Article Text

Abstract
Systematically review observational studies concerning the question whether workers that perform pushing/pulling activities have an increased risk for upper extremity symptoms as compared to workers that perform no pushing/pulling activities. A search in MEDLINE via PubMed and EMBASE was performed with work-related search terms combined with push/pushing/pull/pulling. Studies had to examine exposure to pushing/pulling in relation to upper extremity symptoms. Two authors performed the literature selection and assessment of the risk of bias in the studies independently. A best evidence synthesis was used to draw conclusions in terms of strong, moderate or conflicting/insufficient evidence. The search resulted in 4764 studies. Seven studies were included, with three of them of low risk of bias, in total including 8279 participants. A positive significant relationship with upper extremity symptoms was observed in all four prospective cohort studies with effect sizes varying between 1.5 and 4.9. Two out of the three remaining studies also reported a positive association with upper extremity symptoms. In addition, significant positive associations with neck/shoulder symptoms were found in two prospective cohort studies with effect sizes of 1.5 and 1.6, and with shoulder symptoms in one of two cross-sectional studies with an effect size of 2.1. There is strong evidence that pushing/pulling is related to upper extremity symptoms, specifically for shoulder symptoms. There is insufficient or conflicting evidence that pushing/pulling is related to (combinations of) upper arm, elbow, forearm, wrist or hand symptoms.
Statistics from Altmetric.com
Introduction
Workers of various occupations often report upper extremity symptoms. General estimates indicate that 20–40% of all workers experience symptoms in the neck/shoulders or arms/wrists/hands in the previous 12 months1 ,2 and these symptoms are associated with considerable work-related financial and personal consequences.2 In the Netherlands, the number of notifications of occupational disease (OD) due to upper extremity disorders was 841 in 2012.3 The three sectors with the highest annual incidence (per 100 000 worker years, 95% CI) for these ODs are construction (228, 95% CI 167 to 289), transport and storage (172, 95% CI 167 to 289) and agriculture, forestry and fishing (125, 95% CI 167 to 289).4
Scientific evidence of risk factors for upper extremity symptoms is essential to develop valid methods for the assessment of the work-relatedness of these symptoms—that is, whether (a part of) the symptoms can be attributed to work activities—for ergonomic evaluation or effective interventions at work.5 In the scientific literature, neck, forearm and wrist/hand symptoms are typically studied in association with repetitive movements and awkward (neck/wrist/hand) postures, for instance in office workers.6 Shoulder or neck/shoulder symptoms on the other hand are more often investigated in association with heavy workload.1 ,7 For instance, in a recent systematic review, Mayer et al8 reported strong evidence for an association between shoulder symptoms and manual material handling (MMH), hand-arm vibration, trunk flexion or rotation and working with hands above shoulder level, with OR's ranging between 1.1 and 5.1.
Upper extremity symptoms should be considered also when evaluating manual handling at work.8–14 Assuming that work-related musculoskeletal symptoms are associated with ‘high’ musculoskeletal loading, it can be expected that activities with relatively high external forces at the hands, also in combination with unfavourable arm postures or movements, are potential risk activities. Consequently, for the relationship between MMH and upper extremity symptoms it would be sensible to focus on pushing or pulling rather than on lifting or carrying. In lifting loads from floor level, gravitational forces at the centre of mass of the arm and the hand reaction forces are mainly directed at the glenohumeral joint and thereby resulting in relatively low mechanical joint loading. However, during pushing and pulling this may not be the case, causing relatively large joint moments with often unfavourable arm postures, for instance when a worker pulls with one arm a cart that is located behind the worker while the worker is walking forward. In laboratory experiments it was shown that pushing and pulling are accompanied with relatively high levels of shoulder load and relatively low levels of low back loading.15–18
Pushing and pulling have been defined as the exertion of a (hand) force, of which the direction of the major component of the resultant force is horizontal, by someone on another object or person.19 In pushing the (hand) force is directed away from the body and in pulling the force is directed towards the body. In work, pushing and pulling are ergonomically evaluated using guidelines based on psychophysical criteria,20 of which the maximal acceptable hand forces also have been adjusted based on threshold limits for energetic workload and load at the low back.21 Based on a few studies22 ,23 we proposed to include also shoulder loading in the evaluation of pushing and pulling.24 However, as far as we know, the literature has not been systematically reviewed for evidence of a relationship between pushing and pulling and upper extremity symptoms, which justifies an evaluation of the association between work-related pushing and pulling and the presence of upper extremity symptoms. Therefore, the objective of the present study was to systematically review observational studies concerning the question whether workers that have to perform pushing and pulling activities at work have an increased risk for upper extremity symptoms as compared to workers that have to perform less or no pushing or pulling activities at work.
