Article Text

Abstract
Objectives To provide an overview of the epidemiology of work-related traumatic brain injury (wrTBI) in the state of Victoria, Australia. Specifically, we investigated sex differences in incidence, demographics, injury characteristics, in addition to outcomes associated with wrTBI.
Methods This study involved secondary analysis of administrative workers’ compensation claims data obtained from the Victorian WorkCover Authority for the period 2004–2011. Sex-specific and industry-specific rates of wrTBI were calculated using denominators derived from the Australian Bureau of Statistics. A descriptive analysis of all variables was conducted for the total wrTBI population and stratified by sex.
Results Among 4186 wrTBI cases identified, 36.4% were females. The annual incidence of wrTBI was estimated at 19.8/100 000 workers. The rate for males was 1.43 (95% CI 1.35 to 1.53) times that for females, but the gap between the two sexes appeared to have narrowed over time. Compared to males, females were older at time of injury and had lower preinjury income. Males had higher rates than females across most industry sectors, with the exception of education/training (RR 0.77, 95% CI 0.64 to 0.93) and professional/scientific/technical services (RR 0.64, 95% CI 0.44 to 0.93). For both sexes, the most common injury mechanism was struck by/against, followed by falls. WrTBI among males was associated with longer duration of work disability and higher claim costs compared to females.
Conclusions This study found significant sex differences in various risk factors and outcomes of wrTBI. Sex/gender should be taken into consideration in future research and prevention strategies.
- Occupational Injury
- Traumatic Brain Injury
- Gender
Statistics from Altmetric.com
What this paper adds
-
Work-related traumatic brain injury (wrTBI) is among the most serious occupational injuries and is associated with significant work disability and economic burdens.
-
Knowledge on sex/gender differences in risk factors and impacts of wrTBI is limited, as females have been largely under-represented in most previous studies.
-
Using a large database of worker’ compensation claims, this study provides the first epidemiologic profile of wrTBI in the Australian context, with a focus on sex/gender differences.
-
The incorporation of sex-based analysis revealed significant differences between male and female workers in terms of incidence, trends, demographics, occupational and injury characteristics, as well as outcomes of wrTBI.
-
This study contributes new knowledge on wrTBI through a gender perspective and highlights the need to take sex differences into consideration in future research and prevention strategies.
Introduction
Traumatic brain injury (TBI) is a critical public health issue and a major cause of death and disability worldwide.1 In Australia, the rate of hospitalisation due to TBI was estimated at 107/100 000 population during the fiscal period 2004–2005.2 Although work-related TBI (wrTBI) accounts for less than 10% of all reported TBIs,2–5 it is considered among the most serious occupational injuries. For instance, TBI contributed to nearly half of all worked-related deaths in the Canadian province of Ontario6 and was involved in more than 20% of severe/fatal occupational injuries reported to the Washington State Trauma Registry in the USA.7 Those sustaining TBI at work often face long-term physical, cognitive, psychosocial and emotional consequences that pose significant challenges in daily activities and return to work.8 In addition to work disability, wrTBI is associated with substantial economic burdens in terms of healthcare costs and lost wages.9–12
Given its impacts on workers and society, wrTBI has received little attention in the peer-reviewed literature until recent years, with several studies describing its epidemiology in the USA5 ,11–14 and Canada.4 ,6 ,9 ,10 ,15 However, to our knowledge, no study has specifically examined the epidemiology of wrTBI in the Australian context. According to a recently published report by Safe Work Australia,16 while the frequency of work-related injuries has decreased overall, particularly among males, the number of compensated claims for wrTBI increased by 28% between 2000–2001 and 2010–2011. Furthermore, TBI accounted for a greater proportion of work-related hospitalisations in females (3.5%) compared to males (2.2%).17
Sex disparities in occupational injuries have been previously described.18–21 For example, in the US state of West Virginia, male workers had significantly higher rates of work-related injuries/illnesses compared to females across most industry sectors.18 It has been suggested that differential job tasks and employment characteristics may have contributed to these differences.18–20 However, little is known about sex differences in wrTBI, as females tend to be largely under-represented in previous wrTBI studies focusing on hospitalised and/or fatal injuries.4–6 12–14 Workers’ compensation claims data have been increasingly used to examine the incidence and impact of work-related injuries across a wide range of severity levels.9–11 ,15 ,18 ,19 ,22 Specifically, Colantonio et al9 showed that over 40% of claims for wrTBI in Ontario involved females, with notable sex differences by industry and injury mechanism. These findings warrant further investigation in a larger wrTBI population that allows for detailed stratification by gender. Furthermore, with increasing participation of females in the Australian labour force and in industries typically dominated by males,23 the exploration of sex differences in risk factors and outcomes of wrTBI may have important implications in prevention strategies and rehabilitation efforts.
