Article Text

Abstract
Objectives We aimed to develop and validate a prediction model for the duration of sickness absence (SA) spells due to back pain (International Statistical Classification of Diseases and Related Health Problems 10th Revision: M54), using Swedish nationwide register microdata.
Methods Information on all new SA spells >14 days from 1 January 2010 to 30 June 2012 and on possible predictors were obtained. The duration of SA was predicted by using piecewise constant hazard models. Nine predictors were selected for the final model based on a priori decision and log-likelihood loss. The final model was estimated in a random sample of 70% of the SA spells and later validated in the remaining 30%.
Results Overall, 64 048 SA spells due to back pain were identified during the 2.5 years; 74% lasted ≤90 days, and 9% >365 days. The predictors included in the final model were age, sex, geographical region, employment status, multimorbidity, SA extent at the start of the spell, initiation of SA spell in primary healthcare and number of SA days and specialised outpatient healthcare visits from the preceding year. The overall c-statistic (0.547, 95% CI 0.542 to 0.552) suggested a low discriminatory capacity at the individual level. The c-statistic was 0.643 (95% CI 0.634 to 0.652) to predict >90 days spells, 0.686 (95% CI 0.676 to 0.697) to predict >180 spells and 0.753 (95% CI 0.740 to 0.766) to predict >365 days spells.
Conclusions The model discriminates SA spells >365 days from shorter SA spells with good discriminatory accuracy.
- epidemiology
- occupational health practice
- public health
- sickness absence
- risk assessment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Predictors of sickness absence (SA) for back pain are well-known, but the previous studies have not focused on prediction of the duration of SA spells due to back pain.
What are the new findings?
This study developed and validated a clinically implementable, pragmatic prediction model for the duration of SA spells >14 days due to back pain (M54) for the whole working-age population in Sweden.
The model discriminates the long-term SA spells (>365 days) from shorter SA spells with good discriminatory accuracy.
How might this impact on policy or clinical practice in the foreseeable future?
The prediction model can be applied in Sweden, and perhaps have applicability to other Nordic countries with similar welfare systems for social insurance.
The results of this work are currently implemented in pilot tests in primary healthcare settings to help general practitioners to identify which of their sickness absent patients have high risk for long-term sickness absence.
Introduction
Sickness absence (SA) due to poor health is a major public health problem.1–3 Musculoskeletal diagnoses (MSD) account for most of the SA spells in Europe, although SA due to mental disorders is growing.4 5 The costs of SA due to MSD incurred by individuals, employers and the society at large are high.1 2 Studies showed that low back pain, although not life-threatening, is a top contributing factor to the burden of MSD.6 Back pain is also a common reason for seeing a physician.7 8 So far, however, no consensus has been reached on prognosis and management of low back pain.9 Instead, many clinical practice guidelines for treatment and care of low back pain have been proposed.10 Regarding work incapacity, predictors of SA for back pain are well-known.11 12 The previous studies, however, have not focused on prediction of the duration of SA spells due to back pain.13 Effective prediction methods for the duration of SA spells due to low back pain can improve possibilities to identify patients at risk of long-term SA.
Several studies have developed and validated decision support tools to predict future work incapacity, whether ending in SA or not, in general or related to specific diagnoses.14–18 Most of these studies were limited by low sample sizes,19 20 specific study populations,17 19 short follow-up periods17 21 or lack of information on SA diagnosis.17–19 The grounds for the selection of predictors in those prediction models have varied from using theoretical frameworks, that is, the job-demand-control model,17 mathematical modelling of survey data,14 to selection based on literature.19 Only one previous study developed a model to predict duration of SA among those already on SA—with focus on SA due to stress-related diagnoses.22 Such prediction models are needed, especially in primary healthcare where such consultations are common among general practitioners.23 24 In this study, we developed and validated a prediction model for the duration of SA spells due to back pain with population data from Swedish nationwide registers.