Methods
Search strategy
A manual and computerised literature search was performed using the databases of MEDLINE via PubMed and EMBASE on 28 January 2014. No publication date restrictions were imposed. The keywords used in the PubMed database were ‘push’ or ‘pull’ or ‘pushing’ or ‘pulling’, combined with the more sensitive search strategy for the study of putative occupational determinants of diseases as suggested by Mattioli et al.25:
(occupational diseases [MH] OR occupational exposure [MH] OR occupational exposure* [TW] OR ‘occupational health’ OR ‘occupational medicine’ OR work-related OR working environment [TW] OR at work [TW] OR work environment [TW] OR occupations [MH] OR work [MH] OR workplace* [TW] OR workload OR occupation* OR worke* OR work place* [TW] OR work site* [TW] OR job* [TW] OR occupational groups [MH] OR employment OR worksite* OR industry) AND (push OR pull OR pushing OR pulling).
This search strategy was adapted for EMBASE, but was performed without MEDLINE:
‘occupational diseases’/exp or ‘occupational exposure’/exp or ‘occupational health’/exp or ‘occupational medicine’/exp or ‘work-related’ or ‘working environment’/exp or ‘at work’ or ‘work environment’/exp or ‘occupations’/exp or ‘work’/exp or workplace* or ‘workload’/exp or occupation* or worke* or ‘work place’ or ‘work site’ or job* or ‘occupational groups’/exp or ‘employment’/exp or worksite* or ‘industry’/exp and (‘push’ or ‘pull’ or ‘pushing’ or ‘pulling’) and [embase]/lim
References of key publications and included studies were checked for other relevant studies or reviews and personal databases of the authors were consulted.
Inclusion criteria
The papers identified using the search strategies in PubMed and EMBASE were screened by two authors (MH and PK) using the following inclusion criteria: (1) the study examined exposure to pushing and/or pulling in relation to upper extremity symptoms at the neck, shoulder, arm, wrist and/or hand, (2) the study design was cross-sectional, case–control or prospective cohort, (3) the study was published in English, German or Dutch. If the title and abstract did not provide enough information to decide whether the inclusion criteria were met, the full paper was checked. Next, the inclusion criteria were applied to the full paper. When doubts existed about whether a paper fulfilled the inclusion criteria, a decision was made based on consensus between both authors.
Assessment of risk of bias
After study selection and inclusion, the same two authors (MH and PK) independently assessed the risk of bias in each of the studies using a standardised set of 10 predefined criteria (table 1) according to the method presented by Ijaz et al.26 Each item had to be rated as a low (LR), a high (HR) or an unclear (UR) risk of bias. In accordance with Ijaz et al,26 the 10 items were divided into two hierarchical groups. The group with the major five domains of bias included exposure definition, exposure assessment, reliability of exposure assessment, analysis/research specific bias and confounding. The remaining five domains of bias were considered as the group with the minor five domains: attrition, blinding of assessors, selective reporting, funding and conflict of interest. Thereafter, each study was rated as a low risk or high risk of bias study. Studies were considered as low risk of bias if the study showed LR in four or five of the major domains of bias and in two or more of the minor domains of bias. The results of the assessments of risk of bias of the two authors were compared and differences were discussed during a consensus meeting.
