Article Text

Abstract
Background: There is little previous information of the effects of size fractioned particulate air pollution and source specific fine particles (PM2.5; <2.5 μm) on asthma and chronic obstructive pulmonary disease (COPD) among children, adults and the elderly.
Objectives: To determine the effects of daily variation in levels of different particle size fractions and gaseous pollutants on asthma and COPD by age group.
Methods: Levels of particulate air pollution, NO2 and CO were measured from 1998 to 2004 at central outdoor monitoring sites in Helsinki, Finland. Associations between daily pollution levels and hospital emergency room visits were evaluated for asthma (ICD10: J45+J46) in children <15 years old, and for asthma and COPD (ICD10: J41+J44) in adults (15–64 years) and the elderly (⩾65 years).
Results: Three to 5 day lagged increases in asthma visits were found among children in association with nucleation (<0.03 μm), Aitken (0.03–0.1 μm) and accumulation (0.1–0.29 μm) mode particles, gaseous pollutants and traffic related PM2.5 (7.8% (95% CI 3.5 to 12.3) for 1.1 μg/m3 increase in traffic related PM2.5 at lag 4). Pooled asthma–COPD visits among the elderly were associated with lag 0 of PM2.5, coarse particles, gaseous pollutants and long range transported and traffic related PM2.5 (3.9% (95% CI 0.28 to 7.7) at lag 0). Only accumulation mode and coarse particles were associated with asthma and COPD among adults.
Conclusions: Among children, traffic related PM2.5 had delayed effects, whereas among the elderly, several types of particles had effects that were more immediate. These findings suggest that the mechanisms of the respiratory effects of air pollution, and responsible pollutants, differ by age group.
Statistics from Altmetric.com
People with asthma and chronic obstructive pulmonary disease (COPD) have been reported to be more susceptible to the adverse effects of air pollution than healthy people.1 Many epidemiological studies in Europe and North America have linked different air pollution measures with asthma and COPD hospital admissions and emergency room visits.2–4 However, the differences in the effects of air pollution on asthma and COPD among children, adults and the elderly have rarely been investigated in the same study.3 ,5
There is evidence that ultrafine particles (<0.1 μm in aerodynamic diameter) affect our respiratory system in a disadvantageous way.6 ,7 It may be that ultrafine particles have greater respiratory effects than generally monitored respirable (PM10, <10 μm) and fine particles (PM2.5, <2.5 μm). This argument rests on the physical and chemical characteristics of ultrafine particles, such as their higher number concentration, better lung deposition, larger surface area, ability to inhibit phagocytosis and higher toxicity.7 ,8 However, because of the limited availability of measurement data on particle size fractions, there are very few epidemiological studies evaluating the effects of size fractioned particles on exacerbation of asthma and COPD.3 ,9
In this study, we evaluated the effects of the size fractioned particulate and gaseous air pollution on daily asthma and COPD hospital emergency room visits. We also identified four PM2.5 sources and assessed their effects on the visits. The analyses were performed separately for three different age groups in order to investigate whether the effects of air pollution differ among people of various ages.
MATERIAL AND METHODS
We obtained data on hospital emergency room visits for 1998–2004 for all three public hospitals in the Helsinki metropolitan area (1 million inhabitants, 745 km2), Finland, from the national register. These hospitals encompass, in practice, all asthma and COPD hospital emergency room visits in the area. For asthma visits, we used International Classification of Diseases Revision 10 (ICD-10) codes J45 and J46, and for COPD codes J41 and J44. We analysed a priori chosen age groups that were children (aged <15 years), adults (15–64 years) and the elderly (⩾65 years). For adults and the elderly, we determined the associations between pollutants and pooled asthma–COPD visits, as these conditions are difficult to distinguish. Asthma and COPD visits were also analysed separately.
We used the same outdoor air pollution data measured at urban background stations as in our earlier report.10 Missing data (maximum 2% of days) were replaced with measurements from the closest measurement station (correlation at least 0.60). Briefly, daily particle size distribution was measured with a differential mobility particle sizer. Based on these measurements, the following modes were defined11: nucleation mode (<0.03 μm), Aitken mode (0.03–0.1 μm) and accumulation mode (0.1–0.29 μm). Particles <0.1 μm in the aerodynamic diameter were counted as ultrafine particles. Coarse particulate mass was obtained by subtracting PM2.5 from PM10.