Methods
A prospective cohort study using register microdata was conducted including all new 64 048 SA spells in Sweden >14 days that were initiated in the 2.5-year period of 1 January 2010 to 20 June 2012 with an International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) diagnosis code ‘M54’, that is, dorsalgia/back pain.25
Register linkage
The SA spells were identified by use of the Swedish Social Insurance Agency’s Micro Data for Analysis of the Social Insurance (MiDAS) register, including information on all SA spells with benefits from the Agency. Information from MiDAS (dates, diagnoses and extent of SA and disability pension (DP) and employment status when the SA spell begun) was linked with the following four nationwide registers at individual level by the use of the unique personal identity number of all residents in Sweden26:
The Longitudinal Integration Database for Health Insurance and Labour Market Studies (Swedish abbreviation LISA) from Statistics Sweden, regarding information on sociodemographic factors (age, sex, country of birth, educational level, occupational sector, marital status, family composition, emigration year, geographical area and type of living area for the calendar year preceding the start date of the index SA spell).27
From the National Board of Health and Welfare three registers were used regarding information for 2009–2012; the Swedish inpatient and specialised outpatient registers28 (dates and diagnoses of inpatient and specialised outpatient healthcare); the Prescribed Drug register29 (dates and the Anatomical Therapeutic Chemical (ATC) codes for dispensed prescribed drugs); and the Cause of Death register (dates of deaths).30
Social insurance system in Sweden
In Sweden, all residents aged 16 years or above, with an income from work or unemployment benefits are eligible for SA benefits, if the work capacity of the individual is reduced because of a disease or an injury.4 For most employed, the first 14 days of a SA spell are reimbursed by the employer, otherwise from the Social Insurance Agency. From day 8, a sickness certificate from a physician is required. For individuals aged 19–64 years, DP can be granted, if their work capacity is long-term or permanently reduced because of a disease or an injury. Both SA and DP can be granted for 100%, 75%, 50% or 25% of ordinary working hours. This means that people on part-time DP, for example, for 25%, at the same time can have a part-time SA spell.
Information on SA spells
The duration of each SA spell was calculated from the first until the last day of the SA spell, except when it ended with DP. In this case, the duration of the spell was set to 1000 days (n=1613). SA spells >1000 days were fixed at 1000 days (n=148) to control for extreme outliers in our analysis as has been done before.22
Predictors
A decision was made that for clinical implementation a maximum of nine variables could be included in the model—it was assumed that more variables would take too much time for the general practitioner to include in the algorithm during the consultation. Of these, three were to be included as they were routinely collected information in the medical records (sex, age, and geographical area) and the other six which were simple enough for the certifying physician to ask the patient about. Initially, the number of possible predictors was very large (130) as has been described in detail earlier.22 31 32 Many of these predictors were redundant or partially redundant and/or highly collinear as shown in an earlier study based on the same data sources.22
There were very few missing values for the different possible predictors. Those with missing information on country of birth (0.05% of the SA spells) were coded as ‘non-EU country’ and missing information on educational level (0.3% of the SA spells) were coded as education at elementary level. As described earlier,22 several analyses were conducted with the different variables, to check the predictive value, especially comparing hierarchically related variables referring to specific diagnoses versus their non-diagnosis specific pair. The general variable performed at least as well, but often better than the specific variable. Hence, the general variables were kept for further analyses. The general variables had also an advantage because they could facilitate implementation of the model in clinical settings, as information for its application was to be provided by the patient during the consultation. Last, no difference in predictive value existed if the number of previous SA days were counted during 1–365 days or the 366–730 days period before the start date of the index SA spell. That was also the case regarding hospitalisation and specialised outpatient visits in the two different previous years. Therefore, we choose the most recent period to facilitate the implementation of the model. Furthermore, recall bias, when using information from the patient, was also likely to be smaller if only the recent year had to be considered. Hence, this selection process resulted 14 variables, which were independent predictors for the duration of the SA spell. They are listed below:
Possible predictors regarding the day when the SA spell started:
Age: grouped as 18–34, 35–40, 42–50, 51–57 and 58–64 years.
Sex: woman, man.
Geographical regions: Northern, Middle, Western and Southern Sweden, and Stockholm/Gotland.
Country of birth: Sweden, other Nordic, other EU25 and rest of the word.
Family composition was described with a four-categories composite variable constrained from the following possible situations: living with or without a partner and living with or without children (aged <18 years).
Educational level: categorised as elementary (≤9 years), high school (10–12 years) and university/college (>12 years).
