Article Text

Abstract
Objectives To estimate the risk of surgery for subacromial impingement syndrome (SIS) in relation to occupational exposures, lifestyle factors and diabetes mellitus.
Methods We conducted a case–control study nested in a register-based cohort study of the Danish working population. For each of 3000 first-time cases of surgery for SIS, two age-matched and sex-matched controls were drawn. Cases and controls received a questionnaire on job history and other factors. Job histories were combined with a psychosocial job exposure matrix (JEM) and the updated Shoulder JEM, which provided exposure intensities on measurement scales. Ten-year cumulative exposures to upper arm elevation >90°, repetitive shoulder movements, forceful shoulder exertions and hand–arm vibrations (HAVs) were estimated. We used conditional logistic regression.
Results There were 5396 persons (60%) who answered the questionnaire. For occupational mechanical exposures, the adjusted OR (ORadj) ranged from 1.9 (95% CI 1.5 to 2.5 for HAVs) to 2.5 (95% CI 1.9 to 3.5 for force) among men and 1.7 (95% CI 1.2 to 2.5 for HAVs) to 2.0 (95% CI 1.3 to 2.9 for force) among women. No statistically significant associations were found for occupational psychosocial factors. Body mass index (BMI) and pack-years of smoking showed ORadj up to 2.0. Diabetes mellitus showed ORadj of 1.5 (95% CI 1.1 to 2.2) for men and 2.2 (95% CI 1.4 to 3.4) for women.
Conclusions Our findings add to the evidence of an increased risk of surgery for SIS in relation to occupational cumulative mechanical exposures, even when an increased risk in relation to BMI, smoking and diabetes mellitus is taken into account.
- Body mass index
- diabetes mellitus
- occupational exposures
- shoulder disorder
- smoking
- leisure time shoulder intensive sports.
Statistics from Altmetric.com
- Body mass index
- diabetes mellitus
- occupational exposures
- shoulder disorder
- smoking
- leisure time shoulder intensive sports.
What this paper adds
Little is known on occupational risk factors for surgery for subacromial impingement syndrome (SIS).
This study corroborated a relationship between cumulative occupational mechanical exposures and surgery for SIS (and provided intensity estimates on measurement scales), while occupational psychosocial factors were not related to the outcome.
Higher body mass index, smoking and diabetes mellitus were associated with an increased risk.
Introduction
It is increasingly well-established that clinically diagnosed subacromial impingement syndrome (SIS) is related to occupational mechanical shoulder exposures.1–3 We have recently conducted two studies that indicated that surgery for SIS shares these risk factors.4 5 In one of our previous studies that focused on cumulative mechanical exposures—a nationwide register-based cohort study—we did not have information on occupational psychosocial factors and lifestyle factors, which might have confounded the results.5 Furthermore, we have not previously taken diabetes mellitus into account.
Our previous findings based on the Musculoskeletal Research Database at the Danish Ramazzini Centre indicated no associations between occupational psychosocial factors and surgery for SIS.4 Contradictory results have been reported for the association with clinically diagnosed SIS,1 2 6 whereas associations with shoulder pain have been reported in several studies.7 These findings suggest that occupational psychosocial factors may be more closely related to shoulder symptoms than to pathological changes.8
Regarding lifestyle factors, recent reviews have pointed to a high body mass index (BMI) as a potential risk factor for tendinopathy across anatomical regions.9 10 Two case–control studies of surgically treated patients with SIS have reported positive associations with a high BMI,11 12 but in one of these studies, the results were reported in an unclear way (there seems to be no reference group),11 and studies of clinically diagnosed SIS have not found this relationship.2 4 6 13–18 Based on theories on pathogenic mechanisms, smoking may be a risk factor for SIS (nicotine is a vasoconstrictor and carbon monoxide decreases cellular oxygen tension levels, which decreases oxygen delivery to the tissues, and collagen deposition in the repair of surgical wounds is decreased in relation to smoking),19 but this has not been supported in previous studies of surgically treated4 18 and clinically diagnosed SIS,13 14 16 17 20 except for the subgroup with degenerative rotator cuff tears.19 21 Three studies have indicated a relationship with diabetes mellitus (in particular type I),16–18 while three studies that were based on overlapping study populations did not show a clear tendency.2 6 15 One study found no statistical significant association for leisure time physical activity but did not focus on shoulder intensive sports.17
In our previous nationwide cohort study, we used 10-year cumulative estimates of occupational mechanical exposures and found exposure–response relationships with ORs increasing to around 2.5 The cumulative exposure estimates were calculated using an expert-based shoulder job exposure matrix (the Shoulder JEM), which could not be directly translated to measurement scales.5 Exposure intensities on measurement scales would have been preferable to promote translation of the exposure–response results into practice, for example, to convert measured exposure intensities to risk estimates in connection with labour inspection visits. Exposure–response results on measurement scales would also facilitate future meta-analyses.1 We have recently upgraded the expert-based Shoulder JEM with exposure estimates on measurement scales for upper arm elevation and repetitive shoulder movements,22 and we used the upgraded JEM in the present study.
