Article Text

Abstract
Objective Cleaning products may cause work-related asthma, but information regarding the specific exposures involved is scarce. We aimed to determine the associations between asthma and occupational exposure to cleaning agents in hospital workers.
Methods Analyses were conducted in 179 (136 women) hospital workers and a reference population of 545 subjects (18–79 years) from the French case-control and familial Epidemiological study on the Genetics and Environment of Asthma (2003–2007). Exposures to cleaning agents were estimated using three methods: self-report, expert assessment and an asthma-specific job-exposure matrix (JEM). Associations between cleaning products and current asthma were evaluated by logistic regressions, stratified by sex and adjusted for age and smoking status.
Results According to expert assessment, 55% of male and 81% of female hospital workers were exposed to cleaning/disinfecting tasks weekly (p<0.001). No association was observed between cleaning/disinfecting tasks and current asthma in men or in women whatever the assessment method used. In women, exposure to decalcifiers (expert assessment) was associated with current asthma (OR (95% CI):2.38 (1.06 to 5.33)). In hospital workers classified as exposed according to both the expert assessment and the JEM, additional associations were observed for exposure to ammonia (3.05 (1.19 to 7.82)) and to sprays with moderate/high intensity (2.87 (1.02 to 8.11)).
Conclusions Female hospital workers are often exposed to numerous cleaning products, some of which were markedly associated with current asthma. Low numbers prevented a meaningful analysis in men. Objective and more accurate estimates of occupational exposure to cleaning products are needed to better understand the adverse effects of cleaning products.
Statistics from Altmetric.com
What this study adds
-
Hospital workers, especially women, experience high exposure level to a wide range of cleaning/disinfecting products suspected to play a role in work-related asthma. Previous studies of this relationship largely relied on self-reported exposure.
-
Using an expert assessment alone or combined with an asthma-specific job-exposure matrix, we observed in women associations between current asthma and exposure to decalcifiers, products in spray form and ammonia.
-
Personal care workers and cleaners in hospital appeared as a high risk group for asthma related to cleaning products.
Introduction
There is growing evidence of a deleterious role of cleaning and disinfecting products in asthma and respiratory disorders.1 ,2 Exposure to cleaning and disinfecting products is common, both at the workplace in various occupations and industries and at home during domestic cleaning.2 Healthcare professionals and hospital workers may experience particularly high exposure level to a wide range of cleaning/disinfecting tasks and products,3 in the frame of prevention against healthcare-related infections. Healthcare workers were identified as an occupational group at risk for asthma in population-based4–6 and surveillance studies.7–9 Among healthcare workers with work-related asthma, cleaning and disinfecting products were the most frequently reported agents associated with symptoms.8 ,9 Occupational exposures to cleaning agents were associated with new-onset asthma in nursing professionals,10 ,11 with work-related and work-exacerbated asthma symptoms in healthcare professionals12 and with current asthma in hospital cleaners.13
Most cleaning products suspected to be associated with asthma are assumed to act as respiratory irritants (eg, bleach, ammonia, formaldehyde) but some have sensitising potential (eg, formaldehyde, perfumed products).2 ,12–15 The role of products used in spray-form has been emphasised as well,11 ,16–18 with possibly both irritant and sensitising mechanisms. However, determining the specific tasks and products causing asthma onset or symptoms remains a challenge, partly because of issues related to exposure assessment.3 ,19 Self-report has been widely used in studies of occupational or domestic cleaning and asthma. However, it has been recently shown in the Epidemiological study on the Genetics and Environment of Asthma (EGEA)20 that hospital workers underestimated their occupational exposure to cleaning products as compared with an expert assessment. Furthermore, the possibility of differential misclassification has been suggested.20 ,21 An asthma-specific job-exposure matrix (asthma JEM)22 also provides estimates of exposure to various asthmogens including industrial cleaning/disinfecting products. The asthma JEM was designed to favour specificity over sensitivity22 as recommended especially when exposure prevalence is low.23 Associations between exposure to cleaning products estimated by the asthma JEM and new-onset asthma5 and severe asthma24 have been observed, but this JEM does not provide assessment of exposure to specific cleaning tasks and products.