Employment status: in paid work, on unemployment benefit or at parental leave or student benefit.
SA extent: 25%, 50%, 75% or full-time (100%).
Partial DP: yes, no.
Whether the SA spell was initiated in primary healthcare or not was assessed by having had any inpatient or specialised outpatient healthcare during the period of 4 days before and 8 days after the start of the SA spell and categorised as ‘yes’ or ‘no’.
Possible predictors based on the 365 days preceding the start date of the SA spell:
The number of SA days: 0, 1–90, 91–180 or >180 days.
The number of days spent in inpatient healthcare: 0, 1–2 or >2 days.
The number of specialised outpatient visits: 0, 1–2 or >2 visits.
Multimorbidity was defined, based on dispensed prescribed medication. At least one purchase for a minimum of three different ATC groups were considered as having multimorbidity.
Information about all these items was assumed to be easily retrieved during a patient-physician consultation. To achieve the a priori decided three routinely available and six patient-physician question predictors for the model, we selected the 6 variables with the highest predictive values to the final model from this set of 14 variables through additional analyses.
Statistical analysis
The dataset was randomly split into a training dataset (70% of the SA spells) for model development and a validation dataset (30% of the SA spells) for external validation as has been done before.22 Descriptive statistics are presented in table 1 for the characteristics of the SA spells due to back pain and for the distribution of the predictors in the training and the validation dataset. The duration of the SA spells was used as outcome in the analyses. Piecewise constant hazards regression models were fitted with 20 time intervals of empirical quantiles to predict the duration of the SA spells (see online supplementary tables 1-2).
Supplemental material
Characteristics of all the new sickness absence (SA) spells due to back pain (M54) >14 days during a 2.5-year period