The aim of this study was to estimate the risk of surgery for SIS in relation to cumulative occupational mechanical exposures, occupational psychosocial factors, lifestyle factors and diabetes mellitus. We hypothesised that we would find exposure–response relationships for occupational mechanical exposures, but not occupational psychosocial factors, and that BMI, smoking and diabetes mellitus would be related to surgery for SIS.
Materials and methods
Design and population
We conducted a case–control study nested within a cohort study of the entire Danish working population (n=2 374 403).5 The cohort included all persons born in Denmark, except Greenland, between 1 January 1933 and 31 December 1977, with at least 5 years of full-time employment between 1 January 1993 and 31 December 2007; those who underwent shoulder surgery in the period 1 January 1996 to 31 December 2002 or before reaching 5 years of full-time employment in the period 1 January 2003 to 31 December 2007 were excluded.5 For the purpose of this study, we also excluded those who died, moved to Greenland, emigrated or disappeared before 14 August 2010, those who had address protection or protection against inquiries in connection with scientific studies on 14 August 2010 and those who underwent shoulder surgery before 1 January 2007. Within the cohort, we identified all cases of first-time surgery for SIS in 2007 and 2008. The outcome was defined as surgery performed under a main diagnosis in the International Classification of Diseases, 10th revision, groups M19 or M75.1–M75.9, without a subordinate diagnosis of M75.0 (adhesive capsulitis of shoulder) and registered with a relevant Danish Nordic Medico-Statistical Committee shoulder and upper arm surgery code (KNBA, KNBE, KNBF, KNBG, KNBH, KNBK, KNBL or KNBM). For 3000 randomly selected cases, we randomly selected two controls—matched on sex and date of birth—among those who did not fulfil the case criteria on the index date (date of surgery of the case). Thus, a control could be sampled more than once and even become a case later on (risk-set sampling).
The Danish Data Protection Agency approved the study (j. no.: 2012-41-1187). In Denmark, register and questionnaire studies do not require approval by the Committee System on Biomedical Research Ethics (request no. 130/2009).
Sample size calculation
To show an OR of 1.4 (p<0.05, power 0.8, probability of exposure among controls 0.5, correlation of exposure between pairs in case–control sets 0.2), inclusion of 699 cases would be required with two-to-one sampling (STATA sampsi_mcc). Assuming that 60% would participate, we decided to sample 3000 case–control sets, which would allow exposure–response analyses using categorised data as well as separate analyses for men and women.
Collection of questionnaire data
A postal questionnaire was sent to cases and controls followed by a maximum of three reminders during October 2010 through January 2011. The questionnaire could be answered using the postal paper version or an identical internet version. The questionnaire was designed to be equally relevant for cases and controls by focusing on general health without mentioning the shoulder in the information material. We did not show pictures of work situations on the front page to minimise the influence of occupational exposures on the decision to participate.
Cumulative occupational mechanical exposures
In the questionnaire, we asked for up to six job titles, which each person had held for the longest time in the period 1997–2008 and for the calendar period with each of these job titles. A research assistant transformed all self-reported job titles into occupational titles in the Danish version of the International Classification of Occupations from 1988 (D-ISCO 88), and two occupational physicians (PF and SWS) checked the transformations and performed necessary corrections. Corresponding D-ISCO 88 codes were added (see ‘Occupational psychosocial factors below’).
