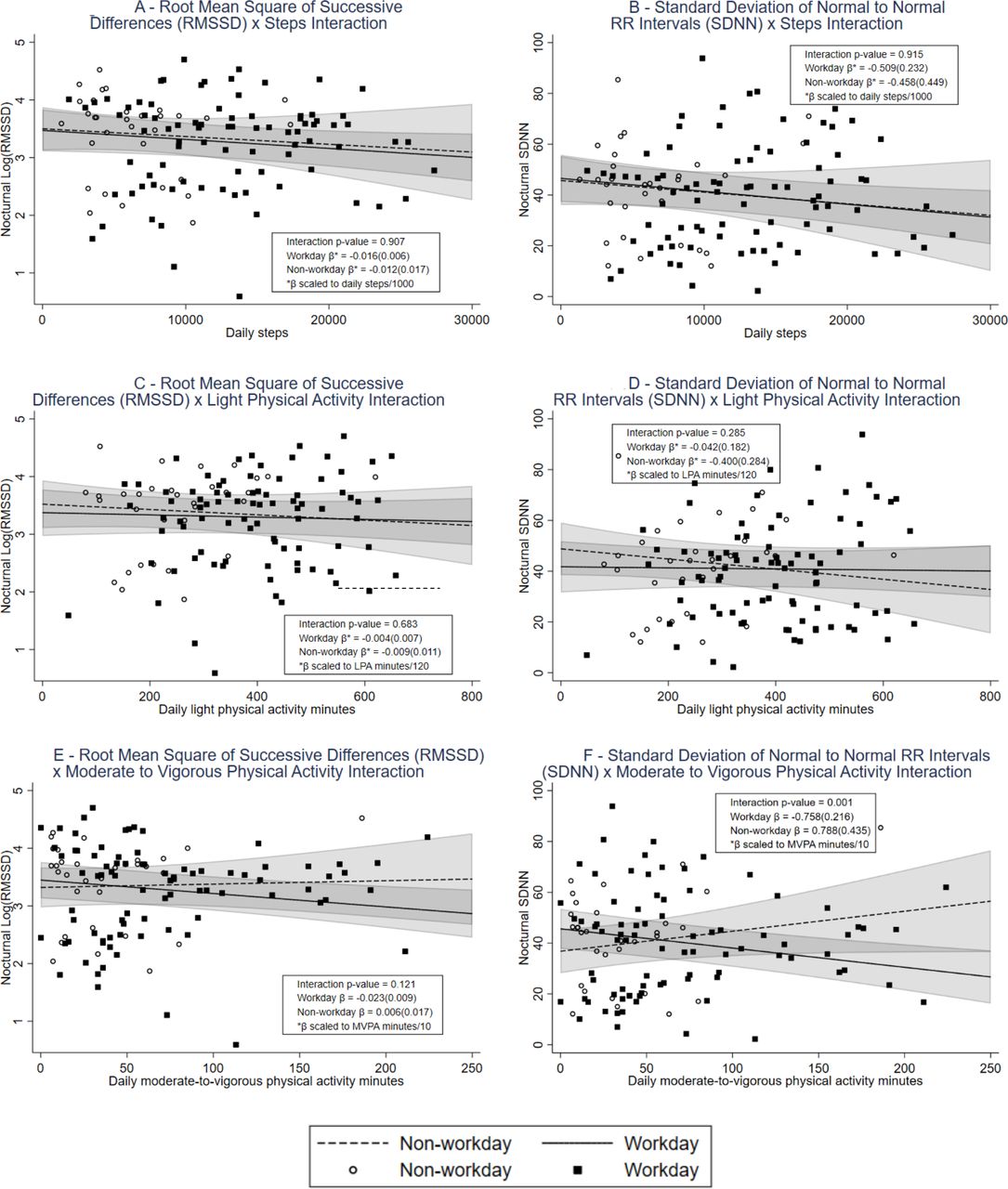
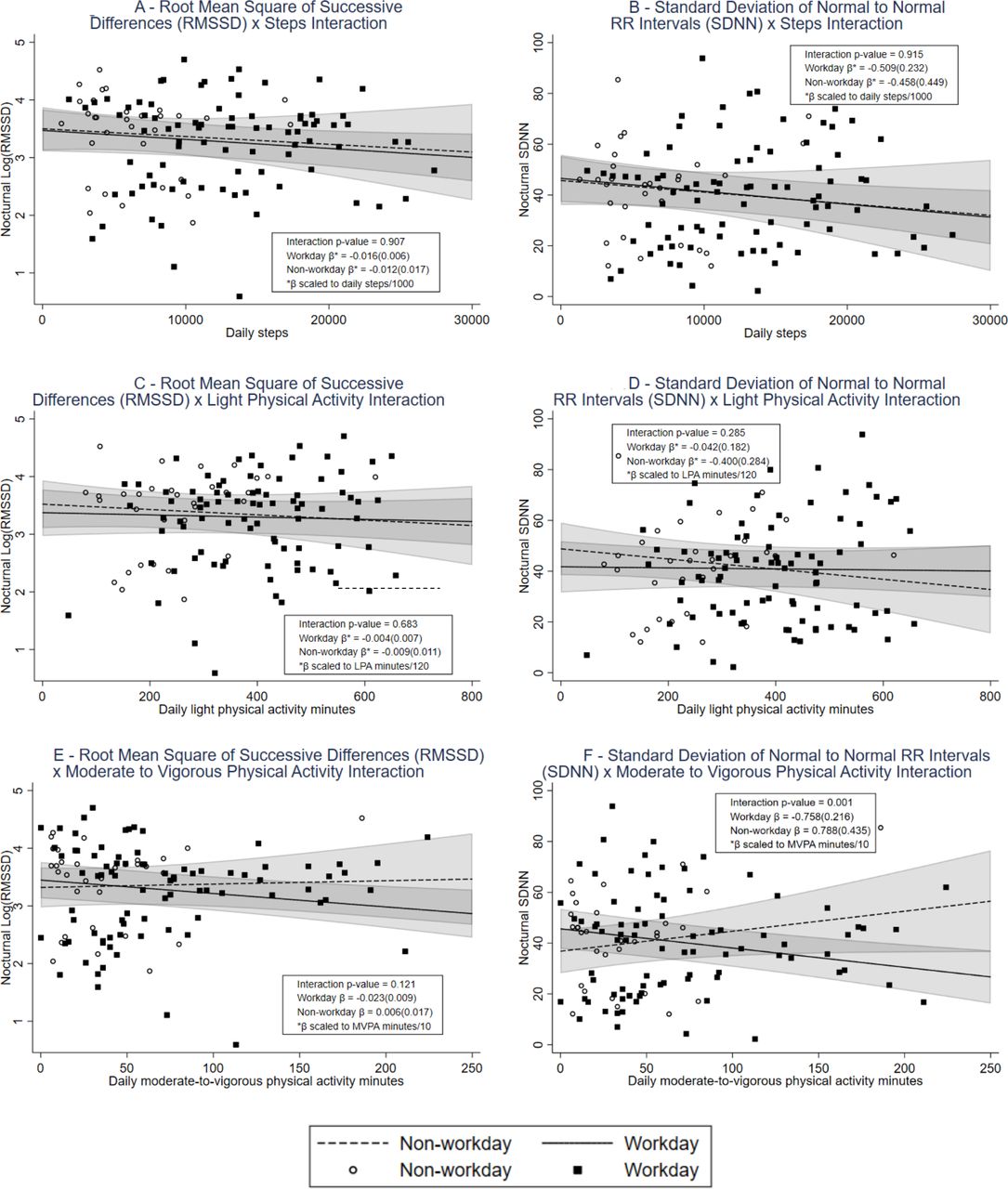
Figure 1 presents the associations and interactions of continuous daily physical activity and nocturnal HRV (RMSSD and SDNN only) by work and non-workday. Online supplemental table 1 provides results for all HRV parameters. On workdays, greater steps were associated with significantly lower nocturnal SDNN, LF and HF HRV, but no associations were found on non-workdays. No significant interactions in the association between steps and HRV were observed between work and non-workdays. No HRV parameters were associated with daily LPA on work or non-workdays and there were no significant interactions. Higher MVPA was negatively associated with RMSSD, SDNN and LF HRV on workdays, whereas non-significant positive associations were found between MVPA and the same HRV parameters on non-workdays. A significant interaction was observed for SDNN across work and non-workdays where the effect of higher MVPA on SDNN was significantly more adverse during the night following a workday.
Supplemental material
{kind=link}
Associations of daily physical activity and nocturnal RMSSD and SDNN following work and non-workdays. LPA, light physical activity; MVPA, moderate-to-vigorous physical activity.
