Article Text

Statistics from Altmetric.com
We welcome the editorial by Thurston highlighting the effects of air pollution on health.1 Air pollution has been shown to have an important effect on the mortality of those with pre-existing respiratory and cardiovascular conditions.2
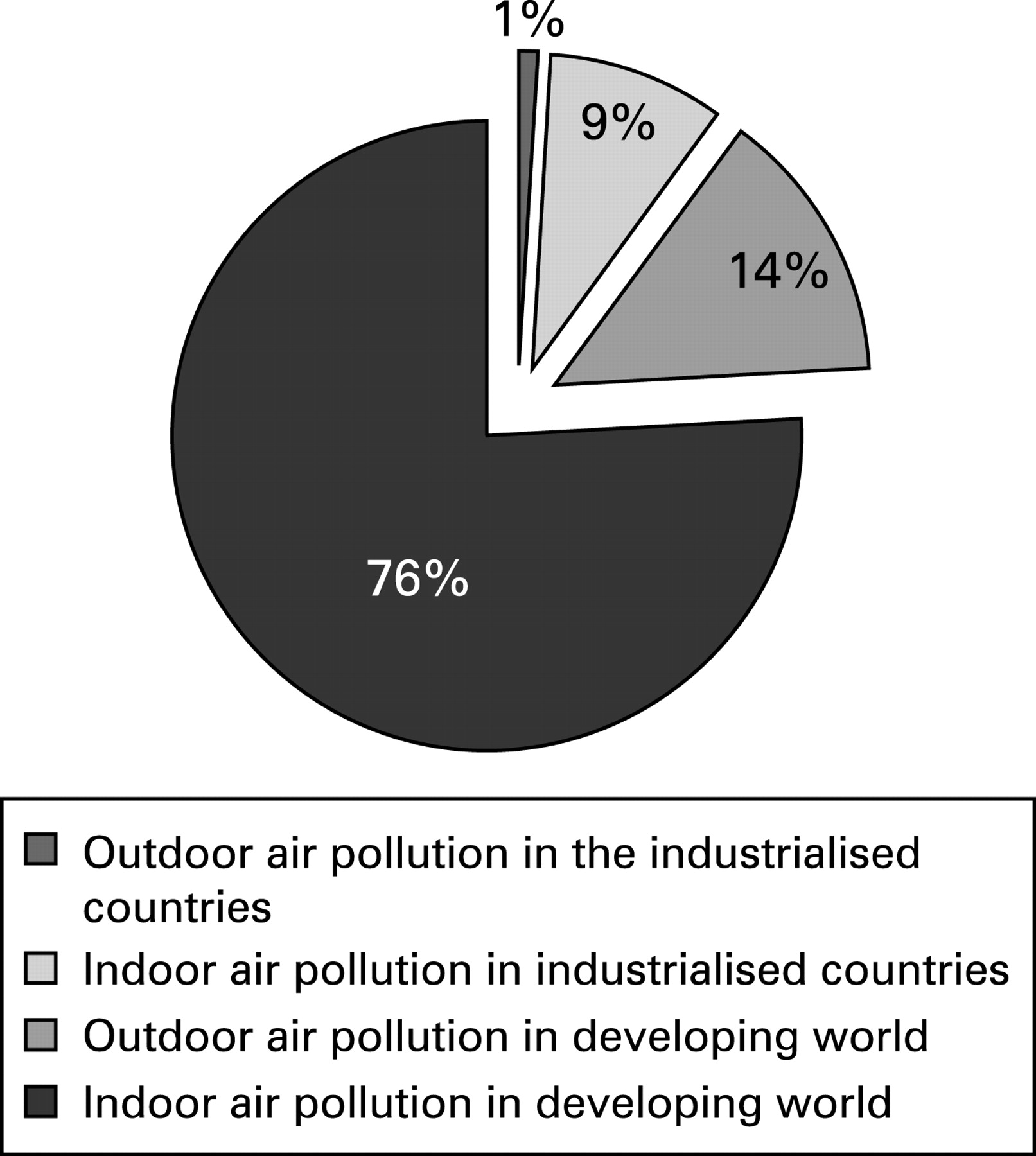
Outdoor sources of air pollution are important contributors to indoor air pollution concentrations, particularly in developed countries. However, global human exposure to particulate matter (PM)—in terms of the number of people, exposure intensity and time spent exposed in various microenvironments—varies greatly in different parts of the world. In industrialised countries, only 1% of global PM exposure occurs in outdoor environments with a further 9% occurring indoors (fig 1). In the developing world, 14% occurs outdoors while 76% of human exposure to PM occurs in indoor environments.3

{kind=link}
As a result of energy poverty, almost one-half of the world population burns organic material such as wood, dung or charcoal for household cooking, heating and lighting. This form of energy is associated with very high levels of indoor PM concentrations (perhaps 2–3 orders of magnitude higher than those found outdoors) and an increased incidence of acute lower respiratory infections, tuberculosis and chronic obstructive pulmonary disease. Women and children, who spend much of their time indoors cooking and preparing food, are disproportionately affected by indoor air pollution.4 The World Health Organization lists indoor air pollution from burning solid fuels as one of the top 10 global health risks, responsible for 1.6 million premature deaths per year, 2.7% of the global burden of disease and an annual loss of over 38.5 million disability-adjusted life-years.5 Compare this with the 800 000 deaths and 4.6 million lost life-years resulting from outdoor air pollution cited in Thurston’s editorial.
Thurston is correct to call scientists and physicians to act on climate change and health. Industrialised countries currently top the table of carbon dioxide emissions per capita (with the USA ranked first and the UK ranked eighth).6 Paradoxically, however, they suffer least from the effects of polluted air. Therefore, while it is important to investigate the effects of outdoor air quality on health, we think that there is a clear and urgent need to expend at least as much effort on attempting to understand and control indoor air pollution in the developing world.
Linked Articles
- Letters