The purpose of this study was to provide an overview of the epidemiology of wrTBI in the state of Victoria, Australia, with a focus on sex/gender differences. Specifically, using a large administrative database of workers’ compensation claims, this study aimed to (1) describe sex-specific burden and trends of wrTBI over an 8-year period; (2) compare demographic, occupational and injury characteristics of wrTBI by sex; and (3) estimate work disability and compensation costs associated with wrTBI by sex.
Methods
Data source
This cross-sectional study involved secondary analysis of the Compensation Research Database (CRD), which contains data derived from administrative records of the Victorian WorkCover Authority (VWA). The VWA is a state government agency responsible for regulating the workers’ compensation system. Approximately 85–90% of workers in Victoria have their workers’ compensation insurance provided by the VWA, with the exception of federal government employees, sole traders and employees of some large self-insured employers.22 Following a work-related injury or illness, a claim may be lodged if the worker is able to demonstrate a causal link between the injury/illness and their work. Employers are responsible for income replacement for the first 10 days lost from work, beyond which the VWA provides compensation benefits to the worker. Medical expenses exceeding a certain threshold amount (eg, $A 592 in year 2010/2011) are also provided by the VWA. Details of the CRD and the Victorian workers’ compensation system have been described elsewhere.24 ,25 For this study, de-identified workers’ compensation claims data were obtained from the VWA for the 8-year period 2004–2011.
Study population
The study population consisted of Victorian workers aged 15 years or older who lodged a claim for TBI occurring between 1 January 2004 and 31 December 2011. For the purposes of this study, TBI was defined using a combination of ‘nature of injury’ and ‘bodily location of injury’ codes derived from the Australian Standard Type of Occurrence Classification System (TOOCS).26 The following criteria were used to identify wrTBI cases: (1) nature of injury coded as ‘intracranial injuries’ and bodily location as ‘cranium’ or ‘brain’; or (2) nature of injury coded as ‘fractures’ and bodily location as ‘head’ (excluding tooth/teeth), ‘head and neck’, or ‘head and other’. According to the TOOCS,26 ‘intracranial injuries’ include cerebral contusion/laceration, traumatic extradural/subdural haemorrhage/haematoma, traumatic subarachnoid haemorrhage, concussion, headache from blow to the head, and other unspecified head injuries, while fractured skull/facial bones without brain damage are coded to ‘fractures’. When multiple injuries are present, the most serious injury is identified, and where in doubt, brain injuries and fractured skulls receive priority over other types of injury.26
Although multiple claims per claimant represented a small proportion in this population (1.2%), previous studies have shown that they are not independent events.22 ,24 It was also difficult to determine from the data whether repeat claims involved new incidents or recurrences of a previous injury. Therefore, analyses in this study were restricted to the first TBI claim lodged by each claimant during the study period.
Measures
Based on previous wrTBI studies,4 ,6 ,9 we grouped the variables into three main categories: preinjury demographic characteristics, injury characteristics and outcomes.