Occupational exposure to cleaning was assessed in hospital workers using three methods: a detailed job-specific questionnaire, an expert assessment20 and the asthma JEM.22 The aim of the current study was to determine the associations between lifetime exposure to cleaning tasks and various cleaning products in hospital workers and current asthma. For this purpose, the three exposure assessment methods were used, independently and combined.
Material and methods
Population
The French EGEA combines a case-control and family-based study25: at the baseline study (EGEA1, 1991–1995, 2047 participants), adult and child cases with asthma were recruited in chest clinics in five French cities. First degree relatives of cases were invited to participate in the study and population based controls were recruited through electoral rolls for adults and in surgery department for children. The study protocol was approved by the institutional ethics committee and all participants gave written informed consent. The current analysis used the data from the follow-up (EGEA2, 2003–2007). At EGEA2, 92% of the initial population answered a brief postal questionnaire (see online supplementary figure E1). More detailed information was recorded for 1601 subjects (77% of the initial population+58 new family members not examined at baseline). Among the 1571 adult participants, occupational data was available for 1477 subjects. Subjects with noncurrent asthma (n=102), aged less than 18 years (n=3), or with missing data (n=17) for the main variable of interest (current asthma) or potential confounder (smoking habits) were excluded from the analyses. Out of the remaining 1355 subjects, subjects who had ever worked in hospital and a reference population (described below) have been selected for the analyses.
Asthma definition
Asthma characteristics were recorded in standardised international questionnaires. Subjects with asthma were cases recruited at baseline in chest clinics according to a standardised procedure,25 as well as family members or population-based controls who answered positively to one of the two standardised questions: ‘have you ever had attacks of breathlessness at rest with wheezing?’ or ‘have you ever had asthma attacks?’. Current asthma was defined as ever asthma (at EGEA1 or EGEA2) and report of asthma attacks, respiratory symptoms or asthma treatment in the last 12 months, as previously in EGEA26 and in the European Community Respiratory Health Survey (ECRHS).27
Occupational exposure
A complete occupational history was recorded by questionnaire. For each job (with duration ≥3 months) or training period (with duration ≥1 month) reported, position, industry and job task were precisely recorded, and a 4-digit code according to the International Standard Classification of Occupation 1988 (ISCO-88) was assigned by an experienced coder.28 Hospital workers and cleaners were further asked to answer job-specific questionnaires regarding exposure to cleaning/disinfecting tasks and products, and an expert assessment of exposure was conducted in 179 (43 men, 136 women) hospital workers (healthcare workers or cleaners in hospitals).20
Estimation of exposure to various cleaning/disinfecting products by self-report in hospital workers
The two job-specific questionnaires for healthcare workers and cleaners have been previously described in EGEA20 and were adapted from the ECRHS questionnaire.11 Briefly, questions regarded the frequency (never, <1 day/week, 1–3 days/week, 4–7 days/week) of cleaning/disinfecting tasks, use of cleaning/disinfecting products and use of latex gloves (healthcare workers only) in the relevant jobs. The participants who had several jobs with similar tasks completed the specific questionnaire only once for all similar jobs. In the current study, subjects were classified as exposed to a given task or product according to self-report if the exposure frequency was greater than or equal to once a week, for at least one of the reported jobs.
Estimation of exposure to various cleaning/disinfecting products by expert assessment in hospital workers
The expert assessment was conducted in hospital workers by an occupational hygienist and two occupational physicians from French hospitals. The assessment procedure has been described previously.20 Briefly, the probability (non-exposed, <0.5, >0.5, 1), frequency (non-exposed, <1 day/month, <1 day/week, 1–3 days/week, 4–7 days/week) and intensity (non-exposed, environmental, low, moderate, high) of exposure to cleaning/disinfecting tasks and to 18 specific products were estimated based on job category, hospital unit and calendar year. Self-reported exposure from the specific questionnaire was taken into account in the expert decision as well. In the current study, subjects were classified as exposed to a given task or product if the estimated exposure probability was greater than or equal to 0.5, and if the exposure frequency was greater than or equal to once a week, for at least one of the reported jobs.
