Article Text

Statistics from Altmetric.com
The proportion of intervention studies in occupational epidemiology has been growing rapidly in recent years. This is a positive trend, which makes it necessary to discuss a number of theoretical, methodological, and practical issues. The aim of this paper is to summarise the specific features of occupational intervention research, to suggest solutions to some of the special problems, and to propose ways of developing worksite intervention studies in the future.
Occupational intervention studies are in this paper defined as “studies in which the effects of planned activities at the worksites with the aim of improving the working conditions and/or the health of the workers are being evaluated with research methods”. The goals of these activities are usually improved health and wellbeing of the workers, reduced absence or turnover, or increased motivation and job satisfaction. In some cases these goals are combined with other objectives such as increased product quality, increased productivity, or increased customer satisfaction.
The present article will focus on interventions with a behavioural, organisational, or psychosocial element. This leaves out purely engineering interventions where, for example, one chemical is substituted with another or one machine with another without changes in employee behaviour. The scope of the article is still very broad since it includes such diverse fields as ergonomics, accidents, psychosocial factors, health promotion, physical and chemical factors, and secondary prevention of occupational diseases and injuries.
WHY INTERVENTION STUDIES?
Why is occupational intervention research so important? The simple answer is that we want to know whether or not interventions at the worksites have the desired effect. This is by no means a matter of course. Some interventions have no effects while others have negative effects in spite of the good intentions of everyone involved.
Going one step further, we can identify at least four good reasons for doing intervention research:
-
Intervention studies are usually considered to be more conclusive regarding causality than observational studies. Many textbooks go as far as stating that only interventional research (and in particular: the randomised controlled trial, RCT) can establish causality. In this connection it is important to notice that intervention studies also provide good evidence on negative causal effects.
-
Intervention studies are important for studying the implementation of worksite changes: How, to what extent, and under which conditions is it possible to improve working conditions?
-
If intervention studies are successful, the results are usually much more convincing than results from observational research. Such studies not only show that it is possible to improve working conditions but also that such improvements have the desired effect. The power of the practical example makes it much easier to disseminate research results to the worksites.
-
Finally, intervention research necessitates a close collaboration between researchers and workplaces. This leads to learning on both sides and hopefully also to improved understanding and communication.
WHAT ARE THE MAIN PROBLEMS AND CHALLENGES IN INTERVENTION STUDIES?
The randomised controlled trial