List of criteria used to assess the risk of bias in and across the included studies26
Data extraction
The following information was extracted from the included articles: primary author (including country), year of publication, study design (prospective cohort, case–control or cross-sectional), characteristics of the study population (numbers of participants and respondents, age, sex and occupation), duration of follow-up, instruments used for exposure assessment and exposure definition, instruments used for outcome assessment and outcome definition, the main results of the study concerning the association between pushing or pulling and upper extremity symptoms, potential confounders assessed in the study and confounders included in the analyses (see online supplementary table S2). The data were extracted by one of the review authors (MH) and another review author (PK) checked the extraction.
Levels of evidence
A forest plot was made of the effect sizes found in the observational studies without a summary estimate, due to the heterogeneity in exposure and outcomes in the observational studies. To determine whether pushing or pulling at work is related to upper extremity symptoms a best evidence synthesis, presented by Kuijer et al27 and adapted from Van Tulder et al28 and De Croon et al,29 was applied consisting of three levels of evidence, taking into account the risk of bias, the design of the study (prospective cohort, case–control or cross-sectional) and the outcomes of the included studies. (1) Strong evidence was defined as consistent findings in at least two prospective cohort studies with low risk of bias and effect sizes in the same direction. (2) Moderate evidence was defined as consistent findings in at least one prospective cohort study with low risk of bias and one cross-sectional/case–control study with low risk of bias or one prospective cohort study with high risk of bias. In all other cases the evidence was defined as (3) Insufficient or conflicting evidence. We used the following rules for consistent findings27–29: (1) if there are four or more studies, the statistically significant findings of 75% or more of the studies have to be in the same direction; (2) if there are three studies, the statistically significant findings of at least two studies have to be in the same direction; (3) if there are two studies, the statistically significant findings of both studies have to be in the same direction.
Results