Estimation of exposure cleaning/disinfecting agents by the asthma JEM in all workers
The asthma-specific JEM was set up in the context of the EGEA1 study,22 and has since been largely used in the literature (http://cesp.vjf.inserm.fr/asthmajem). The asthma JEM provides an evaluation (yes/no) of exposure to a list of 22 agents a priori classified as at high or low risk for asthma. To improve exposure assessment, the application of the JEM included an occupational hygiene expert re-evaluation step: occupational exposure or job codes were checked independently by three experts for 28% of all jobs/training periods (in the whole dataset). For jobs with at least one disagreement between experts, the final decision was taken by consensus. In the current study, the asthma JEM was used to estimate lifetime exposure to industrial cleaning/disinfecting products and to latex (2 of the 22 listed agents of the JEM) in all subjects.
Estimation of potential exposure to cleaning/disinfecting agents by experts in all workers
In addition, potential exposure to cleaning/disinfecting products (yes/no) was evaluated in all subjects by two other experts based on task description in the main occupational questionnaire, available for all workers.20 As in this case only limited information regarding tasks was available, this definition of exposure had a low specificity, and was used only to exclude subjects with potential exposure from the reference category (see below).
Reference category
In the current study, the reference category (non exposed subjects) corresponded to subjects classified as never exposed according to each of the four following estimation methods: (1) self-report in job-specific questionnaires for healthcare workers or cleaners; (2) expert assessment in hospital workers; (3) evaluation of potential exposure to cleaning/disinfecting products in all subjects by two experts; (4) asthma JEM (any of the 22 agents). Based on these criteria, the reference group consisted in 545 (212 men, 333 women) subjects without any occupational exposure suspected to be related to asthma.
Statistical analyses
Associations between current asthma and various cleaning/disinfecting products were studied, using estimation of exposure derived from (1) self-report, (2) the expert assessment and (3) the asthma JEM in hospital workers. Analyses were performed for specific products for which at least five subjects with asthma were exposed.22 According to the expert assessment, 10 products (listed in table 2) fulfilled this condition. According to self-report, only four products (bleach, formaldehyde, alcohol, sprays) were analysed, as exposures to Dakin's solution, chlorexidine, glycol ether and decalcifiers were not assessed by self-report, and exposure to quaternary ammonium compounds and ammonia were reported by too few subjects.
Using information from the expert assessment, analyses have been conducted to determine how the associations with asthma varied with frequency or intensity of exposure, and the number of different products used. Additionally, associations between current asthma and cleaning products in hospital workers classified as exposed according to both the expert assessment and the asthma JEM (industrial cleaning agents) have been assessed.
Exposure to latex was analysed separately and the results are presented in the online supplementary file.
Analyses were stratified by sex. For most analyses, too few men were exposed to be studied separately, and results are presented mainly in women. Associations were adjusted for age and smoking status. Further adjustment and effect modification by Body Mass Index (BMI) has been tested in women but led to similar results (not shown). Associations have been evaluated by logistic regression and using a Generalised Estimating Equation approach to account for the familial structure of the data. Analyses have been performed using SAS 9.1.
Results
The subjects were aged on average 44.7 years, and subjects with current asthma were significantly younger than subjects without asthma (p<0.001). Detailed clinical characteristics according to asthma status are presented in supplementary table E1. Women working in hospital were significantly less often overweight than women from the reference population, and had similar age and smoking habits (table 1). In men, hospital workers differed from the reference population only in age (p=0.06).
Description of the population
According to self-report, 88% of the women and 80% of the men working in hospital were exposed weekly to cleaning/disinfecting tasks (p=0.19). According to expert assessment, these proportions were respectively 81% and 55% (p<0.001). Among those exposed weekly, women were exposed at higher frequency (80% women exposed 4–7 days/week vs 68% men, p=0.22) and at significantly higher intensity (57% women with moderate to high intensity vs 23% men, p=0.004) compared with men.