The RCT is the basic methodological paradigm for intervention research. A model of a typical RCT is shown in fig 1. The RCT has a number of features worth noticing before we proceed to the problems of practical occupational intervention research. These features will be presented briefly below, without touching on the important aspects regarding ethics and psychological issues. At this point we stick to the purely methodological principles:
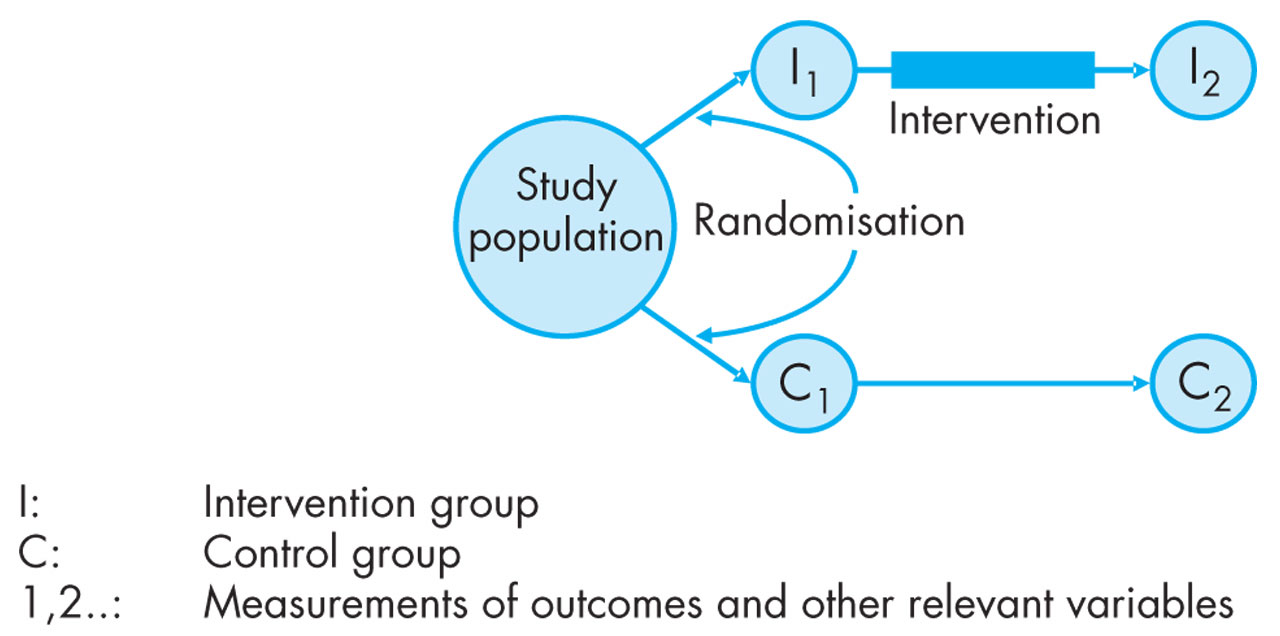
Model of the randomised controlled trial.
The first feature is randomisation. Randomisation can be done in several ways, but the guiding principle is that only chance should determine whether a person (or a worksite) is placed in the intervention or the control group. Randomisation is performed for two reasons: (1) to avoid confounding; (2) to avoid selection bias. Once an intervention study is biased because of some form of differential selection into the intervention and control groups it is impossible to adjust for this source of error in a satisfactory way.
The second feature is the control group. The control group is established in order to make it possible to distinguish between change and effect. This distinction is a parallel to the basic distinction in science between association and causality. In intervention research we are interested in the specific effect(s) of the planned intervention. By definition, the effect is the difference between what happened in the intervention group and what would have happened without the intervention. Our problem is that we cannot repeat history in order to find out what would have happened. This is why we need the control group. The control group is a “stand in” for the intervention group, and the purpose of having it is to find out what would have happened.
The third feature is the prospective design with at least one measurement before the intervention and (at least) one after. The prospective design is necessary since we are—by definition—studying changes over time. By comparing the difference in change in the intervention and control group we get an estimate of the effect, and we can only talk about effect if we are sure that the intervention (cause) comes before the effect.
The fourth feature is the intervention itself. It should be administered to the intervention group and to this group only. It sounds easy but in fact a myriad of problems are buried here. In biomedicine the term compliance refers to the degree to which members of the intervention group actually take the pills they are supposed to take (while the members of the control group do not). In medicine this is a big problem, especially in trials with long intervention periods. In occupational research the interventions are much more complicated and difficult to standardise than a pill. It is no exaggeration to say that this is one of the very large challenges of occupational intervention studies.
The final features are blinding and the use of placebo treatment. In the perfect trial the participants do not know which group they belong to. Also, the researchers and other relevant persons should be blinded (in which case one talks about double blind trials). Blinding is important because it reduces information bias from the persons involved in the RCT, and placebo is important because the effect of the specific treatment should be distinguished from the effect of “being under (any) treatment”. It should be noted that blinding and the use of placebo are not core elements of the RCT. These features have special relevance for biomedical research.