Search and selection
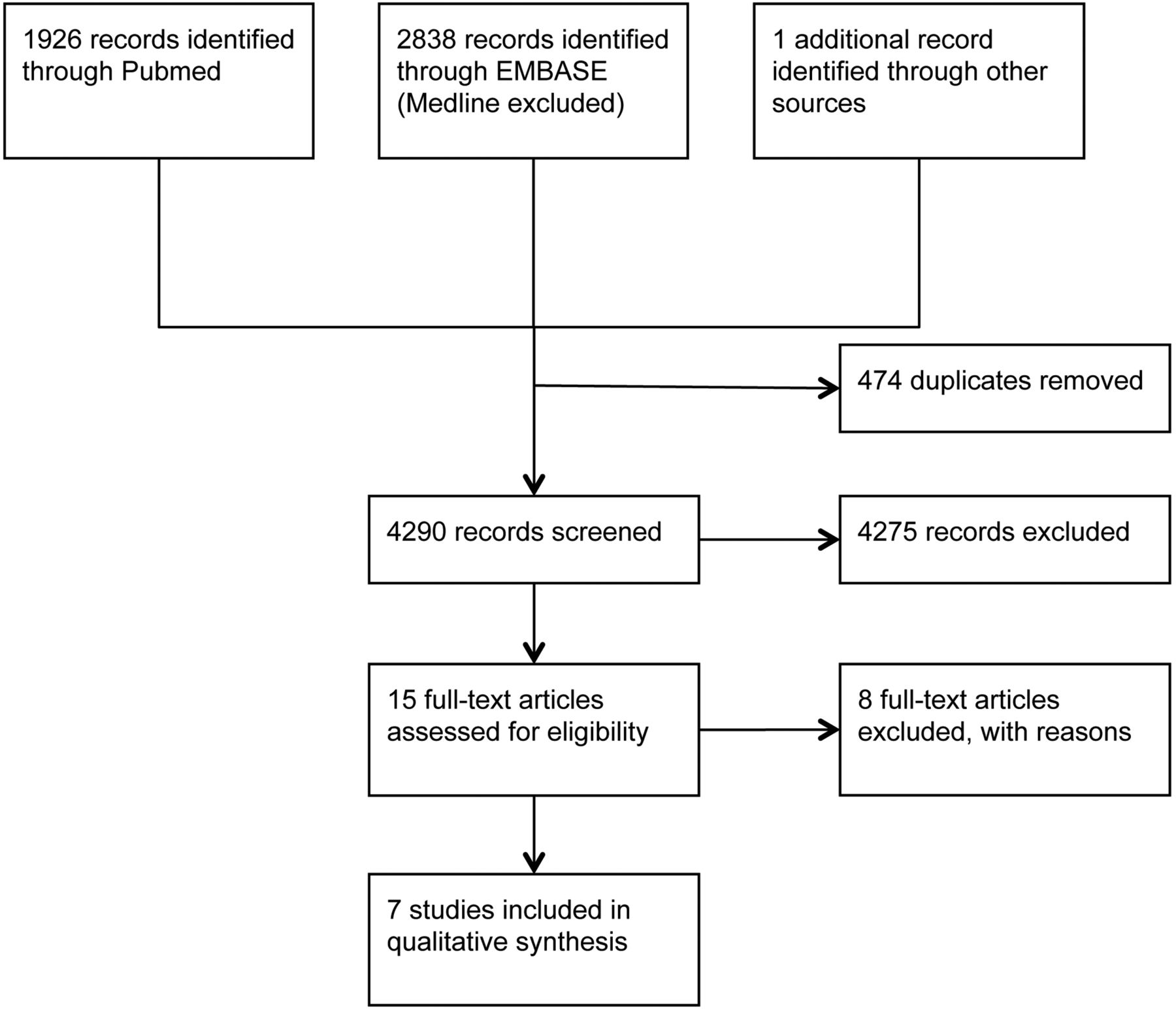
The search strategy resulted in 1926 hits in PubMed and 2838 hits in EMBASE (figure 1). A total of eight studies met the inclusion criteria, including three cross-sectional studies, one case–control study and four prospective cohort studies. Seven studies were performed in Europe and one in the USA. One cross-sectional study30 and one prospective cohort study23 were from the same study population. We decided to exclude the cross-sectional study30 from the evidence syntheses. The most important reason for excluding seemingly relevant studies was that pushing or pulling was not included in the analyses as a separate exposure, but as part of an exposure measure that included MMH in general, including lifting, carrying, pushing and pulling. The characteristics and results of the seven included studies are presented in online supplementary table S2.

Study flow diagram.
Study characteristics
In the seven studies a total of 8279 participants were observed (Median=683, IQR=705). Four studies1 ,9 ,22 ,23 had a prospective cohort design with a follow-up period ranging from 1223 to 24 1 ,9 ,22 months. Response rate ranged from 32%9 to 91%.22 Shoulder symptoms were specifically explored in five papers22 ,23 ,30–32 and neck/shoulder symptoms in two papers.1 ,9 Other upper extremity regions and combinations of regions were each studied in only one of the papers. Upper extremity symptoms were generally assessed using self-administered questionnaires and in one study31 by physical examination and in one other study11 using MRI. Also pushing and/or pulling were mainly assessed by self-administered questionnaires. Other methodologies used were systematic observation,23 job-surveillance checklist,31 interview11 and job description.32 Exposure to pushing and/or pulling was often defined in terms of frequency, sometimes in combination with load mass or duration. Only one study31 did not report an effect size in terms of OR or HR.
Assessment of risk of bias
Of the total of 70 items for the seven studies, the two raters agreed on 48 items (69%, table 2). After reaching consensus, and following the method presented by Ijaz et al,26 three prospective cohort studies were determined to be of low risk of bias and the other (four) studies of high risk of bias. Of the major domain of bias, reliability of exposure assessment was the item that was scored negative (HR or UR) most often (six out of seven studies).