Individual occupational titles were linked to the Shoulder JEM, which cross-tabulates occupational titles and occupational mechanical exposures.4 5 22 Of note, this procedure was different from the procedure in our previous nationwide cohort study, where we only had access to registered D-ISCO 88 codes.5 The construction of the Shoulder JEM has been described previously.4 5 22 In brief, the Shoulder JEM contains 172 job groups with expected homogeneous shoulder exposure patterns.4 5 The original JEM was based on five experts’ ratings.4 5 For upper arm elevation >90° and repetitive shoulder movements, we recently converted the expert ratings to measurement scales by calibration against technical measurements and labelled the calibrated mean exposure intensities ‘predicted measured job exposures’.22
We estimated cumulative occupational mechanical exposures for a 10-year time window with a 1-year lag time up to the index year (year of surgery of the case). As previously, we expressed the cumulative exposure estimates in accordance with the pack-year concept of smoking.5 When calibrated into ‘predicted measured job exposures’, one arm-elevation-year adds 4.8 min to the background duration of 2.3 min per day with the arm elevated >90° and one repetition-year adds 25°/s to the background median angular velocity of upper arm movements of 27°/s per day.22 We also used a shoulder load variable, which represented upper arm elevation >90°, repetitive shoulder movements and forceful shoulder exertions, either individually or in different combinations.4 5 Furthermore, we recalculated the shoulder load variable by dividing the highest exposure category into a category, which represented one high exposure only and a category that represented two or more high exposures, that is, combined exposures.
Occupational psychosocial factors
In the questionnaire, we asked about occupational psychosocial factors for the job held for the longest time in the period 1997–2008. The occupational psychosocial factors were assessed by questions on job demands (four items), job control (two items) and social support from leaders and/or colleagues (six items) based on the short version of the Copenhagen Psychosocial Questionnaire.23 Each item was scored from 1 (best) to 5 (worst), and global scores were calculated as the mean for each scale.24 To minimise the potential for recall bias and to avoid the associated ‘triviality trap’,25 we constructed a psychosocial JEM by grouping the participants according to occupational titles and then calculating median exposures.24 The psychosocial JEM was sex specific. If less than 10 participants of the same sex held a given occupational title, median exposures within the same four-digit, three-digit or two-digit D-ISCO 88 code were calculated; 73% of the men and 84% of the women were placed in a group based on four-digit D-ISCO 88 codes. Job demands (median for men: 2.9, median for women: 3.1), job control (median for men: 2.6, median for women: 2.9) and social support (median for men: 2.5, median for women: 2.5) were dichotomised based on sex-specific medians.24 Based on the dichotomised demand and control variables, we constructed a job strain variable (four categories): low strain (low demands and high control), passive (low demands and low control), active (high demands and high control) and high strain (high demands and low control).24
Lifestyle factors and diabetes mellitus
We obtained questionnaire information on present weight and height, smoking history and leisure time shoulder intensive sports for ≥2 hours per week in the period 2000–2005. BMI was calculated as weight divided by height squared (kg/m2). Pack-years of smoking were calculated as number of years with regular smoking times average daily smoking intensity (standardised to cigarettes per day) divided by 20 cigarettes per pack. Leisure time shoulder intensive sports was categorised as <2 hours per week, ≥2 hours per week of activity without overhead arm motion (running, football, cycling, boxing, strength training and fitness) and ≥2 hours per week of activity with any overhead motion (swimming, tennis, squash, badminton, basketball, volleyball and handball). The questionnaire contained the question: ‘Do you have diabetes mellitus?’ with the response options no, yes and do not know. The answers no and do not know were collapsed as no in the analyses.
Other covariates
We obtained questionnaire information about education level, which we used as a proxy for socioeconomic status.26 A priori, we decided only to include education level in supplementary analyses to avoid overadjustment of our main results due to expected high correlations with occupational mechanical exposures. We used register information on region of residence to account for regional variations in surgery rates.
