Article Text

Statistics from Altmetric.com
Endotoxins, part of the outer membrane of Gram negative bacteria, are a potent inducer of neutrophilic airway inflammation. A large number of studies in occupational epidemiology has shown that exposure to endotoxins increases the likelihood of organic dust toxic syndrome, chronic bronchitis, and asthma-like syndrome. In contrast, it has been shown that exposure to endotoxins in the occupational and environmental setting protects from respiratory allergies and sensitisation to allergens.
With respect to asthma, the evidence is conflicting at first glance. While some studies indicated an increased risk of asthma after endotoxin exposure, others have shown that endotoxin exposure protects from asthma. However, these differences can be explained when different asthma phenotypes are taken into account. The risk of atopic asthma, mainly dominated by eosinophilic response, is decreased in those exposed to endotoxins. In contrast, the risk of non-atopic asthma, characterised by neutrophilic response, is enhanced in subjects with higher endotoxin exposure. These data are in accordance with the so-called hygiene hypothesis and have been supported by animal studies and at the cellular level.
At the workplace, measures should therefore be taken in order to reduce endotoxin exposure. The effectiveness of such measures with respect to the incidence of diseases associated with a chronic neutrophilic inflammation in the airways should be assessed in intervention studies. At the same time we need to learn whether the evidence from epidemiological studies in farming environments might help us to obtain effective intervention strategies against allergies.
WHAT ARE ENDOTOXINS?
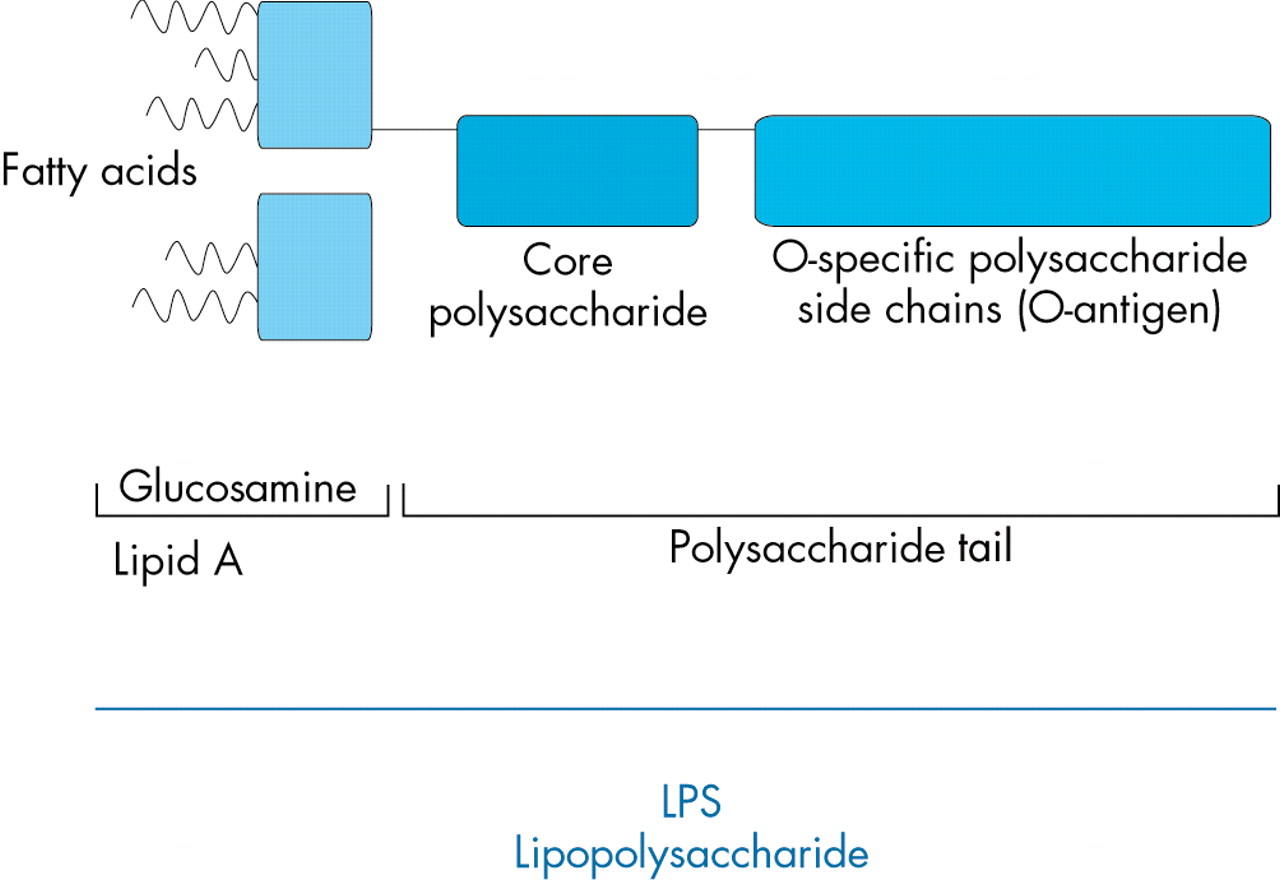
In contrast to Gram positive bacteria, Gram negative bacteria are surrounded by an inner and an outer membrane.1 Endotoxins are parts of the outer membrane. Their purified derivatives are called lipopolysaccharides (LPS).2
Endotoxins and LPS are present in the oral and nasal cavities of humans and animals. They can also be found ubiquitously in occupational and environmental settings on surfaces of animals, plants, and soil.2,3 In these environments they are quantified in highly variable concentrations.4 The immune stimulatory capacity of endotoxins can only be inactivated at high temperatures (for example, 160°C for 4 hours). Therefore, endotoxins are active for much longer than the lifetime of the bacteria themselves.
In occupational settings, endotoxins mainly occur in environments with high exposure to organic dusts. These are primarily agricultural environments (livestock, grain dust),5,6 textile production,7 and waste processing.2,8
In the domestic environment, significant concentrations occur from pets kept indoors, carpeting, as well as air conditioning.4 In the agricultural setting, endotoxins have also been shown to be transported from the animal houses into the home environment of farmers and farmers’ children.9 Recent measurements on the endotoxin concentrations in house dust have been summarised by Michel.10 In these studies, the mean endotoxin content of settled bedroom floor dust varied between 7.3 and 63 EU/mg. Exposure from, for example, intensive animal production facilities increases the background exposure to endotoxins in rural areas11 compared to urban settings.12,13
