Article Text

Abstract
Background and aims—Recent studies have shown that the age-specific seroprevalence of H pylori infection parallels hepatitis A (HAV), suggesting similar modes of transmission. The aim of this study was to investigate the seroepidemiology ofH pylori and HAV in the same setting.
Patients—A sample of 705 resident subjects (273 men, age range 1–87 years, median 50) who attended the outpatient medical centre of the rural town of Cirò, Southern Italy (11 000 inhabitants) for blood testing were recruited.
Methods—All subjects completed a structured questionnaire. A serum sample was drawn from each subject and assayed for H pylori IgG by a validated in house enzyme linked immunosorbent assay. Antibodies to HAV were determined in 466 subjects (163 men, age range 1–87 years, median 49). A measure of agreement between H pylori and HAV seropositivity, the κ statistic, was used.
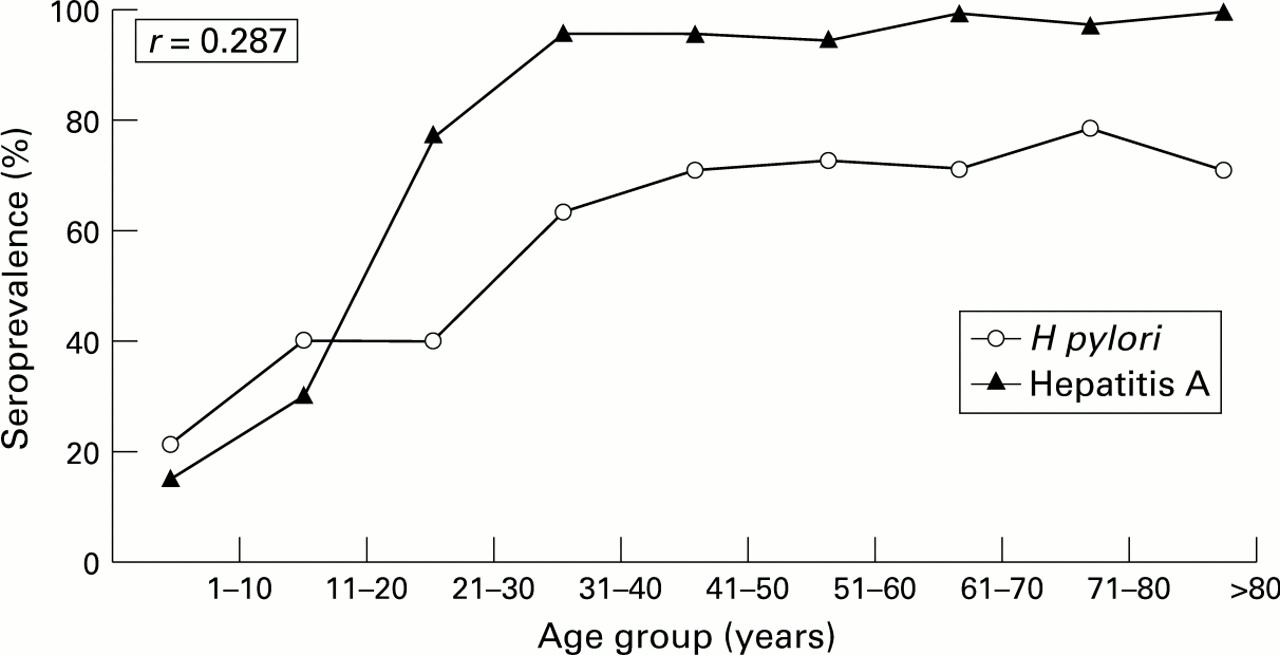
Results—Overall, 446 (63%) subjects were seropositive for H pylori. Of the 466 subjects screened for both H pylori and HAV, 291 (62%) were seropositive for H pylori and 407 (87%) for HAV. Cross-tabulation of these data showed that 275 (59%) were seropositive and 43 (9%) seronegative for both H pylori and HAV, 16 (3%) were seropositive for H pylori, and 132 (28%) were seropositive for HAV (OR = 5.6, CI 3 to 10). There was a parallel, weakly correlated (r = 0.287) rise in the seroprevalence of the two infections with increasing age. However, the agreement between H pylori and HAV seropositivity was little better than chance (κ = 0.21) and in those aged less than 20 years it was worse than chance (κ = –0.064). Furthermore, multiple logistic regression analysis did not show any risk factor shared by both infections.
Conclusions—The correlation between H pylori and HAV reflects the age-specific seroprevalence of both infections rather than a true association. This study provides evidence against a common mode of transmission of H pylori and HAV.