As mentioned above, to facilitate implementation to clinical practice, three routinely available predictors, that is, age, sex and geographical region, were included in the model. Further predictors were selected based on the loss of the log-likelihood when they were removed one-by-one from the full model. Those six that resulted in the largest decreases in the log-likelihood were included in the final model, beside the three preselected predictors. Both Akaike information criterion (AIC) and Bayesian information criterion (BIC) were used to compare the goodness-of-fit of the final model to the full model.
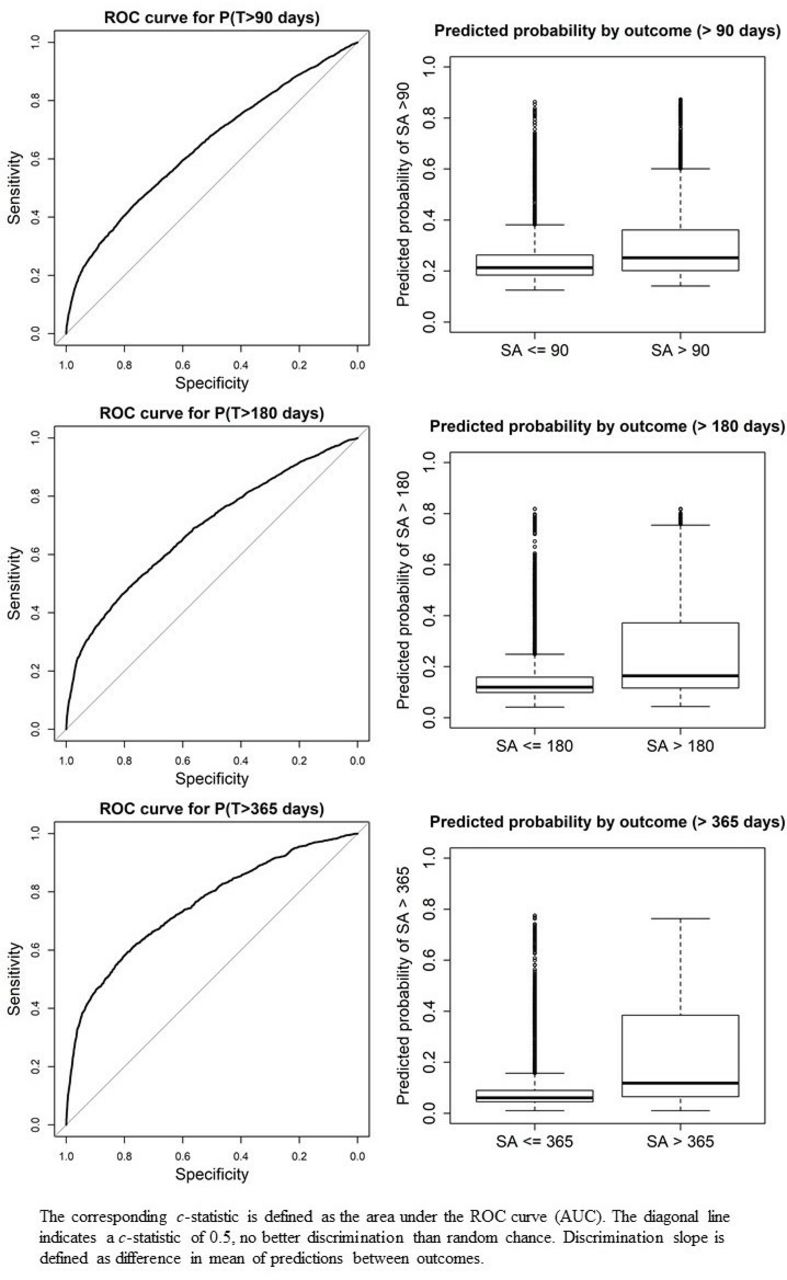
Quantile-quantile plot of the survival probabilities at observed time of event T were used for calibration. The quantiles of the predicted probability that an SA will be longer than its observed length P(T>T_obs) was compared with the quantiles of a uniform distribution to visually test the hypothesis that P(T>T_obs) is uniformly distributed, that is, quantile-quantile plots were used to assess if the model is correctly specified. The overall discriminatory capacity was assessed using the c-statistic.33 34 The CIs for the overall c-statistics were obtained by using bootstrap resampling (n=1000). The observed versus predicted survival probabilities at predefined SA durations (90, 180 and 365) were plotted. Receiver operating characteristics (ROC) curves and their corresponding c-statistics with 95% CI, calculated by the DeLong approach,35 were used to evaluate discriminatory accuracy for predicting duration >90, >180 and >365 days, respectively.
R V.3.4.336 was used for statistical analysis and graphics (packages ‘pch’. ‘pROC’, ‘e1071’. ‘Hmisc’, ‘ggplot2’ and ‘pch’),37 and SAS V.9.4 for the data management.
Results
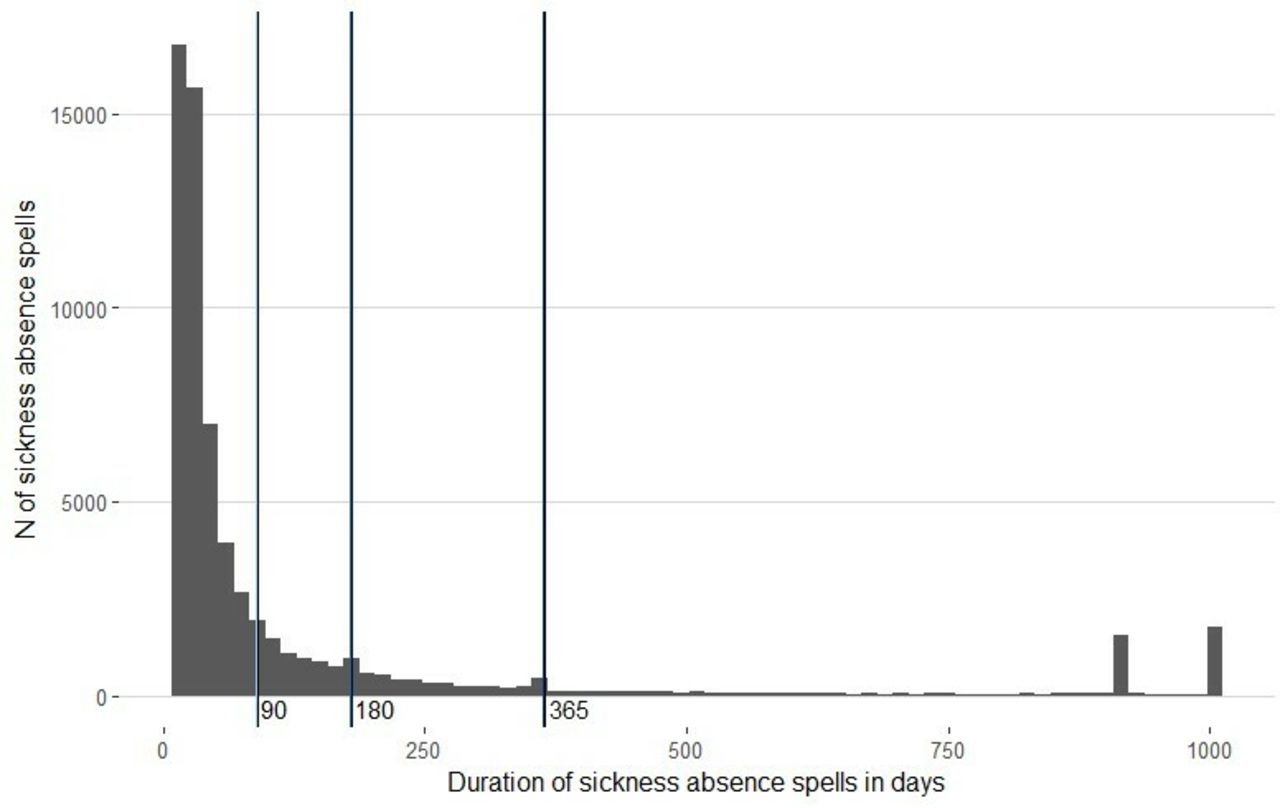
Characteristics of the 64 048 SA spells are shown in table 1. Overall, 73.5% of the spells lasted ≤90 days, while 9.2% (n=5883) became >365 days (table 1 and figure 1). The median duration of the SA spells was 37 days (the IQR 22–98 days). Most of the spells (96.7%) ended due to return to work or to other activity (eg, studies or parental leave), while 2.6% of the SA spells continued as DP (table 1).

Histogram of the distribution of the sickness absence (SA) spells. Vertical lines indicate the cut-off at duration of 90, 180 and 365 days.