Some examples for the range of exposures found in several environments are given in table 1. However, the results of these analyses largely depend on the method used (see “Exposure assessment”).
Examples of the range of endotoxin exposure in different environments
EXPOSURE ASSESSMENT
Endotoxins are usually measured in samples of airborne or settled dust. One of the problems with the exposure assessment is a lack of standardisation of exposure assessment methods and environmental sampling strategies.14 The kinetic limulus amoebocyte lysate (LAL) method, an in vitro biological method, has been widely used for endotoxin measurements since the 1980s.15 The test was standardised by the US Food and Drug Administration and is usually used as a marker of Escherichia coli contamination in, for example, water, food, or infusions.16
The LAL test measures the biological activity of free cell wall dissociated LPS. The lysate used for the test is prepared from the horseshoe crab (Limulus polyphemus).17 Therefore, different test batches might give different results, making the use of an internal standard endotoxin necessary. The results of the test should be expressed as endotoxin units (EU) as the reactivity and molecular weight of different species or strains of endotoxin may vary largely in the hydrophilic and lipid A moiety.15
Due to the different protocols used, large variations in the analyses of endotoxins might also occur between laboratories. Therefore, only intra-laboratory results should be directly compared.15 The lack of consistency between laboratories makes it difficult to propose exposure threshold values for endotoxins.14 The new European standard for endotoxin measurement at the workplace might help to overcome this problem.18
KNOWN EFFECTS OF ENDOTOXINS AT THE CELLULAR LEVEL
Endotoxins are known to have strong immune stimulatory and proinflammatory properties, even in very small amounts.19 After inhalation, endotoxins enter the airways where they encounter alveolar macrophages carrying CD14, an LPS binding receptor. The binding of LPS to CD14 is mediated by the LPS binding protein (LBP). Via toll-like receptors (TLR-2 and TLR-4) the alveolar macrophages are activated, leading to the production and release of proinflammatory cytokines, chemokines, adhesion molecules, and other mediators.2,20 Cytokines associated with endotoxin exposure are TNF-α, interleukin (IL) 1-β, IL-6, and IL-8, as well as metabolites of arachidonic acid.2 These cytokines recruit and activate neutrophils, resulting in local and systemic inflammation with leucocytosis and neutrophilia.2,20
Genetic variations, especially in the polymorphism of the TLR-2 gene, are thought to be responsible for variations in the individual susceptibility to effects of endotoxins.21,22