Hopefully, it should be clear by now that all these basic features of the RCT serve important purposes. Still, only few occupational intervention studies are able to live up to the criteria of the RCT.1,2–10w1–25 In articles on intervention studies many authors explain in great detail why it was not possible for them to live up to the standards of the RCT. The problem is that many researchers seem to think that since there are good reasons for not performing an RCT, they do not have to worry about the problems evolving from the use of an imperfect design. The position of this paper is the opposite: There may be many good reasons for not performing a randomised controlled trial in an occupational setting. But there are no good reasons for ignoring the problems created by not applying such a design. In the following I will discuss some of the ways in which we can do high quality intervention studies without using the full model of the RCT.
The present state in occupational intervention research
In their review from 1994, Goldenhar and Schulte3 evaluated the methodological quality of occupational intervention studies. They found a number of problems common to most of the studies published at that time: (1) There were no criteria regarding adequate intervention duration, frequency, or intensity. (2) There was too little focus on the intervention process itself. (3) There was little attention paid to the selection of samples, and very rarely were statistical power calculations performed. (4) Most studies had no clear theoretical basis. The researchers seemed to rely on their own intuition and experience. (5) Often there was no control group, and randomisation was extremely rare. Other authors have agreed with Goldenhar and Schulte and added two further points to the list: (6) The follow up time is often arbitrary and almost always too short. (7) Statistical analyses are often inadequate.
It might be argued that researchers always want higher quality research—at least from other researchers. This may be true, but there are many examples showing that quality does matter. In their review of worksite health promotion programmes, Heany and Goetzel4 stratified 35 programmes according to study design. Among the best studies (randomisation and control group), 22% were “encouraging”. Among studies with control group but without randomisation, 56% were “encouraging”. And finally, among studies with low quality (no control group, only pre-post comparisons), 100% were “encouraging”. This result clearly suggests that poor study designs with low internal validity can hide poor intervention effects.