Analyses
Two-by-two correlation analyses were performed between the continuous cumulative occupational exposure variables (arm-elevation-years, repetition-years, force-years, hand–arm vibration (HAV)-years). Missing data were considered missing at random, and to minimise the risk of bias due to missing data and increase statistical power, we used single regression imputation to fill out missing values for occupational mechanical and psychosocial exposures, BMI, pack-years of smoking, leisure time shoulder intensive sports, diabetes mellitus and education level. The imputed values were predicted using all explanatory variables.27
The association between surgery for SIS and all explanatory variables was analysed using conditional logistic regression for men and women separately; the resulting ORs can be interpreted as incidence rate ratios since we used risk-set sampling.28 We expected the occupational mechanical exposures to be highly correlated and therefore a priori decided to include only one mechanical exposure variable (three categories) at a time in the adjusted models (the upper category was chosen to correspond to the upper category in our previous study of cumulative exposures and surgery for SIS).5 For each occupational mechanical exposure, we adjusted for occupational psychosocial factors (support (two categories) and job strain (four categories)), lifestyle factors (BMI (three categories), pack-years of smoking (four categories) and leisure time shoulder intensive sports (three categories)), diabetes mellitus (no/yes) and region of residence (five regions). In the models for occupational psychosocial factors, we adjusted for arm-elevation-years (three categories) together with lifestyle factors, diabetes mellitus and region of residence. In supplementary analyses, we controlled for education level (six categories). We repeated the analyses for shoulder load using the recalculated shoulder load variable. Furthermore, we performed complete case analyses. Finally, we repeated the analyses of the association between occupational