ENDOTOXINS AND RESPIRATORY HEALTH; RESULTS FROM OCCUPATIONAL EPIDEMIOLOGY
Endotoxins can be found at higher concentrations in all occupational environments with exposure to organic dust (for example, farming, cotton production, waste processing). Of these, farmers are the professional group that has been most extensively studied throughout the world. The results of these studies may well serve as a model for the association between endotoxin exposure and airway inflammation.
As early as 1555, Olaus Magnus indicated that the respiratory tract of farmers is at increased risk for occupational diseases.23 This has been confirmed in a large number of studies (for reviews, see Schenker15 and Radon and Nowak24). Respiratory diseases among farmers can be compensated as occupational disorders in many industrialised countries, and the number of claims for compensation is high in these countries. In this context, the most important diseases affecting the airways of farmers are:
-
Extrinsic allergic alveolitis or farmer’s lung
-
Organic dust toxic syndrome
-
Chronic bronchitis
-
Respiratory allergies, asthma, and asthma-like syndrome.
Of these, organic dust toxic syndrome, chronic bronchitis, and asthma have been considered to be associated with endotoxin exposure at the workplace.
Organic dust toxic syndrome
Organic dust toxic syndrome (ODTS) is a systemic inflammatory reaction with flu-like symptoms. These include fever, myalgias, chest tightness, chills, and dyspnoea 4–8 hours after exposure.4,24 The symptoms resemble the acute form of extrinsic allergic alveolitis, a type III and type IV sensitisation that is much less common than ODTS with a longer duration.25 In the airways, obstruction might occur together with increased airway hyperreactivity and a reduced alveolar diffusion capacity.4 The affected worker usually recovers within 36 hours without need for treatment. Often the disease is characterised by a clustering of cases in one occupational setting after, for example, cleaning of animal houses.
Endotoxins are considered to be of uppermost importance in the development of ODTS.6 However, if repeatedly exposed, some degree of tolerance seems to develop. The mechanism leading to this tolerance is still poorly understood, but one study indicated that it is associated with interference with transcription factor pathways and a reduced gene expression.26
Epidemiological studies have shown that ODTS is very common in farmers. In the European Farmers’ Study, a cross-sectional study including 7000 farmers across Europe, the lifetime prevalence ranged from 15% in crop producers27 to 23% in pig farmers.28 In one study from Sweden the annual incidence was 1%.29
In the past, ODTS has been considered a self-limiting, harmless syndrome.25 However, newer studies indicate that ODTS is associated with an increased risk of chronic bronchitis in farmers.30–32 Therefore, the acute neutrophilic inflammation of the lung seems to cause a chronic neutrophilic inflammation associated with chronic symptoms in repeatedly exposed workers.