Since 1994, the number of occupational intervention studies has increased dramatically and the overall quality has improved. We also have a number of splendid reviews and guidelines in which the basic methodological principles for intervention studies are explained and discussed.1,2–10 In the following I will not repeat what has already been said in these papers, but focus on the intervention process from the implementation of the intervention via the changes of exposure or behaviour to the health related outcome. For brevity I will use the term “exposure” for both workplace exposures and health related behaviours (such as lifting technique or the use of safety equipment).
The steps in the intervention process
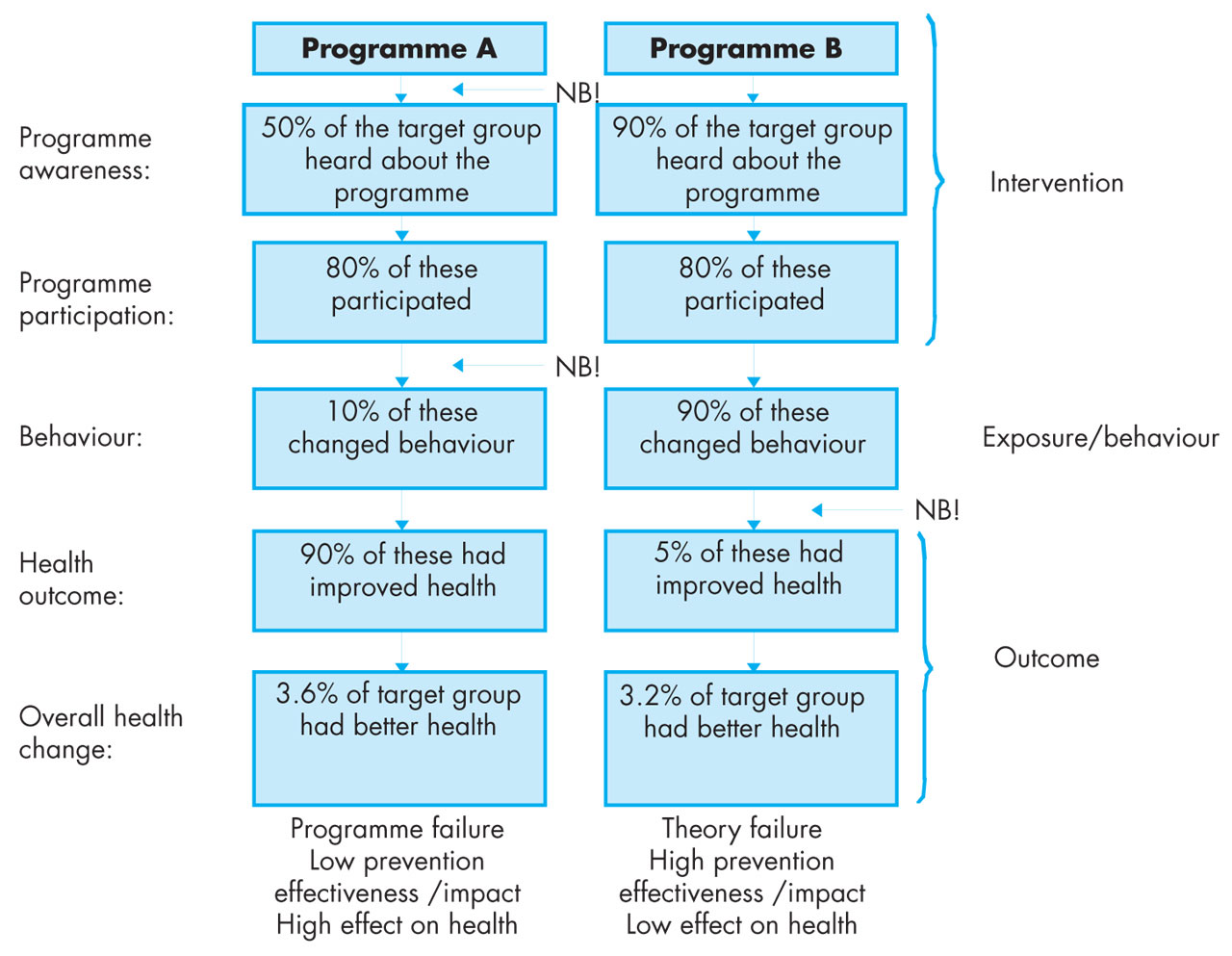
Figure 2 shows “the full model” for occupational intervention studies. To the left we have the theoretical model for the intervention: the intervention is expected to lead to reduced exposure, which is expected to lead to better health. To the right we have the actual course of events in practice. At all three levels the actual events may differ from the intended. In the middle of the model we have the empirical research aiming at measuring all three sets of factors in valid ways. The vertical arrows indicate the connections between intervention, exposure, and health. The horizontal arrows indicate validity: Do we measure what we intend to measure, and do we measure what actually happens? The model in fig 2 is a simple linear model with one way arrows. In real life situations there may be many feedback loops going from the exposure level back to the intervention and from health back to the previous two levels. Such feedback loops should clearly be included in the description and evaluation of the intervention process.

Theoretical model of key elements in occupational intervention studies.
The first research question indicated by this model is whether or not the intervention was carried out as intended. Did people attend the course, hear about the campaign, work according to the new division of labour, or use the new equipment as intended? Of course, this question assumes that there is a well described plan for the intended intervention. Such a plan is a prerequisite for internal as well as external validity. It is often impossible to include detailed descriptions of interventions and intervention processes in research articles. A solution is to publish such material on the internet.
The second question is the issue of impact or prevention effectiveness: Did the intervention lead to the intended changes in exposure? In laboratory research “intervention” and “change of exposure” is the same, since the researcher is by definition in control of the exposure. This is usually not the case in field studies, which makes it necessary to study this issue separately.
Table 1 shows some examples of interventions and intended changes in exposure. It is immediately clear that the intended positive changes may not take place. Whether or not this happens is an important research question, which is often ignored.