Pushing and pulling in relation to upper extremity symptoms
For upper extremity symptoms in general (thus discarding body region), a positive significant association with pushing and/or pulling was observed in all four prospective cohort studies,1 ,9 ,22 ,23 of which three were scored as low risk of bias. For the high exposed categories the significant and adjusted effect sizes ranged from 1.5 (n=1513)1 to 4.86 (n=459).23 In three of four studies, only the high exposure category showed a significant association. Only the study of Hoozemans et al23 showed a stronger association for the medium exposed group compared to the high exposed group. Of the other three studies, two cross-sectional and one case–control study, one showed no association between pushing and/or pulling (effect size 0.9, 95% CI 0.5 to 1.8),11 ,33 ,34 and the other two showed significant associations (effect sizes between 2.0 and 5.0)31 ,32 of which one study31 mentioned that pushing and pulling were not in the final stepwise logistic regression model (variables stayed in the model at p values of <0.20). Considering these results there is strong evidence for pushing and/or pulling being significantly related to upper extremity symptoms.
Shoulder symptoms specifically were studied by two prospective cohort studies with low risk of bias22 ,23 and two cross-sectional studies with high risk of bias.31 ,32 As prospective cohort studies and one of the cross-sectional studies found significant adjusted effect sizes it is concluded that there is strong evidence that pushing and/or pulling are related to shoulder symptoms.
Neck/shoulder symptoms were examined in two prospective cohort studies.1 ,9 Both studies, of which one was scored as low risk of bias and the other as high risk of bias, reported significant effect sizes for the high-exposure groups of 1.51 and 1.6.9 According to the definitions of the presented levels of evidence, there is moderate evidence that pushing and/or pulling is related to neck/shoulder symptoms.
With respect to upper arm, elbow, forearm, wrist and hand symptoms, each of these outcome measures was included in only one of the studies. Andersen et al1 found pushing and pulling to be significantly associated (effect size 1.8, 95% CI 1.1 to 3.1) with elbow/forearm/hand pain. Hughes et al31 reported significant univariate associations for the combinations elbow/forearm and hand/wrist, however, pushing and pulling were not in the final multiple logistic regression model. Seidler et al11 ,33 ,34 found no significant association between pushing and pulling and the presence of supraspinatus tendons tears and Van der Beek et al32 reported significant adjusted ORs of 4.1 and 5.0 for upper arm and forearm symptoms, respectively, in lorry drivers who handled wheeled cages in comparison with lorry driver who only had a driving task. Therefore, there is insufficient or conflicting evidence that pushing and pulling are related to (combinations of) upper arm, elbow, forearm, wrist or hand symptoms.
Discussion
This systematic review is the first to reveal that there is strong evidence for pushing and/or pulling at work being significantly related to upper extremity symptoms with effect sizes in terms of risk ratios ranging between 1.3 and 5.0. More specifically, the evidence synthesis of this literature review shows that there is strong evidence that pushing and/or pulling at work are related to shoulder symptoms, moderate evidence that pushing and/or pulling at work are related to neck/shoulder symptoms and that there is insufficient or conflicting evidence that pushing and/or pulling at work are related to (combinations of) upper arm, elbow, forearm, wrist or hand symptoms.