Preinjury demographic characteristics included sex, age, income, occupation, industry sector, employment type and employer size. Income was defined as the total weekly earnings of the claimant prior to injury and was adjusted for inflation by converting into 2012 Australian dollar equivalent values based on the annual consumer price index (CPI). Occupations and industry sectors were defined using the Australian and New Zealand Standard Classification of Occupations27 and the Australian and New Zealand Standard Industrial Classification,28 respectively. Employment type was classified as full-time, part-time or other. Employer size was determined based on the employer's remuneration in 2010/2011 deflated to 2005/2006 dollars and was classified as small (<$1 million), medium ($1–20 million), large (>$20 million) or government.25
Injury characteristics included mechanism of injury, agency of injury and temporal factors. Mechanism of injury refers to the ‘action, exposure or event that best describes the circumstances that resulted in the most serious injury’, while agency of injury identifies ‘the object, substance, or circumstance that was the direct cause of the most serious injury’.26 Temporal factors examined included year, season, month and day of the week, which were derived from the injury date variable.
Outcome variables included duration of work disability, claim costs paid (total cost per claim, cost of medical and like services, cost of income replacement) and inpatient hospital stay. Duration of work disability was defined as the number of days lost from work and was calculated by adding the first 10 days paid by the employer and the number of days compensated by the VWA. However, for claimants with ≤10 days off work, the actual number of days lost from work could not be determined accurately as the VWA does not keep track of employer payments.25 Therefore, calculations of the number of days of work disability were restricted to those with >10 days off work. Total cost per claim refers to the total amount of payments associated with each claim, including payments for medical and like services (eg, rescue, treatment, rehabilitation), income replacement, superannuation entitlement, as well as payments for a work-related death.24 All costs were converted into 2012 Australian dollar equivalent values based on the CPI and were estimated as an average for all claims (ie, zero costs were included) as well as separately for time-loss claims with >10 days off work and medical-only claims with medical expenses exceeding the threshold amount. Additionally, the proportion of claimants with at least 1 inpatient hospital stay was determined based on hospital admissions’ data collected by the VWA.
Statistical analysis
Descriptive statistics were computed for the total wrTBI population and separately for males and females by generating frequency distributions for categorical variables and calculating means, SD, medians and IQR for continuous variables. To make comparisons by sex, χ2 tests and t tests were conducted for categorical variables and continuous variables, respectively. Fisher's exact test was used when cells had an expected count of <5. For all tests, p<0.05 was considered statistically significant.
The annual incidence of wrTBI was calculated by dividing the number of claimants with TBI by the total number of workers and expressed as a rate per 100 000. Since the proportion of full-time workers differed significantly by sex, incidence was also calculated among full-time workers alone. In addition, sex-specific and industry-specific rates were determined as an average over the 8-year period, and risk ratios (RR) were computed for males relative to females, with 95% CI. Denominators used for the rate calculations were derived from Labour Force Survey data provided by the Australian Bureau of Statistics.29 The proportion of wrTBI among all work-related injuries/illnesses was also determined, using the total number of claims as the denominator. Time trends over the 8-year period were assessed using negative binomial regression. All analyses were performed using SAS V.9.3.
Results
During the period 2004–2011, a total of 4186 workers, including 2661 (63.6%) males and 1525 (36.4%) females, lodged a claim for wrTBI. This represented ∼1% of all claims lodged during the study period. Of all wrTBI cases, 74 (1.8%) resulted in death, most of which involved males (93%). The incidence rate of wrTBI was averaged at 19.8/100 000 workers per year. Sex-specific rates were estimated at 22.9/100 000 and 16.0/100 000 for males and females, respectively (RR 1.43, 95% CI 1.35 to 1.53).