The distribution of the baseline predictors is presented in table 2. Employment status, multimorbidity, SA extent at the start of the spell, whether the SA spell was initialised in primary healthcare as well as the gross number of SA days and number of specialised outpatient clinic visits during the 365 days preceding the start date of the SA spell, were the six selected predictors that had the largest log-likelihoods loss, and therefore were included in the final model together with the three routinely available variables: age, sex, and geographical region (table 3).
Tabulation of possible baseline predictors for the training and test data
Decrease in likelihood of the 14 predictors of the duration of SA spells due to M54
Both the AIC (453 078 vs 453 089) and BIC (458 664 vs 456 737) were lower for the final compared with the full model. The log-likelihood was only slightly higher for the final than for the full model (−226 119 and −225 904 with 420 and 640 free parameters, respectively). The probability integral transform value of the model was basically uniform, indicating a good calibration and specification of the final model. The overall c-statistic was rather low, 0.547 (95% CI 0.542 to 0.552) suggesting a low discriminatory capacity at the individual level. Binary predictions of risk of SA duration showed reasonable performance for SA spells >90, >180 days, and good performance for SA spells >356 days. The c-statistics were 0.643 (95% CI 0.634 to 0.652), 0.686 (95% CI 0.676 to 0.697) and 0.753 (95% CI 0.740 to 0.766), respectively (figure 2).
{kind=link}
{kind=link}
Receiver operating characteristics (ROC) curves and box plots of predicting duration of sickness absence (SA) for outcomes of >90, >180 and >365 days.
Discussion
We developed and validated a prediction model for the duration of SA spells >14 days due to back pain (M54) to be easily implementable in primary healthcare. Analyses were based on all SA spells due to M54 in Sweden during a period of 2.5 years. Age, sex, geographical region, employment status, multimorbidity, SA extent at the start of the spell, whether the SA was initialised in primary healthcare settings as well as the number of SA days and visits in specialised outpatient healthcare during the preceding year were included into the final model as predictors. The overall discriminatory capacity to predict SA duration at an individual level was poor, but the prediction model was good at discriminating SA>365 days from shorter SA spells.