mechanical exposures and surgery for SIS by replacing the ‘predicted measured job exposures’ with measured job exposures for the 36 job groups where these were available22 (when measured job exposures were available for both men and women, we used the sex-specific estimates (10 job groups)). All analyses were performed using Stata 13 (StataCorp LP, College Station, Texas, USA).
Results
Figure 1 shows the flow-chart. The proportion that responded was 60.1%. Among cases, 62.6% responded (59.5% among men and 65.3% among women) and among controls, 58.8% responded (54.2% among men and 63.5% among women). The mean age of men, who either did or did not respond, was 55.8 (SD 8.2) and 52.9 years (SD 8.9); the corresponding mean ages of women were 53.5 (SD 7.9) and 52.3 years (SD 8.5). One thousand five hundred and sixty-four (52.1%) case–control sets with at least one case and one control were available for analysis (701 case–control sets for men and 863 for women). Complete information for analyses was provided by 83.3% of the respondents, 85.3% of the men and 81.7% of the women; 70 respondents (1.4% of the men and 2.2% of the women) did not provide information on job history.
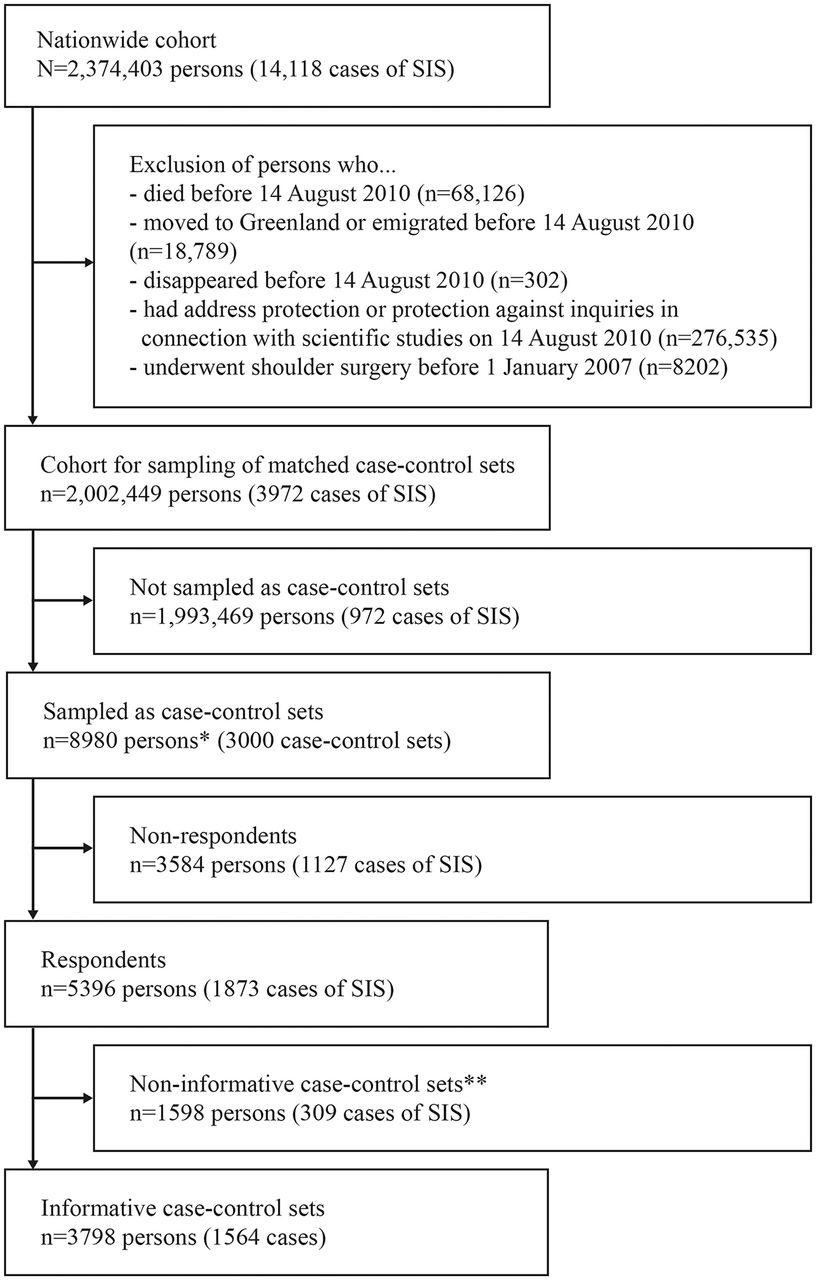
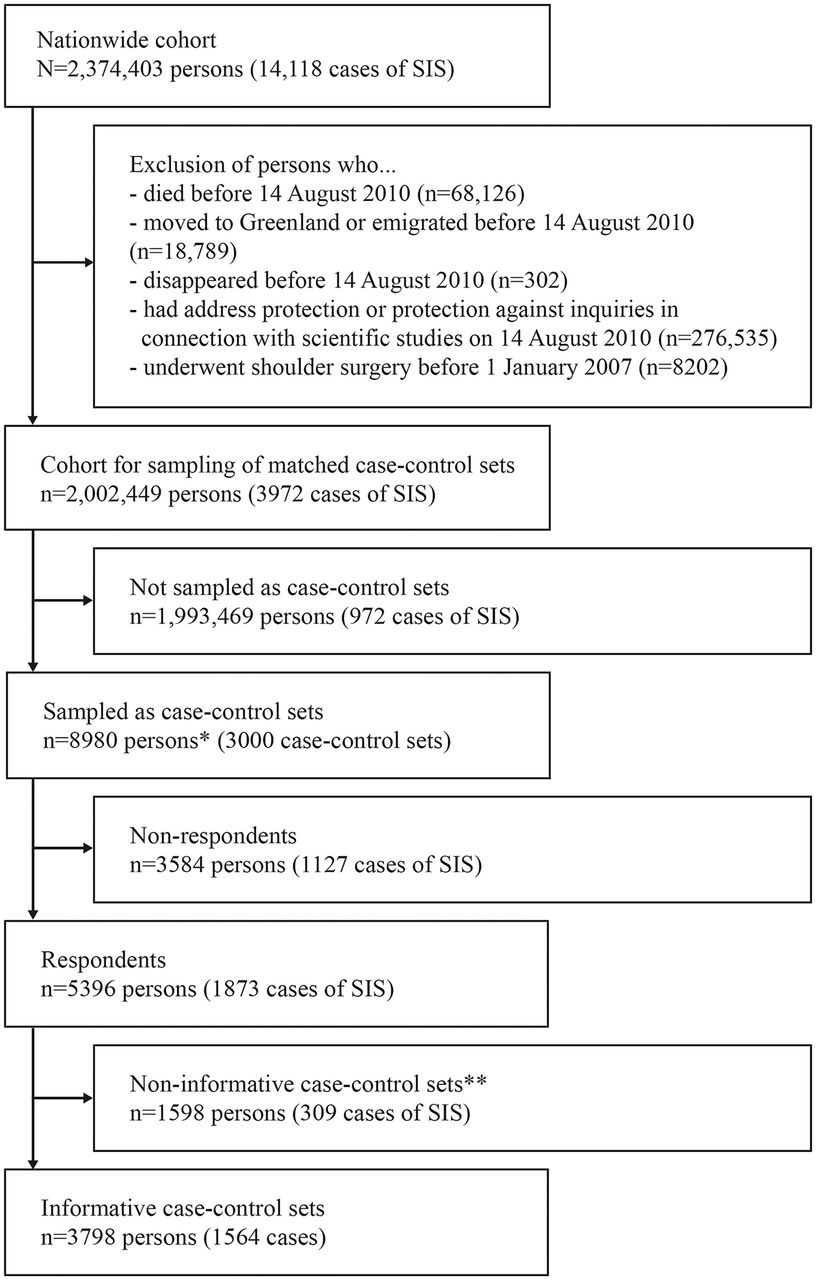{kind=link}
Flow-*/chart for the age-matched and sex-matched nested case–control study.* We sampled two controls per case, but a control could be included more than once and even be included as a case later on (risk-set sampling); 20 persons were represented twice.** Responding cases without any responding matched controls and responding matched controls without any responding case were excluded. SIS, subacromial impingement syndrome.
Table 1 shows characteristics of cases and controls according to arm-elevation-years. Two-by-two correlation coefficients between the cumulative occupational mechanical exposures were 0.7–0.8 for arm-elevation-years, repetition-years and force-years, and 0.5–0.6 for HAV-years in relation to the just-mentioned exposures.