Trends
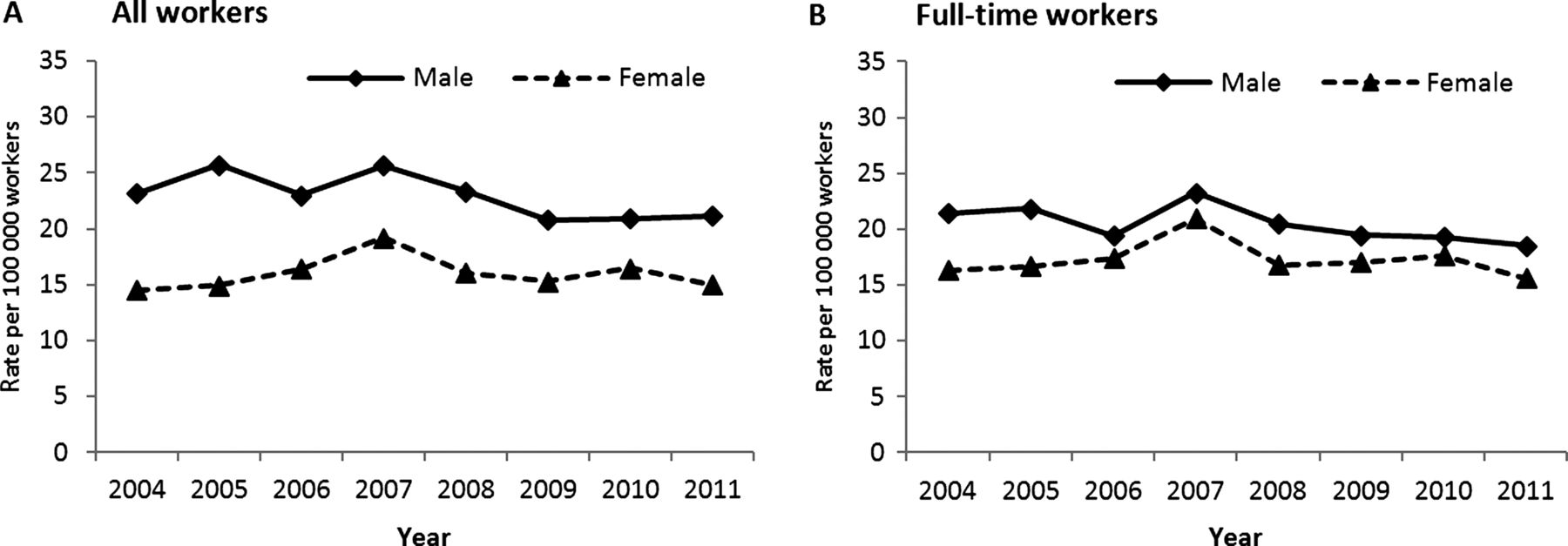
Figure 1 displays the trend of wrTBI over the 8-year period. While rates in males fluctuated between 2004 and 2007, a steady increase was observed in females, from 14.5 to 19.2/100 000 (figure 1A). For both sexes, the rate of wrTBI peaked in 2007, followed by a decline. Similar patterns were observed among full-time workers (figure 1B), although the gap between the two sexes were notably narrower, especially since 2006. Overall, the rate of wrTBI among full-time males was 1.18 (95% CI 1.09 to 1.28) times that among full-time females. Additionally, while there was an overall decline in rates among male workers, from 23.2/100 000 in 2004 to 21.2/100 000 in 2011 (–2.5% per year, 95% CI –4.2 to –0.8, p=0.005), a small non-significant increase was observed in females, from 14.5 to 15.0/100 000 (p=0.865). Similar results were obtained for full-time workers. Furthermore, wrTBI accounted for a larger proportion of claims lodged by females compared to males for all years studied (data not shown), with an increasing trend found for males (0.7% to 1.2%, p<0.001) and females (0.8% to 1.4%, p<0.001) over the 8-year period.

{kind=link}
Incidence of work-related traumatic brain injury among (A) all workers and (B) full-time workers, Victoria, Australia, 2004–2011.
Preinjury demographic characteristics
Table 1 presents preinjury demographic characteristics of wrTBI cases. The mean age at injury was 38.9 years, and females were on average 1 year older than males (39.5 vs 38.5, p=0.029). For males, wrTBI occurred most frequently in those aged 25–34 years (24.8%), while the highest proportion of female cases were aged 45–54 years (27.3%). Compared to females, males had higher preinjury income and were more likely to have been working full-time and employed by small or medium-sized companies.