Examples of interventions and intended changes in exposure/behaviour
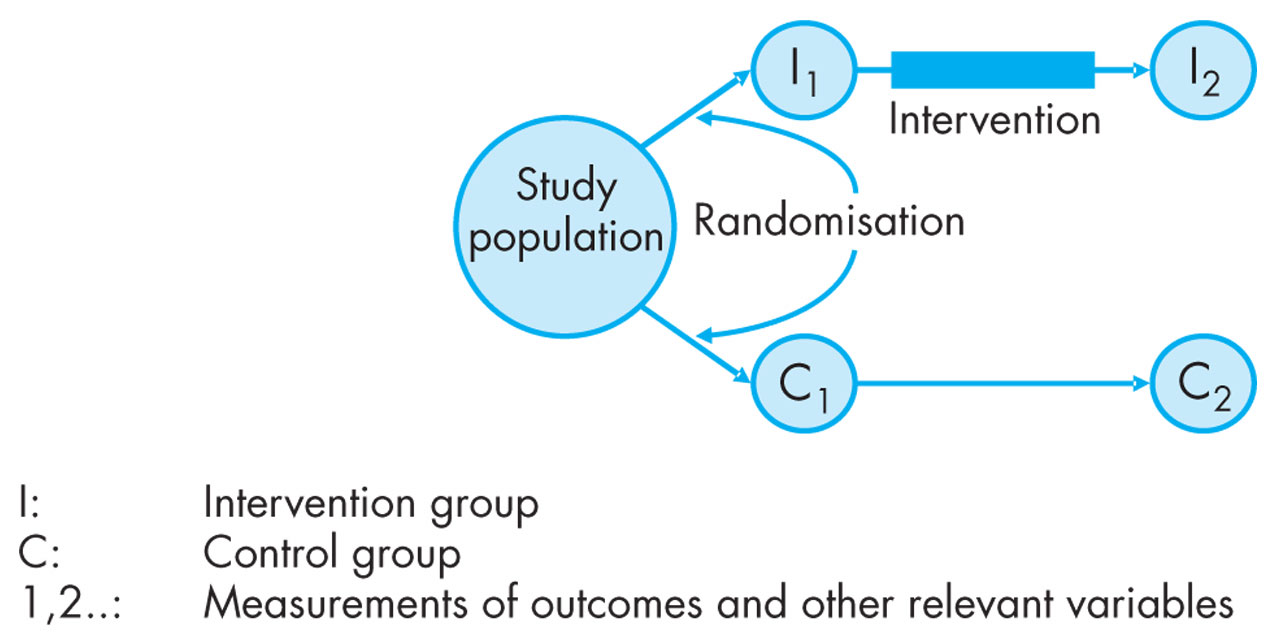
The next question is whether or not the changed exposure had the intended effect on health and other study outcomes. Figure 3 illustrates how important it is to be able to distinguish between lack of impact of the intervention and lack of effect of exposure on health. The figure illustrates two programmes (A and B) with the same overall change in health: 3–4% of the target group experienced better health. This is of course a very modest change to the better. In a “black box” study in which the researcher only measures the health outcomes in the two groups the conclusion will be that the two programmes are equally (in)effective. This is, however, an unsatisfactory analysis. Figure 3 shows that the two programmes worked very differently. In programme A there were two clear signs of programme failure: only 50% of the target group heard about the programme; and only 10% of the participants changed behaviour. In programme B the programme worked extremely well but only 5% of those who changed behaviour experienced improved health (theory failure). The basic point here is that it does not help that the pill has effect if the patient does not take it (programme A) and it does not help that the patient takes the pill if it has no effect (programme B). In intervention research we should always be able to distinguish between programme and theory failure (or success!), and the way to do this is to study all steps in the intervention process.

Programme failure or theory failure? No impact of the intervention on exposure or no effect of exposure on health?