Chronic bronchitis
There is a large body of literature showing that exposure to farming environments increases the risk of chronic bronchitis. The prevalence among farmers ranges from 5%33 to 39%.34 In the European Farmers’ Study, farmers in the age group 20–44 years were already at increased risk for chronic bronchitis.28 In a recent meta-analysis, the summary odds ratio for chronic bronchitis among animal farmers compared to unexposed reference populations was 2.0 (95% CI 1.7 to 2.4).35
The endotoxin and β-glucan concentrations in organic dust are thought to be major risk factors for the chronic neutrophilic inflammation of the airways among farmers.6 However, several studies have indicated that among farmers the symptoms of chronic bronchitis do not correlate with an airway obstruction.15 Beside the fact that many of the epidemiological studies were done on a cross-sectional base, potentially resulting in a healthy worker survivor effect,36,37 it is difficult to clearly distinguish between the different chronic respiratory diseases in questionnaire based studies. As shown in fig 2, wheezing might indicate early symptoms of chronic bronchitis as well as asthma. In addition, without allergic sensitisation, physicians might fail to diagnose asthma in a patient with asthma-like symptoms.11 This problem is discussed in the next section.

Structure of lipopolysaccharides (LPS).

{kind=link}
{kind=link}
Venn diagram of doctors’ diagnosed asthma, wheezing without a cold, and chronic bronchitis among 18–44 year old adults living in rural areas of Lower Saxony, Germany (n = 6820).
Allergic sensitisation, asthma, and asthma-like syndrome
In the past, cattle farming was shown to be a risk factor for allergic sensitisation against cattle epithelium.15 At the same time, sensitisation against storage mites and moulds has been shown, especially among farmers (see Schenker15 for a review). In the cotton industry, asthma symptoms mainly occurring after days off work (“Monday asthma” or byssinosis) were associated with endotoxin exposure.38 In a prospective cohort study in the Chinese cotton industry, the cumulative incidence over 15 years was 24% in cotton workers compared to 0% in silk workers.38 At the same time, it is well known that endotoxins can exacerbate airflow obstruction and inflammation in patients with atopic asthma. Likewise, subjects with atopic asthma have an enhanced respiratory response to endotoxin.39
During recent years more studies have included unexposed reference groups. In this context, the evidence for the association between farming environments and asthma and allergies became conflicting. For example, the European Respiratory Health Survey, a general population survey among adults throughout Europe, indicated an increased odds ratio of 2.6 (95% CI 1.3 to 5.4) for asthma among farmers.40 In contrast, in the context of the European Farmers’ Study, allergic asthma and respiratory allergies were only more frequent among crop farmers, especially among farmers involved in flower production, with a prevalence of 5%.27 In this study, the prevalence of asthma was 1% among animal farmers aged 20–44 years compared to 3% in the general population.28 Of 100 pig farmers with work related respiratory symptoms, 16% were sensitised to common allergens compared to 18% in the general population, even though the exposure to, for example, house dust mites, was 50-fold increased.41
Atopic and non-atopic asthma
One potential explanation for these contradictory results is that not all asthma is associated with allergic sensitisation. For farmers with symptoms of asthma but without allergic sensitisation, the term asthma-like syndrome was coined.15 Symptoms associated with asthma-like syndrome are chest tightness, wheeze, or dyspnoea, and a cross-shift decline in FEV1 of usually less than 10%. In contrast to atopic asthma the syndrome is associated with a neutrophilic inflammation of the airways.15 As described by Schenker 1998,15 several studies have indicated that endotoxins might be the agent responsible, causing the airway inflammation responsible for the asthma-like syndrome.
Overall, asthma-like syndrome mainly describes what now is known as non-atopic asthma.42 It has been estimated that about 50% of all asthma cases are attributable to this non-atopic asthma based on neutrophilic airway inflammation; in the occupational environment it might even be more.42 This is supported by our recent finding that only about half of young adults living in a rural area of Lower Saxony, Germany, who reported wheezing were also sensitised against common allergens or reported symptoms of allergic rhinitis. Endotoxins are one of the relevant exposures associated with non-atopic asthma.15,25,30,42,43
Eduard and colleagues44 have shown that animal farmers are at increased risk of non-atopic asthma with increasing endotoxin concentration at the workplace, while allergic sensitisation and atopic asthma was inversely related to endotoxin levels in airborne dust. A similar association has recently be shown by our group.11 Therefore, it seems to be important that the different phenotypes of asthma are taken into account when the prevalence of asthma in different populations is compared.