Preinjury demographic characteristics of claimants with work-related traumatic brain injury, stratified by sex, Victoria, Australia, 2004–2011
Male and female cases were significantly different in the distribution of occupation groups and industry sectors. Male cases worked predominantly as technicians/trade workers (23.6%), machinery operators/drivers (21.9%), or labourers (21.0%), while the majority of female cases were professionals (32.3%) or community/personal service workers (20.3%). An examination of occupation subgroups (data not shown) revealed that the most common occupations among male cases were truck drivers (8.4%), miscellaneous labourers (6.8%) and security officers/guards (5.2%), while the largest proportion of female cases were secondary school teachers (9.9%), primary school teachers (6.1%) and registered nurses (5.6%). Furthermore, wrTBI among males occurred most frequently in manufacturing (17.1%), transport/postal/warehousing (13.1%) and construction (12.7%) industries, while nearly half of female cases worked in education/training (28.1%) and healthcare/social assistance (20.3%).
Industry-specific rates
Table 2 reports industry-specific rates of wrTBI among all workers and full-time workers. For both sexes, the highest and lowest rates were observed for arts/recreation and financial/insurance services, respectively. Transport/postal/warehousing, education/training, public administration/safety and mining sectors also experienced some of the highest rates overall and for full-time workers. Among all workers, males were more likely to sustain wrTBI than females across most industries, with the largest ratio estimated for construction (RR 4.45, 95% CI 2.37 to 8.35) and rental/hiring/real estate services (RR 3.11, 95% CI 1.42 to 6.83). Meanwhile, males working in professional/scientific/technical services (RR 0.64, 95% CI 0.44 to 0.93) and education/training (RR 0.77, 95% CI 0.64 to 0.93) had significantly lower rates compared to females working in these sectors. When analyses were restricted to full-time workers, similar patterns were observed, as males still had higher rates across most industries and significantly lower rates in professional/scientific/technical services and education/training compared to females. However, male-to-female ratios were attenuated or no longer significant for several sectors, particularly construction (RR 1.65, 95% CI 0.88 to 3.11).
Incidence rate of work-related traumatic brain injury by industry sector and sex among all workers and full-time workers, Victoria, Australia, 2004–2011
Injury characteristics
Table 3 presents injury characteristics of wrTBI cases. Overall, the most common mechanism of injury was struck by/against (53.1%), followed by falls (23.7%), assaults/violence (12.5%) and motor vehicle collisions (MVC; 7.2%). Struck by/against and falls accounted for significantly higher proportions of wrTBIs among females than males, while assaults/violence and MVC were more common in males. Additionally, compared to males, females were more likely to have been struck unintentionally by a person or against stationary objects. The type of fall also differed by sex, with most falls occurring from a height for males and at the same level for females.
Injury characteristics of claimants with work-related traumatic brain injury, stratified by sex, Victoria, Australia, 2004–2011
Further analyses of injury mechanisms by age group (see online supplementary figure S1) showed that for both sexes, the percentage of falls increased with age, replacing struck by/against as the most common cause of wrTBI in older workers, particularly among females aged ≥55 years. Assault-related wrTBI occurred most frequently in younger males and middle-aged females. MVC were slightly more common among older males, while no significant age differences were observed in females. With the exception of those aged 35–44 years, the distribution of injury mechanisms differed significantly by sex within all age groups (p<0.02). Moreover, when stratified by industry (data not shown), struck by/against was the most common cause of injury across almost all sectors for both sexes, except for a large proportion of males in public administration/safety (eg, police) sustaining wrTBI due to assaults/violence (57%). Similarly, falls was the second most common injury mechanism across most industries, with particularly high proportions among males in construction (37%) and females in education/training (26%).