The literature search resulted in only seven eligible studies, of which four were prospective cohort studies with a follow-up period of maximally 2 years. This means that, although the levels of evidence were strictly defined, the conclusions are based on a relatively low number of studies. Two of the seven studies had a cross-sectional design. This design is not suitable to detect whether pushing or pulling cause upper extremity symptoms. If workers with upper extremity symptoms changed to jobs that require pushing or pulling activities, this could result in the observed positive association between pushing or pulling and upper extremity symptoms in the two cross-sectional studies. However, this explanation seems not likely. In addition, the episodic nature of upper extremity symptoms hampers establishing a cause–effect relationship altogether and we, therefore, decided to include also cross-sectional studies. Moreover, in the best evidence syntheses, cross-sectional studies only minimally affect the levels of evidence, that is, when only cross-sectional studies are available the evidence is ‘conflicting or insufficient’ at best. For the prospective cohort studies, populations were free from symptoms at baseline and the incidences of symptoms in the follow-up period point to a potential causal relationship with pushing or pulling. However, the methodology of the assessment of exposure and outcome used, generally self-administered questionnaires and the episodic characteristic of upper extremity symptoms increase the risk of biased relationships. If exposure misclassifications are independent of the presence of symptoms, or precursors of symptoms, the reported effect sizes may even be underestimated.35 It is, however, difficult to rule out differential misclassification. The presence of minor symptoms at baseline, which is sometimes defined as pain free,1 ,9 may result in the self-report of relatively high exposure, which undermines the causal relationship. However, in one of our own studies,23 systematic observation was used to assess exposure to work-related activities and this more reliable classification appeared to be significantly associated with shoulder symptoms. Furthermore, ignoring significance, three of the four prospective cohort studies found dose–response relationships when looking at the effect sizes. Thus, it can be considered likely that work-related pushing and/or pulling can actually cause (self-reported) upper extremity symptoms.
Effect sizes (see figure 2 and online supplementary table S2) are difficult to compare because of differences in confounding variables that have been taken into account. We therefore assessed ‘potential confounders assessed’ and ‘confounders adjusted for’ during data extraction (see online supplementary table S2). In addition, we have considered ‘working/lifting above shoulder height’ to be an important potential confounder in the assessment of risk of bias (see table 1 and online supplementary table S2). As such, ‘working/lifting above shoulder height’ should have been assessed and its confounding effect should have been explored in the individual studies, for instance using multiple regression analysis. However, this does not mean that working or lifting above shoulder height has to be taken into account in the final regression model. It depends on the presence of this potential confounder in the work of the study population and on the distribution over exposure categories whether it biases the effect size, that is, the regression coefficients of pushing and pulling, in that particular study. If the effect sizes are not largely affected by including the potential confounders they should not appear in the final model. Also, it is often not clear whether studies had taken multicollinearity of potential confounding factors into account. Multicollinearity was only specifically reported in the studies of Andersen et al,1 Harkness et al22 and Hoozemans et al.23 Although Anderson et al1 reported no additional information and stated that ‘the one with the highest point estimate in the partially adjusted model was used’, Harkness et al22 mentioned that ‘Lifting weights at or above shoulder level’ was strongly correlated with ‘working with hands above shoulder level’ and with ‘lifting weights with one or two hands’ and only used the last one in the final analyses. Hoozemans et al23 indicated that ‘working behind a video display’ and ‘driving vehicles’ were highly correlated with pushing and pulling and, therefore, were not included in the analyses.

{kind=link}
{kind=link}
Forest plot—with the axis presented in logarithmic scale—of studies included. P&P, pushing and pulling, ns/na, effect size is not significant and not available.
A general limitation of this review is the limited number of studies, the relatively large differences in workload, and the diverse methodologies used for the assessment of exposure and outcome. This also refrained us from performing a meta-analysis and calculating a summary estimate for the forest plot (figure 2). Generally, exposure should be defined in terms of duration, frequency and intensity.36 However, in the included studies, the definition of exposure to pushing and pulling varied considerably using for instance job title, number of workdays and weights pushed or pulled besides duration and frequency. Significant risk ratios were observed for pushing or pulling >355 kg/h,1 >32 kg,22 >300 working days,33 >5 times/shift,9 88–234 times/day23 and >783 s/day.23 Unfortunately, this variation in exposure definition also makes it hard to establish threshold limits or cut-off points in exposure to prevent upper extremity symptoms.