Characteristics of male and female cases and controls according to cumulative occupational exposure to upper arm elevation >90°. Numbers in cells are percentages
Table 2 shows ORs for occupational exposures. With the exception of HAV-years >0, men and women had equal mean exposures within each exposure category. Exposure–response relationships were observed for arm-elevation-years, repetition-years, force-years and shoulder-load-years with maximum ORadj between 2.2 and 2.5 for men and between 1.7 and 2.0 for women; HAV-years >0 showed an ORadj of 1.9 for men and 1.7 for women. On a measurement scale, 10 arm-elevation-years correspond to a mean exposure intensity of 7.1 min per day ((10 arm-elevation-years*4.8 min per day/10 years)+2.3 min per day). Likewise, 10 repetition-years correspond to a mean exposure intensity of approximately 52°/s per day for 10 years ((10 repetition-years*25°/s/10 years)+27°/s). In supplementary analysis, adjusting for education level reduced the ORadj for all exposures; for example, for the highest category of arm-elevation-years, the ORadj was reduced from 2.3 to 1.8 (95% CI 1.3 to 2.4) for men and from 1.9 to 1.5 (95% CI 1.1 to 2.0) for women. Using the recalculated shoulder load variable, the ORadj for the highest exposure category was 2.5 (95% CI 1.9 to 3.3) for men and 2.0 (95% CI 1.4 to 3.0) for women. Complete case analyses yielded similar results as analyses including imputed values; for example, based on complete case analysis, the ORadj was 2.3 (95% CI 1.7 to 3.1) for the highest category of arm-elevation-years among men. Forty-three per cent of the study population had occupational titles for which we had measured job exposure estimates. When we repeated the analyses using measured job exposure estimates instead of ‘predicted measured job exposures’ when available, the ORadj for arm-elevation-years did not change much (for men the ORadj reached a maximum of 2.4 (95% CI 1.8 to 3.2) and for women 2.4 (95% CI 1.5 to 3.8)), while the ORadj for the highest category of repetition-years was 2.2 (95% CI 1.3 to 3.7) for men and 1.7 (95% CI 1.1 to 2.6) for women.