As shown in table 3, the most common agencies of wrTBI were unpowered tools/equipment (26.1%), animals/humans (21.6%), and materials and objects (18.0%). Compared to males, injuries among females were more likely to have involved unpowered tools/equipment, while injuries involving machinery/fixed plant and mobile plant/transport were more common among males. Environmental agencies, such as slippery conditions and surfaces with hazardous objects, also accounted for a larger proportion of wrTBIs among females than males (18.2% vs 11.6%). For both sexes, 16% of wrTBIs occurred as a result of actions of another person, while animals contributed to ∼5% of all injuries.
The distribution of wrTBI cases by season and month was almost identical for males and females, with the highest occurrence in winter (26.9%) and the lowest in summer (21.5%). Specifically, the number of cases peaked in the months of May and August. In terms of wrTBI trends by day of the week, the highest frequency of injuries occurred on Tuesday (19.2%), after which a gradual decline was observed through to Friday (16.1%). Similar trends were observed for both sexes, although more males were injured during the weekend, particularly on Sunday.
Outcomes
Outcomes of wrTBI are presented in table 4. Among all claimants, 74.5% had lost time from work. While this proportion did not differ significantly by sex, wrTBI among males were more likely to result in inpatient hospitalisation (21.8% vs 9.9%, p<0.001) and work disability exceeding 10 days (27.7% vs 18.2%, p<0.001) compared to females. Among claimants with >10 days off work, the duration of work disability for males averaged nearly 40 days longer than females, although the difference was not statistically significant (229 vs 191 days, p=0.115). Moreover, wrTBI claims among males were associated with significantly higher costs compared to females for all cost types examined and across all claim types. Overall, the mean total cost per claim for male claimants ($A 39 963) was nearly four times that for females ($A 10 285).
Outcomes of work-related traumatic brain injury by sex and claim type, Victoria, Australia, 2004–2011
Discussion
This study provides the first epidemiologic profile of wrTBI in Australia and the first detailed examination of wrTBI with a sex/gender focus. Using workers’ compensation claims data spanning 8 years, we estimated wrTBI incidence by sex and industry sector in a statewide population and noted sex differences in terms of demographic, occupational and injury characteristics, as well as outcomes. Unlike studies using trauma registry or death records,4 ,6 ,7 ,14 in which females accounted for <10% of wrTBI cases, over one-third (36.4%) of wrTBIs were sustained by females in our study. This is most comparable to an Ontario-based study, in which 42% of claims for wrTBI across a range of severity levels involved females.9 Additionally, in agreement with previous findings,4 ,10 ,14 ,30 we showed that males were at higher risk of wrTBI than females (RR 1.4). However, the sex difference observed here is much smaller compared to those reported in the USA for hospitalised (RR 6.3)30 and fatal (RR 15.0)14 wrTBI, suggesting that while male workers are at higher risk of severe/fatal injuries, females may be almost as likely to sustain wrTBI when milder injuries are captured. This is also supported by our results on wrTBI outcomes, which indicate that males were more likely to be hospitalised and have longer duration of work disability compared to females.
Our study is one of the very few that has examined time trends of wrTBI. Overall, a small decline in wrTBI rates was observed in Victoria during the 8-year period, specifically in males. In addition, although rates in males were consistently higher compared to females, the gap between the two sexes has narrowed over time. Our findings are somewhat consistent with the downward trend in overall claim rates reported in Victoria22 and nationally,16 where males experienced a greater decrease in work-related injury/illness rates. The narrowing of the gender gap in wrTBI also corresponds with patterns observed in overall claim rates,16 possibly reflecting the shift of women into more physically demanding jobs. It should also be noted that fluctuations in rates, particularly changes observed around year 2007, may reflect changes in legislation, coding guidelines and reporting practices, in addition to workplace factors (eg, job tasks, safety standards).22 ,31 However, further investigation may be needed, as we are not aware of any major changes during this period. Furthermore, the trends observed in this study, including the closing gender gap, are unique to TBI occurring at work, as TBI rates in the general Australian population remained relatively stable over time, with no notable changes by sex.2 Future research should continue to assess long-term trends in wrTBI, stratified by sex, age and industry, in order to identify specific needs for targeted prevention.