- Helicobacter pylori
- hepatitis A
- serology
- epidemiology
- faecal-oral transmission
Statistics from Altmetric.com
Helicobacter pylori infection is probably the most common chronic bacterial infection in humans. In particular, the prevalence of the infection varies from about 50% of adults in developed countries to nearly 90% in developing countries.1 Overcrowding and poor socioeconomic conditions during childhood appear to be risk factors for H pyloriinfection.2 ,3 These data are consistent with the suggestion that the infection may be acquired in early life and that person to person contact plays an important role in its transmission. The recent isolation of H pylori from faeces, dental plaque, and saliva further supports the possibility of an oro-oral or faecal-oral route of transmission.4-6 This emerging pattern of the epidemiology of H pylori infection seems very similar to that of hepatitis A virus (HAV). HAV is known to be spread by faecal-oral contact and has a high incidence in populations with poor standards, poor hygiene practices, and low socioeconomic level. Some authors have shown that the age-specific seroprevalence ofH pylori infection and HAV tend to overlap7 ,8 but this finding has not been confirmed by others.9 ,10 Furthermore, limited research has been designed to identify potential risk factors associated with the two infections. A large national multicentre study of a population who underwent endoscopy showed a prevalence rate of 78% of H pylori infection in southern Italy (our district) compared with 61% in northern Italy,11 which may have been related to the well documented low socioeconomic status in southern Italy during the period 1950–1970.
The aim of this study was to investigate the seroepidemiology ofH pylori infection and HAV in a large series of subjects from a geographically defined rural area of southern Italy and to assess the agreement between H pylori infection and HAV seropositivity in the same setting.
Methods
SUBJECTS
The study population consisted of 705 resident subjects (273 men; age range 1–87 years, median 50) who attended the medical outpatient centre of Cirò for blood testing between January and September 1995. All consecutive subjects who attended the public referral centre on two days of the week (Tuesday and Friday) were eligible for the study. More than 90% of the eligible subjects agreed to participate. Cirò is a rural town in southern Italy, Crotone Province, with a resident population of approximately 11 000.
The blood pressure of each subject was measured and a blood sample was taken. Serum was separated and stored at –20°C until tested. One observer (GP) used the same mercury sphygmomanometer throughout the study.
QUESTIONNAIRE
All subjects were interviewed by means of a structured questionnaire for general demographic details, height, weight, and current and childhood socioeconomic circumstances. History of cardiovascular disease, high blood pressure, diabetes, dyspepsia, peptic ulcer, smoking, and alcohol consumption were recorded and treated as dichotomous variables. Smoking habit was grouped according to age at starting smoking (never, <15, 15–20, >20 years) and lifetime cigarette consumption (pack-years) was calculated from the duration of smoking and normal daily consumption; likewise, alcohol consumption was grouped according to duration (<10, 10–20, 20–30, >30 years) and usual weekly intake (<150 g, 150–250 g, >250 g). The body mass index (BMI = weight (kg)/height (m2)) was calculated. Each subject’s occupation (or principal lifetime occupation if retired) and that of their father when the subject was aged about 10 years was classified as manual or non-manual. Years of school education were reported for each subject and coded into five categories (none, 1–5, 6–8, 9–14, >14 years). The current and childhood social class of each subject was grouped into two main categories (low and middle) according to the annual household income. The number of siblings sharing a bed/bedroom and the ratio of the number of persons per room (excluding kitchen and bathroom) were separately considered as a quantitative index of housing density during childhood and used in the analyses as continuous untransformed variables. Childhood possession of a bathroom, indoor toilet, and refrigerator was checked. The hot water supply and presence of household pets during childhood were also considered.
The same interviewer (GP) administered all the questionnaires.
DETERMINATION OF H PYLORI AND HAV STATUS
IgG antibodies to H pylori were measured in duplicate by an in house enzyme linked immunosorbent assay (ELISA) using a crudeH pylori sonicate as previously described.12Levels (optical density, OD) of IgG were categorised as seropositive and seronegative for H pylori according to a chosen cut off value (0.600 OD) which gave 97% sensitivity and 91% specificity when using microscopy (Giemsa staining) and the rapid urease test as the gold standard.12 To avoid a loss of accuracy in children under 18 years13 we standardised the IgG ELISA in a control group of 50 children who underwent endoscopic examination of the upper gastrointestinal tract with histological examination and the rapid urease test for H pylori. The optimal cut off point was lower (0.400 OD) and a similar sensitivity (96%) and specificity (88%) were obtained (unpublished data).