To the best of our knowledge, this is the first time that a prediction model has been developed to predict the duration of SA spells due to back pain. To be able to predict the risk that an ongoing SA spell due to back pain will be long, is an issue of great clinical importance, especially in primary healthcare. To date, to the best of our knowledge, the previous two studies using prediction models instead aimed at predicting which people, among those yet not on SA, will become long-term sickness absent due to back pain or due to any diagnoses,19 38 hence not being comparable to this study with prediction of duration of SA spells.
Several studies have identified previous (long-term) SA as a strong risk factor for future SA17–19; we also found this to be a predictor and included it in our model. We also accounted for other factors such as age, sex, educational level and family composition based on their well-known importance for SA.19 32 As our major aim was to develop a minimalistic model that is easily implementable in primary healthcare settings with a reasonable model performance, we tested many predictors available in the registers and those which were used in the final model were such that they could be assessed with great accuracy during the short time of a patient-physician consultation. Our model predicted long-term SA spells, that is, >365 days with good discriminatory accuracy, which may be useful to identify the patients on SA due to back pain who are at high risk of long-term SA or even DP, in order to take preventive actions.
The duration of SA spells is an extremely complex phenomenon, influenced by many factors at different structural levels, especially SA spells due to back pain.32 One can argue that if prediction of SA duration would be easy, a model would have been developed long ago. This model is a first step and we hope others will use other types of data to pursue development of such models.
The major strength of our work was its population-based design with a full coverage from nationwide registers,39 as all SA spells >14 days that had been initialised in Sweden during the 2.5 years could be included in the study. Moreover, the use of high-quality register-based information26 28 40 (not self-reports) on the possible predictors, no dropouts, the complete and very large study group, meant that our data were not hampered by recall bias or selection bias and made it possible to validate our model for the whole population. However, it also limited our possibility to include some predictors that have been shown to be of importance for occurrence of SA but which are usually obtained through surveys, such as: self-rated health, sleep problems, body mass index, smoking or social support.17 18 Other studies might be able to investigate if such factors can increase the discriminative capacity of the model.
Another limitation of the study is that MiDAS includes only the main SA diagnosis of each SA spell, that is, we had no information on whether the physician assessed also other diagnoses to have contributed to the work incapacity. However, we were able to include information on multimorbidity based on dispensed prescribed medication and we included at least one purchase for a minimum of three different ATC groups; the number that had the highest predictive value. In the preliminary analyses, we also included information on multimorbidity from diagnosis-specific previous SA, DP, hospitalisation and specialised outpatient visits, however, information on dispensed prescribed medication contributed more to the model. Also, our results concern SA spells initiated in 2010–2012, and the predictive models need to be updated to examine possible needs of changing predictors when new data are available.
Furthermore, SA diagnosis was only registered at a 3-digit level for the diagnosis code (ICD-10) in MiDAS. As M54 is a large diagnosis group varying from unspecified pain conditions to inflammations and from radiculopathies to sciatica, information at a 4-digit level might have led to a possibility to make better predictions.
Our model was internally validated under the conditions applying to the Swedish healthcare and social insurance system, and therefore, can be applied in Sweden, and perhaps have applicability to other Nordic countries with similar systems. However, further research is needed to assess the performance in other social insurance settings as generalisability might be low in countries with different welfare systems and lower employment frequency than in the Nordic countries. The results of this work are currently implemented in pilot tests in primary healthcare settings to help general practitioners to identify which of their sickness absent patients have high risk for long-term SA.
Conclusions
We developed and validated a clinically implementable, pragmatic prediction model for the duration of SA spells >14 days due to back pain for the whole working-age population in Sweden. The model discriminates the long-term SA spells (>365 days) from shorter SA spells with good discriminatory accuracy.
References
Footnotes
Twitter @anninarop
Contributors KA and EF contributed to the study conception and design. Material preparation, data collection and analysis were performed by KA, EF, KG, GA, MB and PF. The first draft of the manuscript was written by AR and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding This work was financially supported by the Swedish Social Insurance Agency and the Swedish Research Council for Health, Working Life and Welfare.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The project was approved (2007/5:6, 2009/23–32, 2009/1927–32, 2011/806–32) by the Regional Ethical Review Board of Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.