In some cases we know (or believe that we know) enough about the association between exposure and disease (such as passive smoking and lung diseases, heavy lifting and low back pain, low decision latitude and absence from work). In those cases we do not have to carry out large aetiological intervention studies in order to show this once more. Rather, we need prevention effectiveness studies in order to find out how to reduce the exposure. In many intervention studies it is unclear whether the aim is to find out how to reduce exposure or how to reduce the occurrence of the disease. This is regrettable since the methodological requirements for carrying out prevention effectiveness studies and aetiological studies of diseases are very different.w20 The main differences are indicated in table 2.
Two types of intervention studies: aetiological and prevention effectiveness studies
In aetiological studies we typically need large samples, randomisation, blinding, etc as already discussed above. In the prevention effectiveness studies the removal or reduction of the exposure is the very purpose of the intervention. We do not need large samples for this, but rather case studies of different settings in which to test our programme theory for prevention effectiveness.w7 12 13 26 Health promotion programmes, for example, should not only be tested in middle class samples, which so far has been the most common setting, but also among blue collar workers, immigrants, young workers, obese workers, workers in small and medium size enterprises, or temporary workers. Only by testing the intervention paradigm in such different settings can the basic programme theory be challenged. Furthermore, the use of qualitative methods is important here in order to study the dynamics of the intervention process.w2 7 10 16 w27
EXAMPLES OF GOOD INTERVENTION STUDIES
Ten examples of good intervention studies are included in the reference list.11–20 These studies are not necessarily the 10 best occupational intervention studies ever performed but, although very different, the studies have one important thing in common: They all have a high degree of conclusiveness. They add substantially to our scientific knowledge and at the same time they all represent ways of tackling important workplace health problems in practice.
The effect of debriefing was studied by Carlier and colleagues11 after the major airplane disaster by Schiphol airport in 1992. The authors found no positive effects of debriefing among the policemen who took part in the rescue work. This result corresponds well with other studies and with reviews on debriefing.w28–33 Engels and colleagues12 found improvements in ergonomic load after an educational course for nurses. Evanoff and colleagues13 studied the introduction of mechanical lifts in hospitals and long term care units. They found decreased rates of musculoskeletal injuries and lost workdays and a positive correlation between use of lifts and the two outcomes. Krause and colleagues14 showed a substantial reduction in the number of accidents after the initiation of behaviour based interventions at 73 worksites. Larson and colleagues15 studied the effects of an intervention in a hospital aiming at improved hand washing behaviour among the employees. The intervention resulted in better hygiene and fewer hospital infections. Loisel and colleagues16 studied ergonomic and clinical interventions among workers with long term absence due to back pain. The study showed substantial effects of both interventions. In the Finnish study of carbon disulphide exposed workers,17w34 w35 a clear excess risk of ischaemic heart disease was seen after a few years of follow up compared with the well chosen control group. A vigorous intervention resulted in decreasing risk among the exposed workers. This is an example of a well designed study that “convinced the world”. Oldenburg and colleagues18w36 performed a randomised health promotion intervention study in the Australian ambulance service. Four different types of intervention were compared. Orth-Gomér19 studied shiftwork systems among Swedish policemen and found that a “clock-wise” system resulted in better health and sleep than a “counter clock-wise” system. Finally, Rydstedt and colleagues20w37 w38 studied psychological hassles among Stockholm bus drivers. After a systematic reduction of sources of hassles in the traffic and from the passengers, the wellbeing of the drivers was improved and blood pressure was reduced.
Some of these studies were pure prevention effectiveness studies,12,18 some were aetiological studies,14,17,19 some combined the two aims,13,15,20 and some studied aetiology in secondary prevention.11,16 Two of the studies had a randomised control group,16,18 two had no control group,13,14 and the remainder had well chosen comparison groups. The follow up time went all the way from 8 weeks19 to 15 years.17 The number of participants was less than 25 in the Stockholm bus drivers’ study and 6835 work-years in the Evanoff study. All the studies had some kind of theoretical basis, and this basis was explicitly stated in some of the studies.14–16,18,20 Two of the studies16,18 also included an evaluation of cost effectiveness.