According to the asthma JEM, 44 women (32.4%) and seven men (16.3%) working in hospital were classified as exposed to industrial cleaning agents. Most of them (76.5%) were ‘institution based personal care workers’ (ISCO-88 classification), and the others (23.5%) were ‘helpers and cleaners in offices, hotels and other establishments’. Overall, the subgroup of women classified as exposed according to the asthma JEM was more often exposed (according to expert assessment) to cleaning/disinfecting tasks (93% weekly) than those not classified as exposed by the asthma JEM (75% weekly, p=0.01). A significant difference between these two groups was observed for the use (>1 day/week) of decalcifiers (50% vs 2%, p<0.0001), ammonia (41% vs 10%, p<0.0001), chlorexidine (45% vs 16%, p=0.001), sprays (59% vs 36%, p=0.01), bleach (60% vs 41%, p=0.04), and Dakin's solution (29% vs 14%, p=0.05).
Cleaning/disinfecting tasks and products and current asthma
In men, no association was observed between exposure to cleaning/disinfecting tasks and current asthma, according to self-report (OR (95% CI): 0.73 (0.34 to 1.58)) or expert assessment (0.62 (0.23 to 1.66)). Too few subjects were exposed according to the asthma JEM to perform separate analyses for men.
In women, cleaning/disinfecting tasks were not associated with current asthma, according to both self-report (1.14 (0.69 to 1.87)) and expert assessment (1.04 (0.64 to 1.70)). Exposure to cleaning products according to the asthma JEM was not significantly associated with current asthma (1.75 (0.87 to 3.52), p=0.12). Associations between specific cleaning products (according to self-report or expert assessment) and current asthma are presented in women (table 2). Exposure to decalcifiers estimated by the expert assessment was significantly associated with current asthma. No significant association was observed with any other cleaning product studied.
Associations between exposure to cleaning task and use of cleaning products according to self-report and expert assessment in hospital workers and current asthma in women
Level of exposure to cleaning/disinfecting tasks and products according to expert assessment and current asthma
In women, the number of different products used weekly (expert assessment) varied from one to nine (out of 10 products included), and the median was 4. No association was observed between the number of products used and current asthma (<4 products: 0.77 (0.39–1.56); >4 products: 1.11 (0.64–1.92)). Analyses taking into account the number of different products used at a moderate to high intensity did not show significant associations neither (not presented).