Daily mass concentration of PM2.5 was apportioned between sources using the EPA PMF 1.1 model.12 In the source apportionment, we used, in addition to the above mentioned pollutants, SO2 and SO42− (see table S1 in the online supplement). We identified four source categories: traffic exhaust, long range transport, soil and road dust, and coal/oil combustion (see table S2 and figs S1 and S2 in the online supplement). Detailed description of the source apportionment is provided in the appendix (online). In the analyses for PM2.5 sources and emergency room visits, we used all four sources simultaneously in the model.
We analysed the associations between daily air pollution levels and emergency room visits with Poisson regression and penalised thin plate regression splines in the generalised additive models framework. We implemented modelling using R version 2.1.113 and mgcv 1.3–7 procedure.14
We used 24 h median number counts for ultrafine particles and nucleation, Aitken and accumulation mode particles because of the rightly skewed distribution of particles. For particulate mass and NO2 we used 24 h average concentrations, and for CO and O3 maximum 8 h moving average. Lag 0 was defined as the 24 h period from midnight to midnight, of the day of the visit, and lag 1 as the preceding 24 h period, and so on. Lags up to 5 days were tested.
We built the basic model controlling for time trend, weekdays, general holidays, weather variables (temperature, relative humidity, air pressure), and influenza and pollen episodes. The dummy variable for pollen episode was constructed based on the counts of four of the most allergenic species. More detailed description of the model building is provided in the online supplement. We also tested the differences in coefficients of pollutants between the age groups with t test assuming 0 covariance between the coefficients (ie, using the formula):

To avoid over-smoothing and to define the amount of autocorrelation in the residuals, we did visual inspection of the smoothed curves and partial autocorrelograms of the residuals. All results are provided as per cent change in hospital emergency room visits for an interquartile increase in the pollutant concentration.
RESULTS
There were a total of 4807 asthma hospital emergency room visits among children, and 6312 and 7239 pooled asthma–COPD visits among adults and the elderly, respectively. Descriptive data for daily hospital emergency room visits, pollutant concentrations and weather variables are shown in table 1.
Correlation of ultrafine particles with NO2, CO and traffic related PM2.5 was moderate or high (0.65, 0.45 and 0.74, respectively). Gaseous pollutants NO2 and CO correlated moderately with each other (0.43). Of the particulate measures, nucleation mode particles correlated highly with ultrafine particle counts (0.92), and accumulation mode particles with PM2.5 (0.88). The correlations between pollutants, weather variables and source specific PM2.5 are given in table S1 (online).