Our results revealed significant sex differences in the distribution and rates of wrTBI by industry sector. While male cases were concentrated in occupations or industries normally associated with physical labour and/or hazardous work conditions, most female cases occurred in service industries, such as healthcare and education. These findings are similar to those of the Ontario study,9 although direct comparisons are difficult due to differences in workforce composition, workers’ compensation systems and industry classifications. Moreover, consistent with a US study exploring gender differences in work-related injuries/illnesses,18 we found that males were at higher risk of wrTBI than females across most industry sectors. As suggested by others,18 ,19 ,32 differential participation in physically demanding occupations as well as dissimilar job tasks and work exposure patterns, even within the same occupations, likely accounted for the sex disparity. Furthermore, since males were more likely to work full-time, the length of work exposure may also explain some of the sex differences in wrTBI rates, as demonstrated in our analyses restricted to full-time workers. As expected, we found smaller sex differences among full-time workers compared to all workers, in terms of time trends and within certain industry sectors where employment status differed significantly by sex (ie, construction). Nevertheless, regardless of full-time status, males remained at significantly higher risk of wrTBI compared to females in several industries, such as transport/postal/warehousing and public administration/safety. This again highlights the need to examine gender-specific job tasks and exposures contributing to wrTBI. Furthermore, the finding that females in education/training and professional/scientific/technical services were at higher risk of wrTBI than males is interesting and warrants further exploration. Since these industries are not normally associated with high physical demands, the sex disparity in injury rates may be explained, at least in part by, gender differences in psychosocial risk factors, such as workplace culture and mental exhaustion or stress.21 ,33 For instance, women in education and research sectors are known to experience higher levels of work-related stress, which could predispose them to greater risk of injury, compared to men.33
While our results reaffirm the high incidence of wrTBI among transport/warehousing, public administration/safety, and mining industries as reported by others,4 ,9 ,14 we also highlight wrTBI occurrence in previously less recognised industry sectors. In particular, we found a large burden of wrTBI, in terms of numbers and rates, in the education/training sector. Kristman et al15 also noted a high prevalence of mild TBI among education workers in Ontario. These findings suggest the need to identify risk factors contributing to wrTBI in the education environment, including potential sex differences as noted earlier. Furthermore, contrary to previous studies,4 ,14 we observed the highest rate of wrTBI among the arts/recreation services sector. This unique finding may be associated with the large professional football and horse racing industries in Australia. Specifically, using workers’ compensation claims data from the VWA, Cowley et al34 found that intracranial injuries accounted for >10% of claims filed by workers, including jockeys, in the Victorian thoroughbred racing industry.
In terms of injury mechanism, while most previous studies identified falls as the leading cause of wrTBI,4–6 11–13 ,30 our results indicate that struck by/against accounted for the greatest proportion of wrTBI among both sexes and across most age groups and industries. These findings most resemble the Ontario study,9 likely because both studies examined wrTBI across a broader range of severity, suggesting that struck by/against may be a more common cause of milder forms of wrTBI relatively to falls and MVC. Sex and age differences in the distribution of mechanism/agency of injury may also reflect differential job exposures and should be taken into consideration in prevention programmes. Moreover, age-related trends observed in the occurrence of wrTBI caused by falls coincide with other studies4 ,9 ,14 and may be associated with pre-existing comorbidities and medication use that make older workers, particularly females, more prone to falling.35
Our results demonstrate substantial work disability and economic burdens associated with wrTBI. In agreement with previous work,9 wrTBI sustained by males resulted in longer duration of work disability and higher claim costs compared to females, likely explained by sex differences in injury severity as well as preinjury earnings and employment status. Notably, average costs per wrTBI claim estimated in our study, including income replacement and medical costs, are greater than those reported for all work-related injuries/illnesses in Victoria.24 However, among claimants with >10 days off work, wrTBI resulted in slightly shorter median duration of work disability (51 days) compared to work-related injuries/illnesses overall (59 days).36 To investigate these discrepancies and to further assess long-term impacts of wrTBI, future studies should examine return-to-work outcomes as well as healthcare and disability service utilisation.36 ,37