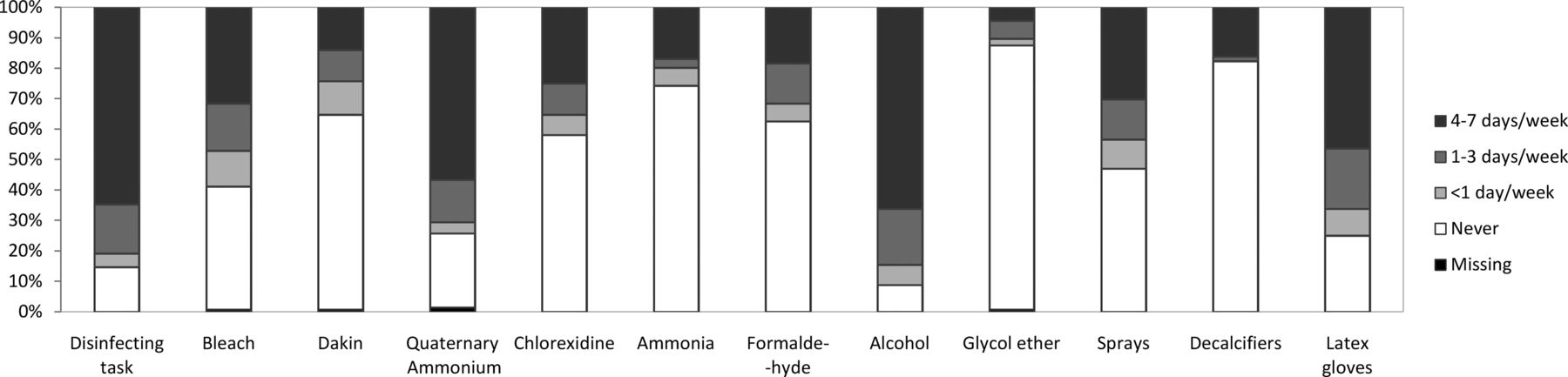
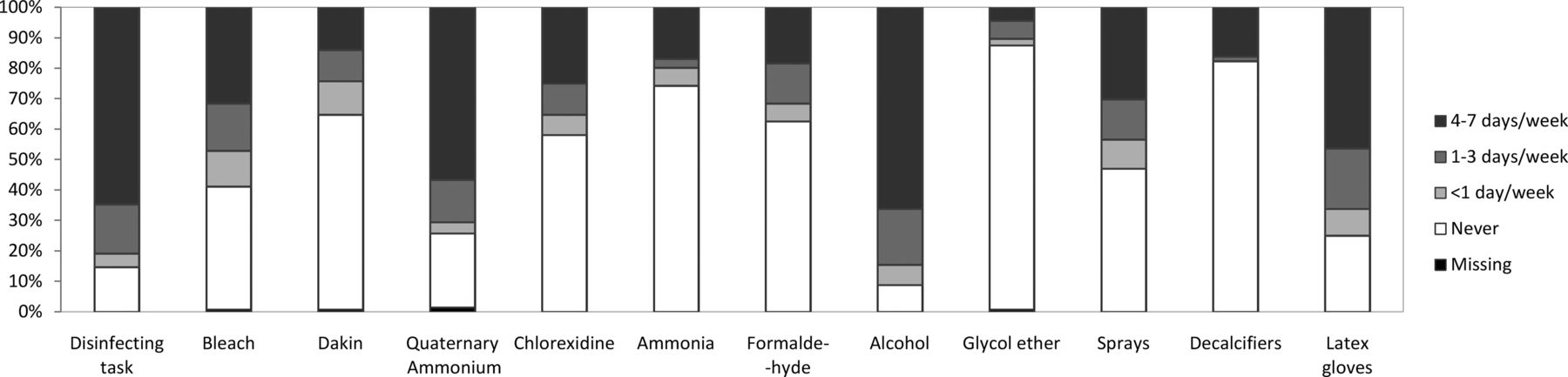
The frequency of cleaning task or use of cleaning products according to the expert assessment in the 136 female hospital workers is presented in figure 1. The products most commonly used according to the expert assessment were alcohol (84%) and quaternary ammonium compounds (71%). The highest frequency of exposure (4–7 days/week) was observed in most women classified as exposed (>1 day/week), for each task or product studied. In analyses of the associations between current asthma and exposure to cleaning tasks or products 4–7 days/week, only slightly higher and non-significant ORs were observed (not shown).
{kind=link}
Frequency of cleaning task or use of cleaning products according to expert assessment in female hospital workers. The expert assessment procedure has been described in detail by Donnay et al.20
In analyses taking intensity of exposure into account (table 3), OR were increased for moderate to high intensity of exposure to cleaning/disinfecting tasks, bleach, and quaternary ammonium compounds, and an OR of 2.06 was observed for sprays (p=0.10), but no significant association was observed. For ammonia and decalcifiers, all exposed subjects had a low intensity of exposure.
Associations between current asthma and intensity of exposure to cleaning task and products in female hospital workers, according to the expert assessment alone and combined with asthma JEM
Cleaning/disinfecting task and products and current asthma in hospital workers classified as exposed according to both the expert assessment and the asthma JEM
When limiting the exposed group to the subgroup of hospital workers classified as exposed according to both the expert assessment and the asthma JEM (industrial cleaning products), significant associations were observed between current asthma and exposure of moderate to high intensity to cleaning/disinfecting tasks (2.32 (1.11 to 4.86)) and sprays (2.87 (1.02 to 8.11), as shown in table 3. Exposures (of low intensity for all exposed subjects) to ammonia (3.05 (1.19 to 7.82)) and decalcifiers (2.32 (1.01 to 5.31)) were associated with current asthma as well. Although non-significant, ORs close to 2 were observed (see table 3) for exposure of moderate to high intensity to bleach (p=0.09) and quaternary ammonium compounds (p=0.12).