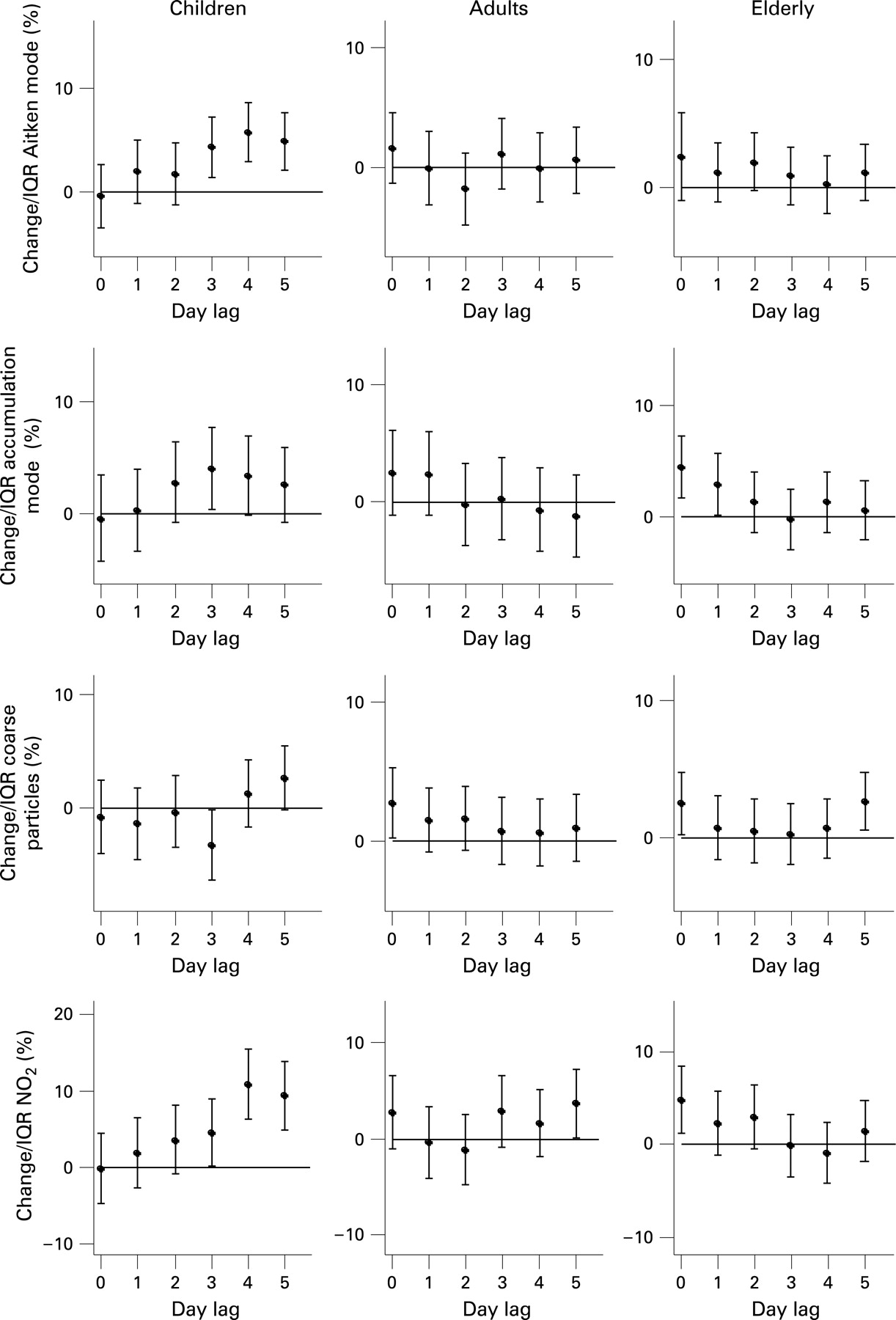
All particle fractions below 250 nm, and NO2 and CO were associated with asthma emergency room visits for children at 3–5 day lags (table 2). Asthma visits from children were also associated with ultrafine particles at lags 4 (6.6% (95% confidence interval (CI) 2.34 to 11.0)) and 5 (6.7% (95% CI 2.48 to 11.0)).
When more accurate particle size segregation was used, nucleation mode was associated with asthma visits of children with a lag of 5 day (5.4% (95% CI 0.74 to 10.2)), compared with Aitken mode with lags of 3, 4 and 5 days, and accumulation mode with lags of 3 and 4 days (fig 1). We found positive associations for the pooled asthma–COPD visits of the elderly with PM2.5, accumulation mode particles, coarse particles, CO and NO2 at short lags (table 2). Among adults, the current day coarse and accumulation mode particle levels were statistically significantly associated with the pooled asthma–COPD visits, and the effect estimate for ultrafine particles was also considerable.
Two pollutant models for lag days 0–5 were then used to study whether the above observed associations between pollutants that were not too highly correlated (PM2.5, nucleation and Aitken mode, coarse particles, NO2 and CO) were independent of each other. Among children, the effect of ultrafine particles disappeared when analysed together with NO2 (−0.89% (95% CI −6.11 to 4.62) for ultrafine particles at lag 4). Overall, the effect of NO2 was independent of other pollutants. The estimate of the association between CO and asthma visits was reduced when CO was adjusted for NO2 or for ultrafine particles, but PM2.5 did not confound the association. Correlations between ozone and other pollutants were typically low (−0.23 to 0.32) and therefore ozone was not included in the two pollutant models.
Among the elderly, ultrafine particles confounded the association between PM2.5 and the pooled asthma–COPD visits (1.8% (95% CI −0.53 to 4.1) for PM2.5 at lag 1). Also, the estimate for ultrafine particles reduced to 0. The current day association for PM2.5 was reduced to 2.3% (95% CI −0.01 to 4.7) when analysed with NO2, and to 2.3% (95% CI 0.09 to 4.6) when analysed with CO. The association of the current day coarse particles was also reduced when adjusted for ultrafine particles (1.7% (95% CI −0.65 to 4.10)). Very similar reductions were observed when adjusting coarse particles for PM2.5, CO and NO2. However, among adults, the observed coarse particle association was not confounded by other pollutants.