It has been argued that genetic differences might explain the reduced risk of atopic asthma and allergic sensitisation in animal farmers.45,46 However, while genetics might play some role in the observed differences (healthy worker effect), environmental studies as well as findings from in vivo and in vitro studies contradict this explanation.47
Range of exposure in different areas of agriculture
Beside the different phenotypes of asthma, the type of farming has to be taken into account when the effect of farming on respiratory health is under consideration. The term “farming” covers a large variety of tasks, techniques, and products. Type, duration, and level of exposure to allergens and irritants vary from, for example, grain production to greenhouse farming and from dairy farming to poultry production.5 Exposure also depends on climate.48 Therefore, the European Farmers’ Study has shown large differences in the prevalence of atopic asthma and allergies between animal farmers and greenhouse farmers.27,28 These environments differ considerably in the amount of endotoxins, ranging from a median of 3 EU/m3 in greenhouses to 610 EU/m3 in swine confinement houses.5
Current evidence therefore suggests that endotoxins in the occupational environment are associated with a decreased risk of atopic diseases. In contrast, the risk for non-atopic asthma increases with increasing endotoxin exposure. These hypotheses are supported by data from the general environment.
ENDOTOXINS AND RESPIRATORY HEALTH; RESULTS FROM ENVIRONMENTAL EPIDEMIOLOGY
Several epidemiological studies have been conducted on an international base in order to determine the prevalence and risk factors for asthma and allergies across the world.49 These studies have indicated that the prevalence of respiratory allergies and asthma is considerably higher in high income countries compared to developing countries. In addition, while the prevalence of respiratory allergies and asthma was significantly lower in Eastern Germany compared to the Western part of the country at the time of the German reunification, these differences have been levelling off within less than 10 years due to a rise of atopic diseases in Eastern Germany. One explanation for the described differences is covered by the “hygiene hypothesis”, stating that contact to microbial components can protect from the development of hay fever and possibly other allergic diseases.50 This has been supported by several factors shown to be associated with a decreased risk of respiratory allergies in epidemiological studies:47
-
Increasing number of older siblings
-
Day care attendance during the first years of life
-
Gastrointestinal microbes
-
Early exposure to farms.
The latter has been confirmed by a large number of studies from several countries across the world, showing a protective effect of being raised on a farm (for reviews, see Braun-Fahrlander47 and Kabesch and Lauener51) and exposure to animal confinement houses during childhood on the prevalence of asthma and nasal allergies. As in the occupational studies discussed above, the protective effect of early contact to farms seems to be confined to those with contact to livestock farming as opposed to children with contact to farms with mainly crop production.52
Although it is assumed that it is the early-life farm contact that confers a protective effect against allergic diseases, new data show that regular farm animal contact starting later in life is also associated with a decreased prevalence of sensitisation among adults.53 Two small longitudinal studies among young adults54 and schoolchildren55 suggest that farm animal contact starting at a later age not only reduces the incidence, but is also associated with a more frequent loss of sensitisation. The study among 42 Austrian agricultural students54 showed a remission of allergic disease among those with new contact to farm animals; the study, however, was hampered by a high loss to follow up. The other study55 was a three year follow up of 844 Austrian schoolchildren (mean age at baseline 8 years). Farm children (15%) lost sensitisation significantly more often than non-farm children (odds ratio 8, 95% CI 2 to 32). To our knowledge, no other study of the influence of late starting farm contacts is available.