A similar analysis using a combination of self-report and the asthma JEM to assess occupational exposure is presented in (see supplementary table E2). Although no association reached significance, elevated OR were observed for the use of bleach and sprays.
Discussion
This study investigated the associations between current asthma and exposure to various cleaning and disinfecting products, using three exposure assessment methods: self-report, an expert assessment and a JEM, in female hospital workers. Exposure to decalcifiers estimated by expert assessment was associated with current asthma. In a subgroup of hospital workers, classified as exposed according to the asthma JEM and mainly constituted of personal care workers, marked associations were additionally observed between current asthma and general cleaning/disinfecting tasks, products in spray form and ammonia.
We used an expert assessment to estimate exposure to cleaning and disinfecting products for the first time. We also used the asthma JEM as a complementary method to refine exposure assessment. Self-reported exposure has been widely used in previous studies of the relationship between cleaning products and asthma. Using self-report allow covering a wide range of exposures over specific periods, but has important limits as it may rely on recall, personal knowledge, perception or health status of the subjects. In a previous study in EGEA,20 we showed that hospital workers (especially nurses, auxiliary nurses and cleaners) underestimated their occupational exposure as compared with the expert assessment, though variations were observed according to the type of cleaning products. Underestimation was particularly high for formaldehyde, ammonia and quaternary ammonium compounds. For these agents, self-reported exposure seems highly unreliable, and led in the current analysis to low numbers in the exposed groups, limiting the analyses using self-reports. Further, differential misclassification in self-reported exposure was shown,20 in particular for the use of bleach, underlying the relevance of expert assessment to study this product as well. In addition, the expert assessment provides a more complete evaluation of exposure, as it can include information regarding intensity of exposure, and exposure to some products which are not in the usual specific questionnaires. Expert assessment is often considered as the best individual-based approach to estimate occupational exposures in case-control studies,29 though its reliability strongly depends of the experts' competency, the available information regarding job and task description, and the studied agent.30 To our knowledge, no study investigated the validity of expert-assessment for cleaning products specifically. However, the approach chosen here was favourable to a good reliability: detailed information was available regarding work tasks, unit, periods, etc; assessment of hospital workers’ exposure was done in the experts’ area of expertise; and standardised decision rules were set up (see Ref. 20 for a more complete discussion). Yet, the expert assessment alone was probably not specific enough, and some products were associated with asthma only in those further classified as exposed by the JEM. The asthma JEM was designed to be highly specific and, to limit exposure misclassification, a job-by-job exposure re-evaluation step (for some jobs needing a check) was conducted.22 Although associations between exposure to asthmagens evaluated by the JEM (including cleaning products) and asthma have been observed in previous studies,5 ,24 the asthma JEM provided limited information regarding exposure (active chemical). A JEM focused on occupational exposure among hospital workers (including cleaning products) used previously in a U.S. population21 also remains with classification into broad categories.