Determining threshold limits for the assessment of work relatedness of upper extremity symptoms and/or ergonomic evaluation is also hampered by the variation in definition of upper extremity symptoms. Upper extremity symptoms were assessed mainly using questionnaires and in two studies using physical examination or MRI. As self-report using questionnaires and physical examination are associated with reliability and validity issues,37 the use of MRI may be the most reliable and valid method. However, MRI is a very expensive diagnostic method and its validity for the assessment of upper extremity symptoms can be questioned. Using MRI and ultrasonographic examination, rotator cuff tears have been found in people without shoulder symptoms, with prevalences varying between 8 and 34%.38–40 Therefore, the assessment of upper extremity symptoms using MRI should be applied with caution.
It is not clear yet which structures of the upper extremities should be examined in relation to the mechanical load associated with pushing and pulling. For instance, during pushing a cart with two hands at shoulder height it is expected that glenohumeral joint stability is essential. This means that during pushing the humeral head has to be kept inside the glenoid cavity for which rotator cuff activity is important. Another frequently observed activity is walking forward while pulling a cart behind the body with one hand. In this situation it is expected that passive structures, such as capsules and ligaments and muscles (considering their passive characteristics) be at high-strain levels.
Clearly, epidemiological data do indicate that pushing and pulling are related to upper extremity symptoms but do not suggest what exposure level is harmful and which specific upper extremity disorders are to be expected. To arrive at evidence-based guidelines for the prevention of work-related upper extremity symptoms due to pushing or pulling, or forceful exertions using the upper extremity in general, we recommend performing prospective cohort studies with appropriate assessments of exposure and outcome. However, in practice these studies are time-consuming and labour intensive. Another approach would be to specifically focus on the biomechanics of the upper extremity. We have recommended24 applying the shoulder-moment strength mean prediction equations for exertions in the sagittal plane published in the book of Chaffin et al41 for the evaluation of shoulder load. This is, however, a limited data set and based on the rationale that workload should be (somewhere) below the maximal forces or moments that a certain population can generate. Future studies should be aimed at mapping out the mechanical load on the upper extremities during forceful exertions in different postures, for instance using mechanical models.42–44 Net shoulder moments or glenohumeral joint compression forces are outcome parameters of these models that can be used to reflect overall shoulder loading.16 ,45 Efforts should be undertaken to determine the actual structures at risk, such as the rotator cuff or passive structures. However, mechanical models are not yet capable of assessing the load on passive structures. Moreover, this should be accompanied by studies aimed at determining the capacity of those structures in mainly submaximal situations to account for the frequency and duration effects of exposure, for instance using in vitro experiments or energy models.46 ,47
In the present systematic review only studies aimed at pushing and/or pulling and upper extremity symptoms were included. Pushing and pulling have been the subject of other epidemiological studies in which the upper extremity was indirectly included, for instance in terms of musculoskeletal injuries48 or widespread body pain.49 ,50 Most studies on pushing and pulling, however, have focused on the low back. Although older cross-sectional studies found significant associations between pushing and/or pulling and low back symptoms,19 more recent studies indicated that this relationship is at least questionable24 ,51 and biomechanical studies showed that low back loading during pushing or pulling is not as high as for instance in lifting loads.15–18 Still, the low back may be at risk because it is relatively unstable during pushing and/or pulling and therefore vulnerable to unexpected perturbations.52–55 Altogether, considering that pushing and pulling are associated with musculoskeletal symptoms, as well as sickness absence56 and unemployment,57 work-related pushing and pulling should be the subject of future epidemiological and biomechanical investigations to develop evidence-based ergonomic guidelines and preventive measures.
In conclusion, this systematic literature review provides strong evidence that work-related pushing and/or pulling is related to upper extremity symptoms and more specifically shoulder symptoms. However, only a few studies have been published to date, and further prospective cohort studies are recommended, including valid and reliable assessment of exposure and outcome. Only in this way can valid and reliable threshold limits be established for the assessment of the work-relatedness of upper extremity symptoms due to pushing and pulling.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors MJMH, EBK, PPFMK were involved in conception, design, analysis and interpretation. MHWF-D, HEJV were involved in revising the paper critically for important intellectual content and final approval of the version to be published.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.