ORs obtained by conditional logistic regression analyses of surgery for SIS in relation to occupational exposures. Controls were individually matched on sex and date of birth. Men: n=1675, women: n=2123
Table 3 shows ORs for lifestyle factors and diabetes mellitus. We found statistically significant positive associations for BMI, pack-years of smoking and diabetes mellitus for both men and women, but for women the ORadj decreased slightly between the two highest smoking categories. Since a high BMI may be a part of the causal pathway leading to diabetes mellitus, we repeated the analyses without adjusting for BMI, which increased the ORadj for diabetes mellitus to 1.7 (95% CI 1.2 to 2.4) for men and 2.6 (95% CI 1.7 to 4.0) for women. In supplementary analyses, adjusting for education level did not change the ORadj for BMI, pack-years of smoking and diabetes mellitus (results not shown). No differences were found between ORadj obtained including imputed values and using complete case analyses (results not shown).
ORs obtained by conditional logistic regression analyses of surgery for SIS in relation to lifestyle factors and diabetes mellitus. Cases and controls were individually matched on sex and date of birth. Men: n=1675, women: n=2123
Discussion
In this age-matched and sex-matched nested case–control study of surgery for SIS, we found exposure–response relationships for occupational cumulative exposures to upper arm elevation >90°, repetitive shoulder movements and forceful shoulder exertions. Positive associations were also found for exposure to HAVs. For psychosocial factors, no statistically significant associations were found. Exposure–response relationships were found for BMI and pack-years of smoking, and positive associations were found for diabetes mellitus.
An important strength of the study was that we used JEMs to estimate occupational mechanical and psychosocial exposures, thus minimising the risk of recall bias.29–31 Additionally, we were able to control for and evaluate the effects of occupational psychosocial factors, lifestyle factors and diabetes mellitus, which were not included in our previous cohort study.5 Slightly more cases than controls participated (62.6% vs 58.8%). We consider exposure-related selection into the study to be of minor importance because of the quite satisfactory proportions that participated among both cases and controls (with minor differences with respect to age and sex distribution), and our efforts to ensure that the questionnaire and the information material would be equally relevant, irrespective of exposure level. As cases and controls were matched on date of birth and we used conditional logistic regression to account for the matching, age cannot confound the association between our explanatory variables and surgery for SIS. Moreover, the results corresponded closely to the nationwide register-based cohort study,5 in which the present study was nested, where non-response bias was not an issue.
The association between occupational mechanical exposures and surgery for SIS in this case–control study supports our previous findings, in which ORadj of up to 2.0 were found using similar exposure categories.5 This indicates that the results in our previous cohort study were not confounded by occupational psychosocial factors, lifestyle factors and diabetes mellitus. Using the upgraded Shoulder JEM,22 we were able to translate 10-year cumulative exposure estimates for arm elevation and repetition to mean exposure intensities on measurement scales. Exposure–response relationships on measurements scales can be used in practice, for example, in connection with labour inspection visits. A recent cross-sectional study based on measured angular velocities and clinically diagnosed shoulder disorders pointed to 50°/s as a suitable exposure limit.3 In the present study, the mean intensity in the intermediate category, which yielded a significantly elevated ORadj, was approximately 40°/s for both men and women, which suggests that cumulative effects occur at even lower mean angular velocities across 10 years. Further studies are needed to evaluate risks associated with different patterns of acquiring a given cumulative exposure.
The shoulder load variable was constructed to capture exposure profiles that implied an increased risk of surgery for SIS.4 5 When we divided the highest exposure category into two, where the new upper category was defined by a combination of at least two high exposures, we found a higher risk associated with combined high exposures. We plan to further evaluate the effects of combinations of two or more occupational mechanical exposures on the risk of surgery for SIS in our nationwide cohort.
In principle, the relationships between occupational mechanical exposures and the risk of surgery for SIS could be due to an increased risk of SIS (ie, causation) or a higher probability of surgery given SIS (ie, aggravation). We have recently reported an increase in risk when expanding the time window from 2 to 10 years back in time,5 which indicates that the exposures cause SIS and not just aggravate the symptoms (if the exposures only aggravated symptoms, we would not expect to find an increased risk of surgery for SIS when expanding the time window back in time). For psychosocial factors, we found no statistically significant associations with surgery for SIS, which corroborates the results of our previous study5 and supports the viewpoint that occupational psychosocial factors are more closely related to shoulder symptoms than to pathological changes (cf. the introduction).