Taken together, these studies illustrate the great diversity of problems that can be studied with the use of the intervention design. All the studies “made a difference” in their respective fields. This illustrates a central point with regard to intervention studies: although they are very costly with regard to time and manpower, the history of intervention research shows that they are well worth the effort. The benefit from well performed intervention studies is double: theoretical conclusiveness and practical usefulness.
WHAT NEEDS TO BE DONE IN THE FUTURE?
So far, the main point of this paper has been that we need to study all the steps in the intervention process from the planning and implementation of the intervention over the impact on exposure to the effect on health. Before concluding, I would like to emphasise another important point: Occupational intervention studies take place at workplaces, and we should always remember the simple fact that the purpose of a workplaces is to produce goods and services—not to serve as arenas for intervention research. This has two main consequences.
Take home messages
Why intervention research?
Occupational intervention research can:
-
Lead to the establishment of causal evidence with a high level of conclusiveness
-
Elucidate ways of implementingimprovements at the worksites
-
Contribute to dissemination of convincing and relevant research
-
Improve learning and mutual understanding between researchers and practitioners
About the use of the design of the randomised controlled trial (RCT)
There are many good reasons for not being able to use the design of the RCT in occupational intervention studies. But there are no good reasons for disregarding the methodological problems caused by not using this design.
About prevention effectiveness and aetiology
Prevention effectiveness and aetiology of health are equally important: It does not help that the patient takes the pill, if it has no effect. And it does not help that the pill is effective, if the patient does not take it. Hence, both issues should be studied carefully.
About the collaboration with the workplaces
The workplaces are not arenas for intervention research. Their goals are to produce goods and services and to survive economically. The long term challenge for occupational intervention epidemiology is to develop strategies and models where better working conditions and better employee health are necessary conditions for the development and survival of the workplaces.
First, it is necessary to distinguish between the three stages of contact with the workplace: (1) accept (the company has accepted the study); (2) access (the researchers have access to the workplace, the employees, and to written material); (3) commitment (the relevant parties at the workplace consider the intervention as their own and give it high priority). The goal should always be to build the intervention study on the mutual commitment of the workplace and the researcher.
Secondly, it is important that the workplace benefits from participating in the intervention study. Two of the studies above addressed the issue of cost-benefit,16,18 but the activities of almost all occupational intervention studies are still “sideline” activities that are not directly relevant for the core tasks of the workplace. In the future, researchers and workplaces should develop methods in which the efforts for better work environment and for increased productivity and quality are combined and integrated. In fig 4 a model for such integration is proposed. The model was developed by a group of Nordic researchers in the city of Sirdal—hence the name “Sirdal Model”.w24 The model combines the four goals of better work environment, better productivity/quality, better employee health/wellbeing, and better customer/client satisfaction. The implicit assumption of the model is that better working conditions and health among the employees will lead to higher productivity/quality and also increased customer satisfaction. Furthermore, higher productivity and more satisfied customers will also benefit the workplace and the employees. A few researchers have already tested (parts of) the Sirdal model. There are huge potentials for future collaboration between researchers and workplaces in studying the effects of truly integrated intervention programmes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The Sirdal model of work environment, workers’ health, production, and customer satisfaction.
Policy implications
-
High quality occupational intervention studies are important for establishing convincing evidence on the effects workplace interventions.
-
Research funds, organisations, and companies should encourage and provide resources for good occupational intervention research.
Thus, occupational intervention research faces two major challenges in the years to come: (1) To make further improvements with regard to theory and methods. In particular to work with clear and explicit theories of intervention and to study all steps in the intervention process with valid instruments. (2) To develop comprehensive models and strategies where good working conditions and a high level of employee health are integrated and necessary conditions for the development of competitive and sustainable workplaces.
REFERENCES
References
Supplementary materials
Web-only References
The references are available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement: