Article Text

Abstract
Objective To evaluate the effectiveness of a self-management intervention (including an eHealth module), compared with usual care, in employees with chronic non-specific complaints of the arm, neck or shoulder (persisting >3 months).
Methods Participants were randomised into the self-management group (SG) or usual care group (UCG). The SG participated in 6 self-management sessions and could use an eHealth module; the UCG could use all available usual care. The primary outcome of the study was score on the Disabilities of the Arm, Shoulder and Hand questionnaire (DASH). Secondary outcomes included: absenteeism, pain in the previous week, quality of life, pain catastrophising, self-efficacy, work style, presenteeism, fatigue, and limitations experienced during work. Data were analysed using generalised estimating equations (GEE) linear regression and Mann-Whitney U tests, and were collected at baseline, 3-month, 6-month, and 12-month follow-up.
Results On the general module of the DASH, no significant difference between SG and the UCG was detected. On most of the other outcome measures, there were no significant between-group differences. In the DASH work module, the between-group effect was −3.82 (95% CI −7.46 to −0.19, p=0.04). For limitations experienced in job-related activities the between-group effect was −1.01 (95% CI −1.97 to −0.04, p=0.04). The mean hours of sport activities in the past 3 months, measured at 12 months, was 1.00 h (95% CI −1.90 to −0.12 h, p=0.03) less in the SG compared with the UCG.
Conclusions The self-management intervention improved the participants’ perceived disability during work. Since no significant between-group differences were found on most outcome measures, the results of this study should be interpreted with caution.
Trial registration number Dutch Trial Registration number NTR 3816.
Statistics from Altmetric.com
What this paper adds
Since there is no consistent evidence to demonstrate the effectiveness of interventions for work-related complaints of the arm, neck or shoulder (CANS), there seems to be a need for effective intervention programmes for employees with work-related CANS.
A self-management programme for this population was developed because self-management programmes addressing the multifactorial origin of CANS may be useful for employees with CANS.
In this randomised controlled trial, on most outcome measures no significant difference between the groups was found. The self-management group showed a significantly better improvement only on the work module of the Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) and on limitations experienced in job-related activities compared with the usual care group. The usual care group showed significantly higher mean hours of sport activities.
Background
Complaints of the arm, neck or shoulder (CANS) are common among employees. The reported point prevalence varies from 1.6% to 53%, and the 12-month prevalence varies from 2.3% to 41% depending on the setting, definition, and classification used.1–3 Nearly 19% of the patients report chronic complaints of which 58% report the use of healthcare such as the care given by the general practitioner, medical specialist and physical therapist.2–4
CANS include all complaints in the arm, neck or shoulder region not caused by a trauma or systemic disease.4 In CANS, a distinction can be made between specific CANS (23 specific diagnosable disorders) and non-specific CANS.5 Non-specific CANS can cause substantial loss of productivity at work.6 The most important factors associated with this loss of productivity are related to pain and its impact on work and sleep, as well as to the psychological aspects of pain and work.6 Thus, CANS may cause activity limitations and restrictions in work participation (presenteeism, absenteeism and job loss).6 7 In 2012, CANS were responsible for 11.2% of the total absenteeism in the Netherlands.8
Although the exact aetiology of non-specific CANS remains unknown, it is presumed to have a multifactorial origin.9–13 The factors related to CANS are generally divided into three main categories: (1) work-related physical factors, (2) work-related psychosocial factors and (3) personal factors. The importance of each factor and its individual contribution to the risk of provoking symptoms varies among individuals and work environments.14
There seems to be a need for effective intervention programmes for people suffering from CANS.15 16 A recent Cochrane review on conservative interventions for treating work-related CANS17 did found no consistent evidence for significant effects of exercises, ergonomic interventions, behavioural interventions, and some other interventions on pain, recovery, disability, or sick leave.17
Self-management is an approach increasingly used in chronic disease care to improve self-efficacy and wellness behaviours.18 Barlow et al19 defined self-management as ‘the ability to manage the symptoms, treatment, physical and psychosocial consequences, and lifestyle changes inherent in living with a chronic condition’. Given the multifactorial origin of CANS, self-management programmes addressing physical characteristics, psychosocial characteristics and personal factors of the individual worker, as well as characteristics of their work environment, may be useful for employees with CANS.20
Detaille and colleagues21–23 developed a generic self-management programme for employees in the Netherlands with a chronic somatic disease. Following the process of intervention mapping24 25 and based on a recent Dutch multidisciplinary guideline for non-specific CANS,26 and focus group interviews with employees27 and experts,28 we adapted the original programme to suit the needs of employees with CANS, and to alleviate the problems and needs of employees with CANS. The developed intervention included an eHealth module to provide the opportunity to participants to find additional resources which, together with the personal action plans made in the group sessions, would make it possible to tailor the programme to the needs of the individual participant. The overall goal of the intervention was defined as ‘self-management behaviour at work’ with the aim to alleviate the perceived disability of the participants;29 this was operationalised as: (1) to be able to cope with pain, fatigue, and work limitations, (2) to be aware of and adequately cope with stress factors at work and (3) to be able to communicate effectively about CANS with one's supervisor and colleagues.29
The aim of this study is to evaluate the effectiveness of the self-management intervention, compared with usual care, in employees with chronic non-specific CANS (persisting >3 months).
Methods
Study design and sample
The study was a randomised controlled trial (RCT) with a follow-up of 1 year comparing the self-management intervention to usual care. Data were collected at baseline, 3-month, 6-month and 12-month follow-up. The Medical Ethics Committee (METC) of the Radboud University Medical Centre (RUMC) in Nijmegen, The Netherlands, approved the study design, protocols and procedures (number 2012/319). The trial was registered in the Dutch Trial Register (NTR3816) (http://www.trialgregister.nl).
Participation was voluntary and participants could withdraw at any moment without any consequences. The methods used in this study were extensively described elsewhere.20
Participants were recruited from employees of the RUMC, the HAN University of Applied Sciences (HAN UAS), and Sanquin Blood Supply (SBS), all located in Nijmegen, the Netherlands, and from the general population (in the area of Nijmegen). Potential participants were recruited by newsletters and websites within the organisations and were informed about the project by company physicians, occupational health coordinators, and supervisors. Participants from the general population were recruited by calls in local newspapers and by contacting the Dutch patient organisation the ‘RSI vereniging’ (Patient Association for Repetitive Strain Injury).
Candidates willing to participate could contact the first author (NH) who arranged a consultation with a research physical therapist. If potential participants obviously did not meet the eligibility criteria, no consultation was arranged. Potential participants from outside the three participating organisations received a travel allowance of 0.19 eurocents/km for attending the appointment with the physical therapist. Eligible candidates received an information letter about the project at least 7 days before this consultation. The physical therapists (Frank Klomp and Steven van Moorsel) were experts in musculoskeletal disorders and provided additional information about the implications of participation. During the consultation, the physical therapist checked the eligibility of the employee based on the inclusion and exclusion criteria, which were based on a multidisciplinary guideline on non-specific CANS26 (see online supplementary appendix 1 for a shortened version; the extensive version is described elsewhere20), by history taking and screening of the employee (including filling out the Four-Dimensional Symptom Questionnaire (4DSQ)).30 If considered necessary, the physical therapist performed a brief physical examination to rule out any exclusion criterion, including a suspicion of specific CANS.26 During the consultation, each participant was asked to sign an informed consent.
Treatment allocation and procedures
Participants were assigned to either the self-management group (SG) or usual care group (UCG) by randomisation with prestratification for the three participating companies and for participants from the general population (4 groups). The allocation sequence was computer generated (http://www.randomization.com/) with a block size of four. A researcher not involved in assigning participants to their groups prepared concealed, consecutively numbered, sealed, opaque envelopes. Every envelope contained a paper indicating the treatment allocation. Participants received their randomisation envelope at the end of the consultation with the physical therapist, who was not aware of the randomisation sequence. Participants could open the envelope while they were with the physical therapist; subsequently, the physical therapist informed the first author (NH) about the treatment allocation. Participants allocated to the SG received information (from NH) about the next series of the self-management programme after randomisation. At the start of the programme, they also received the login code for the eHealth module. The UCG participants were informed that they were allowed to use all usual care available.
Blinding
Participants, trainers and researchers cannot be blinded for the allocated treatment after randomisation. However, all participants filled in the digital questionnaires at their home or at work, implying that the influence of researchers is ruled out. The data were collected by the developer of the digital questionnaire, who then provided the anonymous data to the researcher.
Interventions
Self-management group
The development of the self-management intervention has been described elsewhere.29 The intervention consisted of six weekly group sessions of 2.5 h each, with 4–12 participants per group. The group sessions were held in the daytime and in the evening. Employees from HAN UAS, RUMC and SBS were able to follow the sessions during working hours.
The meetings were moderated by a moderator (Anneke Nieuwland, Elvira Nouwens, Ingrid Broeders, Nanette Nab or Sarah Detaille). The first session started with an introduction to the programme and of the participants. Each subsequent session started with summary reflection on the action plans made in the previous session. After this, the relevant topics were discussed (see online supplementary appendix 2). At the end of each session, participants were asked to set targets (Specific, Measurable, Acceptable, Realistic, Time-bound (SMART) and formulated in terms of behaviour), and action plans were made.
The group sessions were complemented by an eHealth module. Participants were able to log in on a secured website on which the topics of the group training were discussed. Also, additional information was available on self-management and on specific topics of CANS (see online supplementary appendix 2). The eHealth was available for the SG up to 12 months after the start of the group sessions. Participants in the SG were allowed to attend all available additional treatments (co-interventions). Information on all co-interventions received by participants in the SG and the UCG were collected by questionnaires at 12 months.
Usual care group
The UCG could use all usual care and information available within the organisation of the participant. They were also allowed to use all care available outside the organisation.
Outcome measures and data collection
The SG and the UCG received the baseline questionnaire after randomisation in the week before the start of the self-management programme of the SG. The other questionnaires were provided at 3, 6 and 12 months after the baseline questionnaire. Given the length of the questionnaire, not all secondary outcome measures were measured at all follow-up moments (these questionnaires are marked with an asterisk (*)).
All questionnaires were provided digitally on a secured website. In case participants preferred a paper questionnaire, a paper version was provided.
Characteristics of the participants were collected at baseline together with the first questionnaire. The outcome measures, including clinometric characteristics of the measurement instruments used, were extensively discussed elsewhere.20 In short, the primary outcome measure was the self-reported disability (in the previous week) of the arm, shoulder and hand, measured with the Dutch version of the Disabilities of the Arm, Shoulder and Hand questionnaire (DASH).31 32 Secondary outcomes were absenteeism, presenteeism (Dutch version of the Stanford Presenteeism Scale (SPS-6)33 34 and the Work Limitations Questionnaire35), pain in the previous week (Numeric Pain Rating Scale (NPRS), 0–10), pain catastrophising (Pain Catastrophizing Scale (PCS), Dutch language version),36 self-efficacy (Dutch Adaptation of the General Self-Efficacy Scale),37 self-efficacy at work (self-efficacy at work scale),22 fatigue (Checklist Individual Strength),38 burnout (Utrecht Burnout Scale, UBOS),39 work style (Workstyle Short Form),40 pace and amount of work, relations with colleagues/supervisors, need for recovery, and participation and autonomy at work (questionnaire on experiencing and assessing stress at work (Dutch: VBBA),41 quality of life (SF-12v2),42 and self-reflection and insight (Self-Reflection and Insight Scale).43 Participants also had to respond to questionnaires developed by the authors about the use of healthcare interventions*, workplace adaptations*, conversations with colleagues* and supervisor*, participation in sport*, limitations experienced in work-related activities* (limitations experienced in the previous 2 weeks, Numeric Rating Scale (NRS), 0–10), work capacity* (NRS 0–10), and about attitude towards self-management*22 (7-point Likert scale).
Statistical analyses
Our initial sample size calculation was based on the primary outcome of this study, the DASH,31 and was presented in our study protocol.20 This sample size calculation was based on an independent sample Student t test and revealed a sample size of 71 participants in each group, assuming a drop-out rate of 20%, and assuming an effect of 10 points on the DASH over the entire follow-up period for it to be clinically important;44 we also used a SD of 16.65 that we had used in the previous sample size calculation based on an independent sample Student t test. However, most data were analysed using generalised estimating equations (GEE) with an exchangeable correlation structure. GEE is a longitudinal data analysis technique that is suitable to investigate the course over time of the outcome variable and to compare this overall effect between study arms.45 The earlier sample size calculation was not appropriate when using GEE. Therefore, using the same assumptions as used in the initial sample size calculation, we also calculated the necessary sample size for the GEE analysis assuming a within-subject correlation coefficient46 of 0.4. This renewed power analysis revealed a sample size of 42 participants in each group, which implied that a total of 84 participants were needed to detect a difference in score on the DASH with a power of 0.90 and an α of 0.05.
The SG and the UCG were checked for baseline differences demographic characteristics. All analyses were performed according to the intention-to-treat principle. Normality of the data was checked and verified by histograms, normal probability plots and Shapiro-Wilk tests.47 Since data on absenteeism were not normally distributed, Mann-Whitney U tests were performed on the cumulative means of all three follow-up measurements and no correction for baseline values was applied.
Between-group differences of all outcomes only measured at baseline and 12 months were analysed using linear regression. Between-group differences of all outcomes measured at baseline, 3, 6, and 12 months were analysed using GEE. Since GEE can adequately handle missing values (<20%), no imputation technique was needed.46
Each outcome variable was analysed as a dependent variable using the study group as an independent variable adjusted for the baseline measurement of each questionnaire. Correction for confounding was only applied if the regression coefficient of the intervention variable changed by more than 10% when the potential confounding variable was added to the model.46 Results were considered significant if p<0.05. Data on the use of usual care, workplace adaptations, and conversations about complaints with supervisor and colleagues were presented as descriptive data. Additional to the intention-to-treat analysis, a per-protocol analysis was performed with all participants of the SG who had participated in four or more self-management sessions so as to evaluate the effects of the intervention unaffected by protocol deviations or non-adherence.48 All analyses were performed with IBM SPSS Statistics V.20.
Results
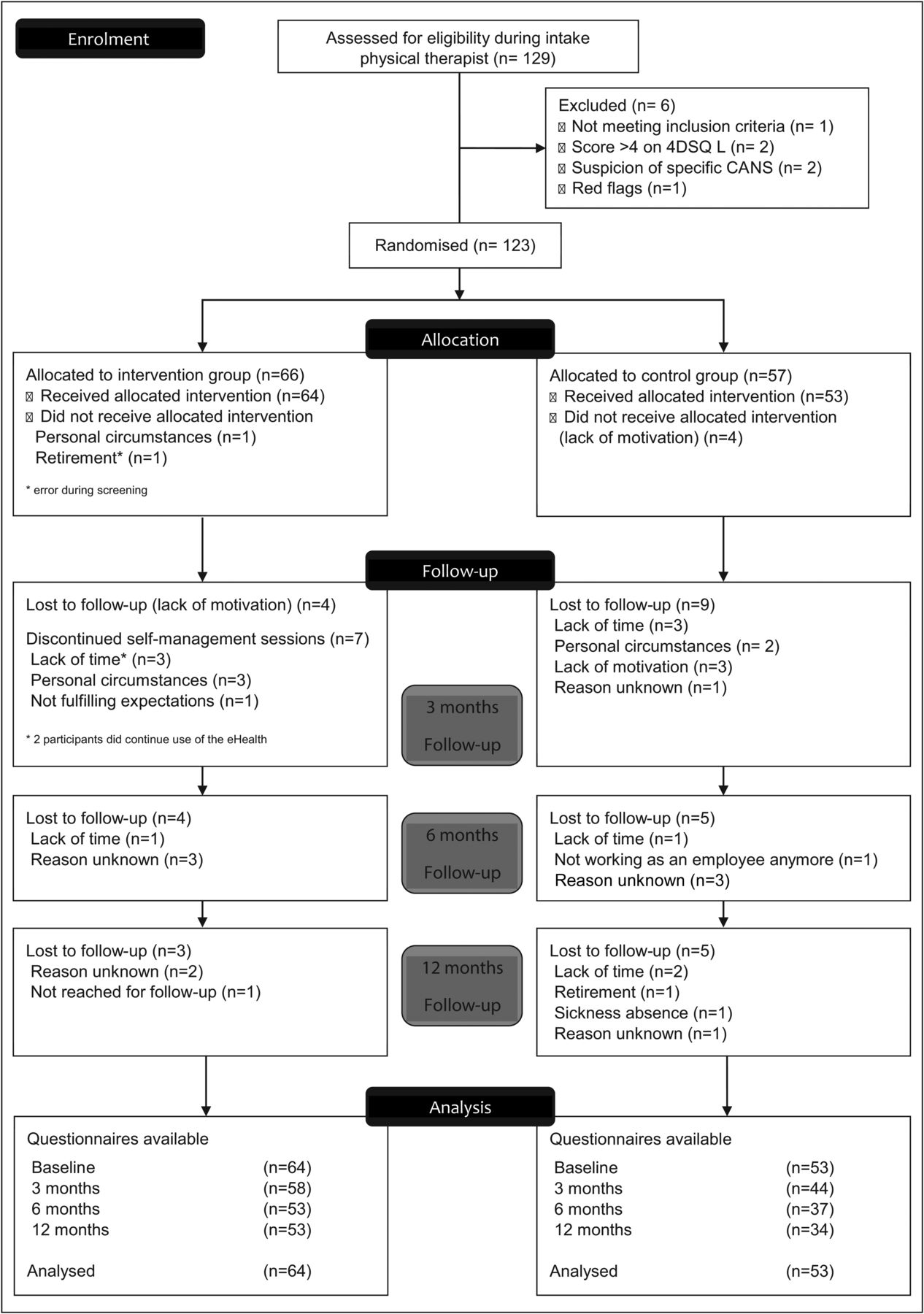
Participants for the intervention were recruited from September 2012 until January 2014, and the self-management sessions were held between October 2012 and March 2014. A total of 243 employees were interested in participating and received information about the trial. A total of 129 participants were assessed for eligibility during the intake, of which 123 were randomly allocated to either the SG (n=66) or UCG (n=57). Forty-four participants were employees from the RUMC, 12 participants were employees from HAN UAS, and 2 participants were employees from SBS; the remaining 65 participants were recruited from the general population. Figure 1 shows the participant flow through the phases of the trial. The baseline characteristics of the participants are presented in table 1. None of the characteristics at baseline differed significantly between SG and UCG.
Baseline characteristics of the study population

{kind=link}
Flow chart of participants through the trial (enrolment, allocation, follow-up and analysis) (CANS, complaints of the arm, neck or shoulder; 4DSQ, Four-Dimensional Symptom Questionnaire).
Figure 1 shows the drop-out of participants in both groups during the study and the questionnaires available for analysis on every follow-up time point. In total, 9 of the 66 participants allocated to the SG did not start or discontinued their attendance at the self-management sessions. Two of these participants did continue the use of the eHealth module. Of the 64 participants who started the self-management sessions, 59 persons (92.2%) participated in four or more of the sessions. They participated on average in 5.34 (SD 1.37) of the 6 self-management sessions. The use of the eHealth by the SG is presented in table 2.
Use of the eHealth module by the intervention group, measured at 12 months (n=53)
Effectiveness of the intervention programme
The results of the GEE analysis showed that on the general module of the DASH, no significant difference between SG and the UCG was detected. Most of the other outcome measures also showed no significant differences between the groups (see table 3). In the DASH work module, the between-group effect was −3.82 (95% CI −7.46 to −0.19, p=0.04), indicating that the SG had a 3.83 lower average score compared with the UCG. For the question about the limitations experienced in job-related activities, the between-group effect measured at 12 months was −1.01 (95% CI −1.97 to −0.04, p=0.04). The mean hours of sport activities in the past 3 months (measured at 12 months) was 1.00 h (95% CI −1.90 to −0.12 h, p=0.03) less in the SG compared with the UCG. Per-protocol analysis showed similar results compared with the intention-to-treat analysis for all outcome measures (data not shown).
Effects of the intervention on the outcome measures
Use of co-interventions, workplace adaptations and conversations about complaints
Data with regard to the use of co-interventions are presented in online supplementary appendix 3. Generally, co-interventions were used slightly more in the UCGs; however, the differences were generally small. It was only in the use of physical therapy that the overall mean use differed considerably (SG: 4.04 vs UCG: 8.77 sessions). The SG had a slightly higher frequency of consultations with the orthopaedic surgeon and psychologist compared with the UCG.
Data on the implementation of workplace adaptations and conversations about the complaints with supervisor and colleagues, including the frequency and the outcome of the conversations (see online supplementary appendix 3), show that these were generally used by the same percentage of participants in both groups. Only on self-adaptation of the workplace, SG showed a higher percentage of participants compared with the UCG (60.4% vs 32.8%). Moreover, the percentage of participants who communicated about their complaints with colleagues was higher in the SG compared with the UCG (25% vs 5.3%) and they also had a (mean) higher frequency of conversations (6.23 vs 1.50).
Discussion
Effectiveness of the intervention programme
This is the first study evaluating the effectiveness of a self-management programme (including an eHealth module) for employees with non-specific CANS. On most outcome measures no significant differences between the groups were found; therefore, the results of this study should be interpreted with caution. In the DASH work module, both groups showed clinically important improvements, with the SG showing significantly more improvement compared with the UCG (p=0.04). However, the difference between the SG and the UCG was not clinically important. The limitations experienced in work-related activities in the SG decreased significantly compared with the UCG at 12 months (p=0.04), which confirmed that the self-management programme improved the work-related capacity of participants in the SG. However, on the Work Limitations Questionnaire, as well as the SPS-6 (both also evaluating disability during work), no significant changes between groups were found. We think this is due to the fact that these two questionnaires consist of questions related to very specific activities (eg, In the past 2 weeks, how much of the time were you able to lift, carry, or move objects at work weighing more than 10 lbs, without difficulty caused by physical health or emotional problems?) which may not have been relevant for the individual employee with CANS in our population; however, the DASH work module and the question on the limitations experienced in work-related activities address more general work limitations (eg, doing your work as well as you would like), so probably the employee is better able to score on this questionnaire with their own specific limitations in mind.
Although no significant difference occurred in need for recovery, the mean values of the SG decreased, while the values of the UCG increased. The overall between-group effect was −4.95 (95% CI −10.62 to 0.71, p=0.09), which could indicate that the intervention had an effect on dealing and coping with the complaints. The descriptive data on the frequency of conversations with colleagues about their condition show that they were more frequently applied by participants in the SG compared with the UCG, while the data with regard to conversations with supervisors showed no major difference. The higher percentage of participants performing self-adaptation of their workplace in the SG, compared with the UCG, indicates that the SG was more actively involved in the adaptation of their workplace.
The UCG showed a significantly higher number of mean hours performing sport activities in the previous 3 months compared with the SG (measured at 3-month follow-up).
Comparison with other studies
Contrary to the study of Detaille et al,23 in investigating the effectiveness of a generic self-management programme in workers with a chronic somatic disease, we found no significant changes in the level of attitude towards self-management at work (enjoyment scale) and the physical health scale of the SF-12 between the groups, although the physical health of the intervention group (Physical Component Scale SF-12) improved more compared with the control group (p=0.09). In our study, the baseline values of the attitude towards self-management were already higher compared with the values of the study population of Detaille et al at baseline and at the follow-up time points, possibly indicating a ceiling effect.
Another intervention49 50 targeted on behavioural change with regard to physical activity and/or work style, in which computer users participated in six monthly group sessions at the work place and obtained tailored advice, was effective in improving recovery from neck/shoulder complaints and reducing pain (with regard to the previous 4 weeks) at 12 months compared with usual care.50 Since we found no significant change in the reported pain in the previous week, the differences in content and design of the two interventions, as well as the characteristics of the study population, might have played a role.
Strengths and limitations of the study
Strengths of the study include the RCT design and the use of prestratification with regard to the participating institutions and employees from the general population. Another strength is the follow-up period over 12 months. Participants were recruited from different organisations and from the general population. Moreover, participants had various jobs and duration of symptoms, which contribute to the generalisation of the results. The start time points of the different SGs were distributed over more than 1 year, thereby eliminating possible seasonal variance. Since the additional per-protocol analysis showed similar results compared with the intention-to-treat analysis, we can conclude that protocol deviations or non-adherence did not influence the results of the intention-to-treat analysis.48 Another strength of the study is the combination of a self-management programme and eHealth module, which could enhance the exposure to the intervention and enhance tailoring of the intervention. Therefore, the effects found in this study are the result of the combined interventions.
This study also has some limitations. The lack of use of the eHealth is a limitation of this study. It can be concluded that the eHealth was not a valuable addition for all participants and that individual preferences may have also played a role. Contrary to our expectations, it seems that the addition of an eHealth module to the self-management sessions did not result in more pronounced results, since the use of the eHealth module decreased between 3-month and 12-month follow-up.
This study also has other potential limitations. First, participants, moderators and researchers could not be blinded for the allocated treatment after randomisation. However, because all participants filled in the anonymous digital questionnaires at home or at their place of work, the influence of researchers is ruled out.20 Participants were generally highly educated and a majority were working in the healthcare setting, which could have influenced the results. In the study of Detaille et al,23 lower educated workers scored better on the Physical Component Scale of the SF-12 in the intervention group compared with the control group. In the present study, most data on the use of co-interventions, workplace adaptations, and conversations about complaints were based on small numbers of participants using co-interventions or workplace adaptations; therefore, no statistical analyses were performed.
Drop-out in both groups of our study differed directly after randomisation, that is, before the baseline measurement. Also, during the follow-up period, participants in both groups dropped-out (SG, n=11; UCG, n=19), which could have led to selection bias. The baseline values of the DASH of the participants in this study were generally low considering the range of the DASH (0–100), which is comparable with another study.51 Therefore, a floor effect could be present and a clinically important improvement of 10 points is less likely to be achievable. Also, a major section of the participants in our study had a longer duration of symptoms. Persons with symptoms with a longer duration often have a stable functional disability score, and are less likely to exhibit dramatic changes after treatment,52 which could also partly explain the small improvements on most outcome measures.
The natural course of complaints could have played a role in the improved outcomes measured in the SG and the UCG. Moreover, effects could be influenced by regressive fallacy, in which people with a chronic disease search for interventions when they are feeling at their worst.23 Another potential cause of bias is the Hawthorne effect,53 that is, the difference in the amount of attention participants receive, which could lead to an overestimation of the effect in the SG and to a lesser extent, in the UCG. Also, since the UCG was aware of the existence of a self-management programme and filled in the questionnaires, it is possible that the UCG became more conscious of the self-management behaviour, and they might have adopted such behaviour more often and in this case changed their behaviour with regard to sport activities. This may have led to improvements on some of the outcome measures.23
In this study, we had some difficulties in recruiting sufficient participants. This was partly due to the fact that participating in the intervention would cost time and not all supervisors of potential participants were willing to cooperate. A major cause of participants refusing to participate was the chance of being randomised to the UCG. During the study, we also had to deal with a high number of drop-outs, especially in the UCG (about 40% drop-out). People were not willing to take the time to fill in (all) the questionnaires, which could have led to selection bias.
We used a follow-up period of 12 months. One study investigating the effectiveness of a job maintenance training programme for employees with a chronic disease found only a significant improvement in self-efficacy after 24-month follow-up.54 Therefore, it is possible, that for some outcome measures a longer follow-up period might be needed.
A final limitation might be that all data were self-reported and there was a possibility of recall or information bias. However, as this study is designed as an RCT, we expect recall bias to occur to the same extent in both study groups,20 except for the questions with regard to the use of the eHealth, which were only collected in the SG.
Implications for practice and future research
In future interventions, it seems necessary to enhance the use of the eHealth module. The cost-effectiveness of the intervention could also be investigated. As mentioned before, Detaille et al23 found that lower educated workers scored better on the Physical Component Scale of the SF-12 in their intervention, and participants in our study were generally highly educated. Therefore, the effectiveness of the intervention in employees with a lower educational level should be further investigated. Moreover, parts of the intervention might also be effective in other disorders or can be used in usual care provided to employees with CANS. In future studies, researchers should try to prevent drop-out from the UCG and if possible, make use of more objective outcome measures, for example, for absenteeism, and for the use of the eHealth module. Also, a longer follow-up could be used to evaluate whether the results are more pronounced in the long run.
Conclusions
In this study, no significantly or clinically important differences between SG and UCG were present on most outcome measures. This should be kept in mind when interpreting the results of this study. However, this study indicated that participants in a self-management intervention, including group sessions and an eHealth module, showed clinically important improvements in the DASH work module, with the SG showing a significantly better (but not clinical important) improvement compared with the UCG. Moreover, the limitations experienced in work-related activities in the SG significantly improved compared with the UCG. It can be concluded that the self-management intervention improved the participants’ perceived disability during work and contributed to the improvement of self-management behaviour at work.
Acknowledgments
The authors thank all participants and organisations involved in this study. They thank Anneke Nieuwland, Elvira Nouwens, Ingrid Broeders, Nanette Nab and Sarah Detaille for moderating the sessions, and Vincent Bastiaans for his contribution to the sessions about sports/exercises. They also thank Frank Klomp and Steven van Moorsel, and the Department of Physical Therapy of the Radboud University Medical Centre in Nijmegen, The Netherlands, and the Department of Physical Therapy of the HAN University of Applied Sciences in Nijmegen, The Netherlands, for performing the eligibility screening of potential participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Funding This study was funded by ZonMw, the Netherlands Organization for Health Research and Development (208030004).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Medical Ethics Committee (METC) of the Radboud University Medical Centre (RUMC) in Nijmegen, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.