Discussion
This study sought to understand the relationship between OPA and acute cardiovascular load to inform a potential physical activity health paradox. Several findings provide mechanistic data in agreement with the physical activity health paradox hypothesis. Measures of cardiovascular load, including 24-hour and waking HR and BP as well as non-work diastolic BP, were significantly higher on workdays versus non-workdays which could be largely attributed to the higher levels of physical activity on workdays. Additionally, no difference in systolic BP or nocturnal BP or HR was observed. Nocturnal HRV was largely similar across work and non-workdays, although LF and HF were lower (ie, worse) following workdays. Further exploring potential physical activity health paradox mechanisms, we evaluated whether the type of day (work vs non-workday) modified the association between activity and cardiovascular parameters. Greater daily steps and LPA minutes were similarly associated with higher 24-hour and waking time HR on both day types (non-significant interactions). In contrast, greater MVPA was associated with higher HR on workdays and significant MVPA by workday interactions were observed for all HR variables and SDNN HRV. This finding suggests a more unfavourable cardiovascular health effect of MVPA in the context of work versus non-workdays.
Previous research suggests that high amounts of OPA may increase 24-hour cardiovascular load (eg, HR and BP) resulting in chronic cardiovascular strain and, ultimately, cardiovascular damage.7 9 10 This study provides initial evidence, using acute OPA exposure, in support of this mechanistic pathway. It is well established that BP and HR increase during acute exercise, but then subsequently decrease acutely for up to 15 hours afterward.31 Contrary to these expected compensatory responses to aerobic physical activity, a significantly higher diastolic BP was observed during non-work time on workdays compared with non-workdays. Similarly, 24-hour and waking HR and diastolic BP were higher on workdays versus non-workdays. Together, these findings suggest that, if any compensatory effects were observed, they were not sufficient to reduce 24-hour cardiovascular load. Our data indicate that a full workday of OPA is associated with higher 24-hour HR and diastolic BP compared with non-workdays. This suggests that long duration OPA exposure, with less subsequent rest, does appear to be associated with increased 24-hour cardiovascular load. This contrasts with the non-workday effects (ie, with LTPA), though we note LTPA did not occur at the high levels of OPA observed in our sample. It remains unclear whether the high volume of activity, the occupational context, or both are responsible for the adverse cardiovascular responses observed.
A previous study of 182 male workers found that greater amounts of self-reported occupational lifting and carrying was associated with significantly higher 24-hour systolic BP,32 possibly due to sustained isometric contractions.33 These findings agree with ours in that they generally support the physical activity health paradox mechanism, whereby OPA increases 24-hour cardiovascular load. However, because our study used objective measurement of ambulatory activity, we could not identify lifting and carrying specifically, nor explore this line of inquiry. Future studies should examine effects of more comprehensive OPA exposures (walking, lifting, carrying, etc) on ambulatory cardiovascular responses.
The only HRV parameters that differed across work and non-workdays were LF and HF, which were lower on workdays. However, the association between MVPA and HRV differed on work versus non-workdays, whereby there were significant inverse (adverse) associations on workdays and nonsignificant but direct (beneficial) effects on non-workdays. This interaction was statistically significant for SDNN, providing intriguing support for the paradox. Two previous studies have evaluated associations of nocturnal HRV with OPA in blue-collar workers concluding that high OPA volume14 and intensity34 was associated with impaired HRV (LF, RMSSD, SDNN and HF). Agreeing somewhat with those results, we found lower nocturnal HF HRV following workdays compared with non-workdays and a negative association of workday MVPA with nocturnal SDNN, possibly indicating that high OPA results in an adverse cardiac-autonomic response of decreased nocturnal parasympathetic activity.
The observed inverse association between occupational MVPA and HRV responses on nights after working may be due to heightened psychological work stress persisting through the night. Previous literature suggests that psychological work stress may decrease vagal tone thus decreasing resting HRV due to increased catecholamine release.35 Also, high psychological stress has been shown to impair sleep quality, which could be reflected in compromised HRV.36 It is possible that high OPA causes or simply coincides with higher levels of work stress; thus, an effect where high OPA and associated work stress results in lower nocturnal HRV is plausible.
One study measured the effect of acute exercise of various durations on nocturnal HRV and HR, concluding that nocturnal HRV was lower following the longest duration exercise potentially due to delayed recovery of cardiac autonomic modulation during the nocturnal period.37 These results align with the current findings indicating reduced HF and LF as well as elevated HR on workdays (greater OPA) compared with non-workdays. However, the effect differences across activity modalities and intensities must be explored further.
In contrast to the above-discussed MVPA interaction results, no significant interactions were observed for steps/day or LPA for any cardiovascular parameters tested. This result does not align with one hypothesised mechanism,10 where long duration light-intensity OPA increase cardiovascular load without improving fitness. Our findings more strongly support a mechanism where high volumes of occupational MVPA result in cardiovascular strain for which workday recovery is insufficient to compensate.
While the current study only measured acute cardiovascular responses over 1 week and did not consider duration of exposure to OPA, it captured habitual OPA that would likely be similar over longer periods. The current study results indicate that workday OPA exposure may elevate 24-hour HR and BP. This elevation, sustained over time, may lead to vascular damage and potentially increased mortality risk.13 However, previous literature has recognised a 2 mm Hg change in ambulatory BP30 and 5 bpm difference in ambulatory HR38 as clinically meaningful for cardiovascular risk. While statistically significant, the differences in diastolic BP (2.7 mm Hg) and HR (5.4 bpm) observed across work and non-workdays were only slightly above those thresholds and should be further confirmed to imply clinical relevance. Considering these implications, future research investigating effects of chronic OPA exposure on vascular and heart structure and function, and subsequent effects on cardiovascular morbidity and mortality, is warranted.
Strengths and limitations
Several strengths and limitations should be discussed. The within-subject design uniquely accounted for previously uncontrolled confounding that has been a major limitation of previous literature.11 39 However, only acute responses among individuals with high OPA jobs could then be examined. Another strength was the objective physical activity and SED measurement, using gold-standard devices and a diary, to determine the activity domain (work, non-work, sleep).19 While objective activity monitoring provides valid classification of ambulation, posture and movement, future research should work to accurately assess lifting, carrying, and isometric work as well which may influence BP differently.
This study was limited to monitoring only volitional activity in free-living environments. Although workdays were significantly more active than non-workdays and consistent findings were found using continuous activity data, comparing the two day types is still influenced by individual and daily OPA and LTPA variability. Furthermore, while the free-living design did not allow for randomisation of the work and non-workdays, this method increases ecological validity of the measurements. Future research would benefit from more highly controlled activity as well as the use of compositional data analysis methods. Further, the cross-sectional design, observational approach and short-term assessment window did not establish temporality or allow for quantification of cardiovascular load, or health effects potentially associated with chronic OPA exposure, that should be studied in the future. This study was limited by a small sample size. Although repeated measurements would tend to increase statistical power, this study may have been underpowered particularly for the exploratory interaction models. Future studies should confirm these results in larger and more diverse samples. The current study was also limited to healthy males who could safety complete our medically unsupervised fitness test. Thus, findings may not be externally generalisable to large occupational populations. Future studies should include females and individuals with cardiovascular risk factors to increase external validity.
Conclusions
This study provides initial evidence that the 24-hour cardiovascular load on high OPA workdays is significantly higher than on non-workdays. Diastolic BP during non-work time and HR during nocturnal periods remained elevated following workdays compared with non-workdays, suggesting inadequate recovery or reduced parasympathetic activation following OPA. Nocturnal HRV analysis provided preliminary evidence indicative of lower parasympathetic activity following workdays compared with non-workdays and suggest that daily MVPA may be differentially associated with 24-hour cardiovascular load and nocturnal HRV on workdays versus non-workdays. These data support the physical activity health paradox hypothesis.
Further study is necessary to better understand the potential mechanisms explaining the physical activity health paradox. Studies with larger, more diverse samples, using controlled laboratory protocols, with better comparison groups and superior longitudinal methods are needed. However, if the physical activity health paradox is true, as our results preliminarily support, physical activity recommendations may need to consider OPA separately from LTPA due to opposing health implications.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
All study procedures were approved by the University of Pittsburgh Institutional Review Board (STUDY# 19050097).
Acknowledgments
Thank you to all of the participants who volunteered their valuable time to participate in this study and for all of the hard work they do each day.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TDQ, CEK, EN and BBG contributed to analytical design development, analysis and manuscript authorship. LR and AA contributed to critical manuscript review and authorship.
Funding This study was funded School of Education’s Dissertation Research Grant Programme at the University of Pittsburgh.
Disclaimer The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centres for Disease Control and Prevention.
Competing interests BBG discloses grant funding from the Agency for Healthcare Quality Research, the American Heart Association, the National Institutes of Health and the Tomayko Fund.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.