This study has several limitations. First, the criteria used for ascertaining wrTBI cases have not been validated, and as our analyses relied on an administrative database, detailed information on clinical diagnoses, including injury severity, was not available. However, since the database contained detailed compensation payment information, we expect the coding of injuries to be relatively accurate. Given the possibility of linkage to clinical data, future studies should assess the validity of TOOCS codes in wrTBI case identification using a similar approach described by Sears et al.13 Additionally, since time-loss from work is a poor proxy for injury severity due to its association with various personal and workplace factors, the inclusion of validated severity measures (eg, Glasgow Coma Scale) in the data is needed to improve the characterisation of wrTBI. Second, since the compensation system identifies the most serious injury sustained by the worker, any mild TBI co-occurring with more severe injuries would not have been captured in our study. Similarly, based on the eligibility criteria for compensation, only injuries involving time off work and/or medical expenses were included in the data. As a result, milder injuries are likely underestimated, thus limiting generalisability of our findings to a more severe subset of injuries. Cases may be also missed due to under-reporting, which is associated with factors such as stigma, fear of reprisal and lack of awareness of the compensation system.38 Moreover, depending on the circumstances of death, fatalities could have also been under-represented in workers’ compensation claims data, as demonstrated previously.39 Together, these factors likely contributed to an undercount of wrTBI cases, and thus a conservative estimate of incidence, in our study. Third, the VWA does not provide population coverage of all workers in Victoria as noted earlier, resulting in further underestimation of wrTBI rates, since denominators from the Australian Bureau of Statistics are based on the entire Victorian labour force. This may also reduce the generalisability of our findings, as workers not insured by the VWA may have different employment characteristics and work exposures compared to the overall working population. Fourth, we were not able to use work hours as a denominator in the rate calculations, although analyses restricted to full-time workers provided some adjustment for the length of work exposure. Finally, since the VWA does not keep track of employer payments, we could not provide a more comprehensive estimate of work disability and costs associated with wrTBI.
In conclusion, this study contributes new knowledge on the epidemiology of wrTBI through a gender perspective. Sex-based analyses revealed substantial differences between males and females in terms of demographics, injury characteristics, and outcomes of wrTBI. While claim rates for work-related injuries/illness decreased over time, relatively little improvement was seen in wrTBI rates over the 8-year period, with a closing gap observed between the two sexes. Furthermore, although females were at lower risk of wrTBI compared to males across most industries, higher rates were observed among females in education/training and professional/scientific/technical services. Our findings also highlight the arts/recreation sector as a potential target for prevention in the Australian context. Although further research is needed to better understand the sex disparities observed, recognition of such differences is essential for developing tailored approaches in injury prevention and reduction of work disability and economic burdens associated with wrTBI.
Acknowledgments
The authors would like to thank the staff at the Institute for Safety, Compensation and Recovery Research for data preparation. The authors also thank Kaye Chen, Pravheen Thurairajah and Gurjit Toor for providing helpful tips for the analysis, Vincy Chan for assistance in study design and Sandra Sokoloff for administrative support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors VCC conducted the analysis of data and drafted the initial manuscript. All authors contributed to the conception and design of the study, as well as the interpretation of data and all authors made critical editorial contributions and approved the final version of the manuscript submitted.
-
Funding This study, including support for Dr. Colantonio and Ms. Chang, was funded by the Canadian Institutes of Health Research (grant #494372). Data for the analysis conducted was provided by the Victorian WorkCover Authority via a grant to the Institute for Safety, Compensation and Recovery Research.
-
Competing interests None.
-
Ethics approval This study was approved by the Health Sciences Research Ethics Board of the University of Toronto and the Monash University Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.