A solid phase competitive ELISA for the detection of antibodies to HAV antigen (Behring Diagnostic Inc, Westwood, Massachusetts, USA) was used to determine the HAV status in a random sample of 466 (66%) subjects (163 men) of median age 49 years (range 1–87).
MEASUREMENT OF SERUM LEVELS OF CHOLESTEROL, TRIGLYCERIDES AND GLUCOSE
In a subset of 528 (75%) subjects (171 men) of median age 53 years (range 1–87) serum levels of fasting cholesterol, triglycerides, and glucose were also measured and used in the analyses as continuous untransformed variables.
STATISTICAL ANALYSIS
The seroprevalence of H pylori infection and HAV was separately analysed in relation to all considered variables. The Mantel-Haenszel χ2 test was used to examine the relation of the two infections with age and sex. Odds ratio (OR) of H pylori infection or HAV, given the presence of a particular characteristic, was used as the measure of association. Data were given together with 95% confidence intervals (CI). Adjusted ORs were estimated by multiple logistic regression analysis. The relation between seroprevalence of H pylori infection and HAV was evaluated by means of the Spearman’s test, χ2 test with continuity correction, OR, and κ statistic. The κ statistic, a measure of the agreement between two observers or tests, ranges from –1 to 1 with 1 indicating perfect agreement, 0 indicating the agreement expected on the basis of chance alone, and values between 0 and 0.4 a poor to fair agreement.14
Results
Seropositivity was found in 63% (446/705) and 87% (407/466) of the subjects for H pylori and HAV, respectively. The seroprevalence of H pylori and HAV increased significantly with age and did not differ according to sex (table 1). There was a parallel, weakly correlated (r = 0.287) rise in the seroprevalence of the two infections with increasing age (fig 1). Cross-tabulation of data showed that 275 subjects (59%) were seropositive and 43 (9%) were seronegative for bothH pylori and HAV, 16 (3%) were seropositive for H pylori, and 132 (28%) were seropositive for HAV (χ2 = 34.24, OR = 5.6, CI 3 to 10) (fig 2). The age-adjusted OR for an H pylori positive subject being HAV positive was 2.9 (CI 1.4 to 5.8) and for an HAV positive being H pylori positive was 2.5 (CI 1.2 to 5). However, the agreement between H pylori and HAV seropositivity was little better than chance (κ = 0.21) and, when assessed in the 44 subjects (three seropositive and 24 seronegative for both infections, 10 seropositive for H pylori and seven seropositive for HAV) aged between one and 20 years (median 10), it was worse than chance (κ = –0.064) (fig 2).
Number (%) of subjects seropositive for H pylori and hepatitis A virus (HAV) by age and sex

: Seroprevalence of H pylori and hepatitis A virus in the 466 subjects tested for both infections by age group: 1–10 years (n = 24), five H pylori positive, four HAV positive; 11–20 years (n = 20), eight H pylori positive, six HAV positive; 21–30 years (n = 62), 24 H pylori positive, 48 HAV positive; 31–40 years (n = 57), 36 H pylori positive, 55 HAV positive; 41–50 years (n = 76), 54 H pylori positive, 73 HAV positive; 51–60 years (n = 81), 58 H pylori positive, 77 HAV positive; 61–70 years (n = 89), 63 H pylori positive, 88 HAV positive; 71–80 years (n = 43), 33 H pylori positive, 42 HAV positive; >80 years (n = 14), 10 H pylori positive, 14 HAV positive.

{kind=link}
{kind=link}
: Seropositivity for H pylori and hepatitis A virus in the 466 subjects tested for both infections. The strength of agreement is calculated by κ statistic analysis according to Landis and Koch15 and shown in (A) the overall population and (B) in the subset of 44 subjects aged between 1 and 20 years. The seroprevalence of H pylori and hepatitis A virus was 62% and 87%, and 29% and 23%, respectively, in the two groups.