We did not identify leisure time shoulder intensive sports as a risk factor for surgery for SIS. Of note, this result only pertains to recreational sport since elite and professional sports were hardly represented in the present study.
In accordance with previous studies of surgery for SIS,11 12 our study showed a relationship with higher BMI. Our study did not account for the temporality of the observed relation, but BMI in 2010 was probably highly correlated with BMI in the years preceding surgery in 2007 or 2008. Self-reported BMI most often underestimates the true BMI, but cases and controls would probably be equally likely to underestimate their BMI. On the other hand, overestimation of BMI is rare so that persons in a high BMI category are most likely correctly classified. This means that the risk estimates for a high BMI are probably close to those that would have been obtained using measured height and weight.11 18 32 Since we have not identified sources of error that can explain away the positive associations in our study, it seems that there is still a case for including a high BMI as a potential risk factor in studies of SIS.
The above arguments regarding self-reported BMI probably also hold for smoking, meaning that risk estimates for high categories of self-reported pack-years of smoking are most likely close to estimates that would have been obtained using true smoking information. Previous studies have not identified smoking as a risk factor for SIS (apart from degenerative rotator cuff tears).19 21 This is the first study looking at pack-years of smoking, and the relationships, which we found, call for further attention to a potential relationship between smoking and SIS.
Little is known about mechanisms that link lifestyle factors and diabetes mellitus to SIS. A high BMI may contribute to peripheral vascular deficiencies through its associations with an increased production of adipokines; these molecules are able to induce inflammation, thrombosis, endothelial dysfunction and oxidative stress.12 Oxidative stress may lead to cell degeneration and apoptosis.12 Furthermore, obesity is associated with atherosclerosis, elevated cholesterol levels, diabetes mellitus and metabolic syndrome, which may induce peripheral hypovascularity.12 These changes may predispose to tendon degeneration and rupture. Nicotine is a vasoconstrictor and decreases oxygen delivery to the tissues.19 In addition, carbon monoxide decreases the cellular oxygen tension, which may also lead to tendon degeneration.19 The associations, which we found with diabetes mellitus and pack-years of smoking, lend support to the hypothesis that a microcirculatory harmful mechanism may play a role in the development of SIS.17 21 Studies focusing specifically on diabetes mellitus and risk of SIS are lacking.
In conclusion, our findings add to the evidence of an increased risk of surgery for SIS in relation to cumulative occupational mechanical exposures among men and women. For psychosocial factors no clear associations were found. Our findings also suggest an increased risk of surgery for SIS in relation to higher BMI, smoking and diabetes mellitus.
Acknowledgments
We would like to thank Ann Christie Poulsen for her coding of occupational titles and Jesper Medom Vestergaard for his help to manage occupational history dates. We also thank Gert-Åke Hansson for input on interpreting data. This study was supported by the Danish Working Environment Research Fund (grant no. 32-2009-03), the Danish Graduate School Network in Public Health Science (grant no. 07-07-2009) and The Danish Rheumatism Association (grant no. A1024).
References
Footnotes
Contributors Conceived and designed the study: PF and SWS. Developed the questionnaire: AD, PF and SWS. Analysed data: AD in close collaboration with PF and SWS. Interpreted data: AD, JHA, PF and SWS. Drafted the paper: AD in close collaboration with PF and SWS. All authors have reviewed the paper for important intellectual content, approved the final version of the manuscript and take responsibility for the integrity of the work as a whole.
Competing interests None declared.
Patient consent Our study is based on a questionnaire survey in which information on patient consent was described. Returning the questionnaire was considered an accept.
Ethics approval The Danish Data Protection Agency approved the study (j. no.: 2012-41-1187). In Denmark, register and questionnaire studies do not require approval by the Committee System on Biomedical Research Ethics (request no. 130/2009).
Provenance and peer review Not commissioned; externally peer reviewed.