The traffic related PM2.5 had a strong and lagged effect (7.8% (95% CI 3.5 to 12.3) at lag 4) on the asthma visits of children (fig 2). Traffic related and long range transported PM2.5 had immediate effects on the pooled asthma–COPD visits of the elderly (3.9% (95% CI 0.2 to 7.7) and 4.5% (95% CI 1.2 to 7.9), respectively, at lag 0). Particles from soil and road dust and coal/oil combustion were not consistently associated with any of the outcomes. Although the correlation between soil derived PM2.5 and coarse particles was high, soil related PM2.5 did not show significant associations with the emergency room visits when all four PM2.5 sources were analysed in the same model. However, when soil related PM2.5 was analysed without other sources of PM2.5, the observed association among the elderly was very similar (2.2% (95% CI −0.04 to 4.4) for soil related PM2.5 at lag 0) to that observed with coarse particles.

{kind=link}
{kind=link}
The lagged effects of pollutants on asthma were larger among children than among adults and the elderly. These differences reached statistical significance (p<0.05) for the coefficients of ultrafine particles (lag 4), NO2 (lag 4) and traffic related PM2.5 (lag 3 or 4) for adults and the elderly, and for accumulation mode particles (lag 3) only among the elderly. In contrast, differences between age groups in the current day effects of pollutants reached statistical significance only for long range transported PM2.5 between children and the elderly.
As a sensitivity analysis, we used the 98th percentile cut point to estimate whether the extreme values of pollutants affected the results. To better control for the effect of temperature, we ran the analyses using the same lag for temperature and the pollutant in the models. To examine the effect of the chosen smooth function, we also ran some of the analyses using the generalised linear model with natural cubic splines with 40 degrees of freedom. We also tested 20, 30, 35, 40 and 45 degrees of freedom for the time trend. In these analyses only minor changes in the results were observed.
When asthma and COPD were analysed separately, the associations of PM2.5, accumulation mode particles and NO2 with COPD were stronger than those with asthma (tables S2 and S3 online). Otherwise, the associations were similar for COPD and asthma.
An indicator variable for pollen episodes was included in all models. Leaving it out of the models increased slightly the effect of ultrafine particles on asthma visits of children (7.0% (95% CI 2.69 to 11.4) at lag 4). Overall controlling for pollen episodes had a minor effect on the other results.
DISCUSSION
In the current study, hospital emergency room visits for asthma among children were associated with smaller particle size fractions (<250 nm), gaseous air pollutants and traffic related PM2.5 at longer lags. In contrast, PM2.5, especially from long range transport and traffic, coarse particles and gaseous pollutants had a more immediate effect on the pooled asthma–COPD visits of the elderly. Associations in general were weaker among adults, but immediate effects of accumulation mode and coarse particles were also observed for adults. Our results are consistent with previous studies showing associations of particulate and gaseous pollutants with respiratory conditions.2–5 ,15–17 However, there are no previous studies on the effects of more accurately size fractionated particles or source specific PM2.5 on hospital emergency room visits.
The observed associations between air pollution and asthma visits among children were lagged by 3–5 days whereas the associations among adults and elderly were more immediate. Only a few studies have determined the effects of air pollutants with time lags longer than 2 days.3 ,15 ,17 However, their results support the current finding of the lagged effect among children. On the other hand, the acute effect of larger particles and gaseous pollutants is consistent with more extensive literature.4 ,16 ,18 The mechanism leading to the lagged effect could partly be explained by inflammation in the alveolar region of the lung caused by the smaller particles in the pollutant mixture.6 Particles in the ultrafine size fraction have been shown to be able to penetrate into the alveolar region of the lung and, in particular, in persons suffering from asthma and COPD the deposition efficiency is increased.19 The immediate effect observed among older people, on the other hand, could be a result of irritation and inflammation caused by particles deposited on the larger airways. Larger particles, such as coarse particles, and other particles larger than 1 μm, deposit mainly on the tracheobronchiolar regions,20 which could lead to the observed more immediate exacerbations of the diseases. Furthermore, ultrafine particles penetrate poorly indoors. As elderly people spend more time indoors, they possibly become exposed to smaller particles to a lesser degree than children. Another possible explanation for the lagged effect is behavioural reasons. Time needed for the exacerbation to become severe enough to lead to an emergency room visit can be several days. This time lag can be modified by medication use, which can differ between children and adults.