Possible causal agents explaining the protective effect of farm contact were sought in the exposure to endotoxin, bacterial DNA, muramic acid, pathogens like Toxoplasma gondii and Helicobacter pylori, and possibly mould components.56 The reaction of the immune system on stimulation of Toll-like receptors (TLRs) may determine the protective effect against allergic disease seen with the contact to microbial components.57 Thus, endotoxins seem to be one of the important exposures occurring in the animal farming environments that might protect from respiratory allergies. Therefore, the distribution of endotoxins in the home environment of children living in rural areas has been studied. A greater exposure to endotoxin in the mattresses of schoolchildren in Switzerland, Austria, and Germany was associated with a lower risk of asthma and allergies.58 In the context of this study it was shown for farmers’ and non-farmers’ children that the indoor home endotoxin levels were associated with the child’s activity on a farm. Additionally, pet keeping was a predictor of the endotoxin level at home.9 This association is consistent with findings from other studies (see Liu59 for a review). The level of indoor endotoxin exposure was inversely related to sensitisation or respiratory allergies in some of these studies, but not for all subpopulations.
Overall, the prevalence of allergic symptoms and symptoms of chronic bronchitis depend on the dose of endotoxins and allergens in the environment (table 2). Higher concentrations of endotoxins in the occupational environment lead to an increased risk of chronic bronchitis and non-atopic asthma. This association was recently confirmed for subjects living in areas with environmental exposure to endotoxins due to intensive livestock production.11 In contrast, increased endotoxin concentrations in the occupational and general environment might protect from sensitisation to allergens.
Prevalence of respiratory diseases depends on concentration of endotoxins and allergens in the occupational and home environment
There is still some controversy as to whether endotoxin exposure is actually the cause for the inverse association between farm contact and the lower rate of respiratory allergies.60 However, as the inverse association between endotoxin exposure and respiratory allergies is also consistently seen among non-farmers, most other factors do not seem to be crucial (for example, genetics, level of air pollution, nutrition).60
POTENTIAL MECHANISMS
The classical hygiene hypothesis assumes that the increase in Th1 cell production associated with infections skews the immune system away from Th2 cell production. Therefore, the prevalence of Th2 dominated diseases like atopic diseases might be decreased in subjects exposed to infectious agents.50
The observation that parasites associated with a Th2 dominated immune response like, for example, hookworms, also resulted in a reduced prevalence of atopic diseases contradicted the classical hygiene hypothesis.50,61 Therefore, it has recently been hypothesised that the immune response might be modified by IL-10 produced by Th3 cells. With respect to cat allergen exposure it has been suggested that a combination of IL-10 with IL-4 may skew the immune response in favour of IgG4 production instead of IgE production.62 The result is that a non-pathogenic Th2 immune response might be induced.63
The underlying mechanisms of this bidirectional response have been shown in animal studies and in vitro experiments. The results of these studies have been excellently reviewed by Renz and Herz.64
Nevertheless, it is still unknown whether endotoxins are the causal component for the protection from respiratory allergies. Cohort and intervention studies are on the way to giving further evidence for the prevention of atopic diseases in the long run. Currently it has been recommended that bacterial extracts should not yet been used clinically.65 Our current knowledge on the adverse health effects of endotoxins with respect to chronic bronchitis and non-atopic asthma has to be used for effective prevention strategies at workplaces with high exposures to organic dust.
QUESTIONS (SEE ANSWERS ON P 10)
-
Endotoxins are:
Part of the outer membrane of Gram negative bacteria
Part of the inner membrane of Gram negative bacteria
Part of the outer membrane of Gram positive bacteria
-
One of the occupations mostly affected by endotoxin exposure is:
Bakers
Greenhouse workers
Hairdressers
Animal farmers
-
Exposure to endotoxins is highest in mattresses of:
Urban citizens
Rural citizens with regular contact to animal farms
Rural citizens without contact to animal farms
-
Exposure to endotoxins decreases the risk of:
Chronic bronchitis
Asthma
Atopy
Extrinsic allergic alveolitis (farmer’s lung)
Organic dust toxic syndrome (ODTS)
-
Organic dust toxic syndrome (ODTS):
Is characterised by clustering of cases
Has long term effects
Is a type IV sensitisation
Is associated with restrictive lung function changes
Is associated with Th2 cell production
Acknowledgments
I am grateful to Rudolf Schierl and Anja Schulze for critical review of the paper.
REFERENCES
Footnotes
-
Competing interests: none declared