Tables 2 and 3 show current and childhood characteristics of subjects who were seropositive or seronegative for each infection. Almost all variables were associated with increased or decreased risk of the infections by univariate analysis. However, when adjusted for age and sex only dyspepsia (OR 1.72, CI 1.23 to 2.41), peptic ulcer (OR 1.95, CI 1.12 to 3.4), occupation (OR 0.75, CI 0.59 to 0.93), crowding (OR 1.11, CI 1.01 to 1.21), and number of siblings (OR 1.09, CI 1.01 to 1.18) remained significantly associated with H pyloriwhile occupation (OR 0.49, CI 0.26 to 0.93), number of siblings (OR 1.36, CI 1.09 to 1.7), and possession of a refrigerator (OR 4.8, CI 1.27 to 18) were associated with HAV infection (table 4). Furthermore, by mutual adjustment of these variables with each other it was shown that no risk factor was shared by both infections (table 4). In particular, dyspepsia (OR 1.58, CI 1.1 to 2.27) and occupation (OR 0.72, CI 0.57 to 0.91) were independently associated with H pylori, and number of siblings (OR 1.32, CI 1.05 to 1.66) and possession of a refrigerator (OR 5.6, CI 1.29 to 24.3) with HAV (table4). The age at starting smoking, and lifetime and usual daily cigarette and alcohol consumption were associated with neither H pylori nor HAV infection.
Characteristics of the study population by seropositivity for H pylori and hepatitis A virus
Childhood socioeconomic features of the study population by seropositivity for H pylori and hepatitis A virus
Relevant independent variables and adjusted odds ratios (ORs) (95% confidence intervals) for seropositivity for H pylori and hepatitis A virus (HAV)
The OR for peptic ulcer, cardiovascular disease, and alcohol consumption associated with HAV could not be calculated because there were insufficient cases among the younger seronegative subjects of mean age 20 (17) years (table 2).
Discussion
In this study the prevalence of antibodies to H pylori and HAV and the associated risk factors have been determined in a large series of residents in a small rural area of southern Italy. Our results showed a high seroprevalence of both infections and a strong relation with age. The last finding is a well known epidemiological feature, mostly considered as a cohort birth effect.16 ,17 The older subjects were born at a time when the risk of infection in childhood was higher than in those born later and therefore the high prevalence of antibody titres in elderly people should reflect their greater exposure to the infection in their early years. In fact, HAV and H pylori are predominantly acquired at a young age and rarely in adult life.2 ,3 ,18Furthermore, HAV is known to be spread by faecal-oral contact and the faecal-oral dissemination is a proposed mode of transmission of H pylori infection.19 From these data we have postulated that, if the mode of transmission of HAV and H pylori was the same, we would expect a higher association of the two infections in the same population, even early in life. Primary analysis of our data showed a fair unadjusted correlation between the seroprevalence curves of HAV and H pylori (r= 0.287) and an overall concordance rate of seropositive and seronegative results of 68% (χ2 = 34.24). However, the χ2 statistic is not a good measure of the degree of association, particularly when dealing with highly prevalent variables. The κ statistic is a more suitable method for ascertaining the strength of agreement in this situation and this revealed a very weak association (κ = 0.21) between the two infections. According to the current epidemiological knowledge—that is, cohort birth effects and socioeconomic improvement—the seroprevalence of H pyloriand HAV in the first two decades was significantly lower than that in the older age group. Nevertheless, the first 20 years of life is considered to be the most critical period for the acquisition of infection.2 ,3 When we applied κ statistic analysis in this setting there was no agreement between the seroprevalence of HAV and H pylori (κ = –0.064). These findings are in contrast with the hypothesis of a common mode of transmission of the two infections. Furthermore, it is conceivable that if the two infections were associated, they would share a number of risk factors. In our study the seroprevalence of H pylori and HAV was separately analysed in relation to a number of variables including crowding (density of living, number of siblings, sharing a bed) and other specific socioeconomic indicators. By means of multiple logistic regression analysis we were not able to find any risk factor shared by both infections. We showed that dyspepsia and a manual occupation were independent risk factors for H pylori, and that the number of siblings and the possession of refrigerator were risk factors for HAV.
Our findings are in agreement with those of Hazell et al 10 and Lindkvist et al 20 but contrast with those of Sathar et al,7 Graham et al,8 and Al-Moagel et al.21 In the last three studies it was found that the prevalence of H pylori paralleled that of HAV, but Graham et al and Al-Moagel et al used unpaired serum samples from two different groups of subjects. Our data support the view that the correlation betweenH pylori and HAV is a result of the high age-related seroprevalence of the two infections and provide no evidence thatH pylori and HAV share a common mode of transmission.
Acknowledgments
The authors thank Dr Dino Vaira, University of Bologna, for the generous supply of H pylori sonicates and for his helpful criticism and advice, and Dr Domenico Monizzi, ASL N.5 Crotone, for providing facilities to perform medical interviews and serum sample collection.
This work was presented at the Annual Meeting of the American Gastroenterological Association, May 19–22 1996, San Francisco, California, and published as an abstract inGastroenterology 1996; 110: A181.