The observed associations with NO2, ultrafine particles, CO and traffic related PM2.5 suggest that traffic related pollutants, partly of unknown character, are the main air pollutants associated with exacerbation of asthma among children.21 In the current study, in common with several past studies,3 ,5 NO2 was found to be a strong and independent predictor of the asthma emergency room visits of children. However, there is little toxicological evidence supporting a causal role of NO2 at current levels.22 Ultrafine particles did not have independent association with asthma, which suggests that NO2 is a better marker of traffic related pollution23 than ultrafine particles, as NO2 is more stable in the atmosphere.
We used ambient air pollution concentrations measured at fixed outdoor monitoring sites to estimate variations in personal exposure. This estimate has been shown to be good in Helsinki for PM2.5.24 However, ultrafine particles have greater spatial variability and poorer penetration from outdoors to indoors than PM2.525 and therefore ultrafine particle concentrations, such as NO2 and possibly CO, are probably mostly indicators of daily variation in the traffic related air pollutants. However, in Helsinki, there is a fairly good correlation between different outdoor ultrafine particle measurement sites.26 Therefore, the exposure assessment for children, who spend more time outdoors than elderly people, is probably more accurate. We have also observed a correlation of 0.5 between total particle counts measured at central sites and indoors at night-time.27 The possible causal role of ultrafine particles is also supported by several toxicological studies.28
Other potentially important causal factors in traffic related air pollution are polyaromatic hydrocarbons and transition metals, such as copper (Cu) and iron (Fe)29 that contribute to the oxidative capacity of particles by increasing the formation of reactive oxygen species. Reactive oxygen species have the ability to cause pulmonary inflammation and exacerbation of lung diseases.30 However, there is a clear need to identify more accurately the causal components in traffic related air pollution, for example the compounds from diesel and gasoline vehicle emissions that we were not able to separate in our source apportionment. This was due to the lack of marker data for these compounds. The method we used for particle source apportionment, the EPA PMF, has been found to be comparable with other methods.31
For the first time, we were able to analyse the associations between respiratory emergency room visits and more accurately size fractioned particulate air pollution. We observed weaker associations of asthma with nucleation mode particles than with Aitken mode particles. The reason for this different behaviour of different particle size fractions may be that they differ in dynamics. Nucleation mode is mainly formed via atmospheric nucleation,32 but also partly directly derives from traffic emissions. Nucleation mode particles have high short term peak concentrations, so they can make significant contribution to short term exposure to inhalable particles. However, lifetime of nucleation mode particles is short, which may partly explain the observed weaker associations. At the same time, peak number concentrations of Aitken mode are smaller, but these particles are always present.
In summary, particulate and gaseous air pollution had a lagged association with asthma hospital emergency room visits among children and a more immediate effect on asthma and COPD visits among the elderly. Effects among children were observed mainly with smaller particle sizes (<250 nm) and traffic related PM2.5, and among the elderly with larger particles, long range transported and traffic related PM2.5. Associations in general were weaker among adults. These findings suggest that mechanisms of the respiratory effects of air pollution and the responsible air pollutants differ by age group.
Acknowledgments
We thank National Research and Development Centre for Welfare and Health, Helsinki Metropolitan Area Council, Finnish Meteorological Institute, Aerobiology Unit of University of Turku and National Public Health Institute’s Infectious Diseases Register that provided the data used in this research.
REFERENCES
Supplementary materials
web only appendices 63/7/635
Files in this Data Supplement:
Footnotes
See Editorial, page 574
Tables S1, S2 and S3, figs S1 and S2, and supplementary data are published online only at http://thorax.bmj.com/content/vol63/issue7
Funding: The study was financially supported by the Centre of Excellence Programme 2002–2007 of the Academy of Finland (Contract 53307), the National Technology Fund (TEKES, Contract 40715/01) and the Ministry of Education (Graduate School in Environment Health SYTYKE).
Competing interests: None.