Thus, regarding future research, improvement of occupational exposure assessment is warranted. The use of self-reported exposure alone is discouraged. In epidemiological studies of occupational risk factors for cancer, self-report is rarely used alone.29 ,30 Expert-assessment is expensive and hardly realisable in large studies, which are needed to properly evaluate the effects of the numerous chemical components of cleaning products. JEMs are an alternative, but designing a JEM efficiently assessing exposure to various specific cleaning products is challenging. Beyond practical questions, which of both methods (JEM or expert assessment) is the ‘best’ to evaluate occupational exposure is intensively debated, but comparison studies have been conducted mainly in the field of occupational cancer epidemiology, and the lack of gold-standard hampers a proper validation of each method. New methods to assess exposure to cleaning products need to be developed. Task-based assessments have shown that exposure level varied with both the product formulation and the application procedure.3 More studies are needed, including quantitative exposure measurement,19 to better determine which type of tasks, work practices, ambient environmental conditions and ventilation influence exposure levels.29 Such measurement may serve as gold-standard to evaluate the validity of existing methods, such as expert-assessment. They may further allow the development of convenient tools for application in larger epidemiological studies such as cleaning-specific JEM or, likely more efficient for cleaning products, task-exposure matrices.31
The associations observed in the current study may reflect occupational asthma as well as work-exacerbated asthma, which may both be related to cleaning exposure.2 ,8 ,12 Lifetime exposure was used rather than current exposure. This choice was related to power issue (few subjects were currently exposed to cleaning products), but also aimed to reduce the healthy worker survivor effect bias.32 However, estimation of exposure to various cleaning products was available only for jobs held at least 3 months. Thus, a possible selection of non-exposed jobs by subjects who were exposed during short-term occupations may have impacted the results.33 In addition, as subjects with childhood onset asthma were included, a healthy worker hire effect may be present,28 and some associations may be underestimated.32
In this study, exposure to cleaning products in hospital workers affected in large majority women. We considered that in studies of such gender-related activity, analyses stratified on gender were more relevant.34 ,35 Both the characteristics of exposure, even within a job,36 ,37 and effects resulting from exposure might differ between men and women. In men, no association between asthma and cleaning products was suggested, but a meaningful analysis was not possible because of low numbers. Few studies report associations between cleaning products and asthma separately in men and women,17 ,38 ,39 with varying results according to asthma definition, type of products or task studied.
In women, the use of decalcifiers, estimated by expert assessment, was associated with elevated risks of asthma in the current study. To our knowledge, this relationship has not been reported previously. Two studies based on self-reported exposure investigated the role of decalcifiers in asthma in subjects cleaning their own home17 or in women employed in domestic cleaning,16 and found no positive association. However, this relationship had never been investigated in healthcare workers. Decalcifiers are acids and may have irritative properties.14 ,40 The use of hydrochloric acid was associated with asthma symptoms in a previous study of cleaning workers.13 Mixing acids with bleach may results into serious inhalation accidents, a possible cause of acute irritant-induced asthma (also named reactive airway dysfunction syndrome). An effect of lower level but repeated exposure to irritants on asthma is also increasingly discussed.41 Whether product mixing was a common practice in hospital workers could hardly be evaluated by expert-assessment. Experience of serious inhalation accidents (to vapours, dust, gases or fumes) was assessed by questionnaire but was reported by only four hospital workers in our study.
Among hospital workers, subjects classified as exposed according to the asthma JEM were working as personal care workers or cleaners. In these workers, when combining information from the expert assessment and the JEM, an association with asthma was observed for high intensity of exposure to cleaning/disinfecting tasks overall. The association with decalcifiers was confirmed, and additionally, significant associations were observed for the use of sprays and ammonia, and associations were suggested with the use of bleach, and quaternary ammonium compounds. The relationship between the use of cleaning sprays and asthma has been reported previously, both in domestic17 ,18 and occupational setting.11 ,16 The high potential for inhalation exposure associated with product spraying was underlined in a study characterising qualitatively airborne exposures during cleaning tasks in hospital workers.3 In the current study, moderate to high intensity of exposure to cleaning sprays was associated with current asthma, consistently with a dose–response relationship previously observed for the use of cleaning sprays at home.17 Previous studies have reported associations between asthma and self-reported use of bleach and ammonia.11 ,12 ,16 Several case-report of occupational asthma related to quaternary ammonium compounds have been published,14 but this relationship has not been previously reported in epidemiological studies. However, as stated above, studies based on self-reported exposure may be inadequate for these agents. A surveillance study of work-related asthma trends in France over the period 2001–2009 showed a significant increase of cases of work-related asthma linked to quaternary ammonium compounds, particularly in healthcare workers.42 In the current study, numbers were low and the association with asthma did not reach significance, but the elevated OR (1.93) suggests that particular attention should be paid to these agents in future research.
In the current study, associations between cleaning products and asthma were not importantly modified after taking into account higher frequency of exposure and the number of different products used. Power issues have limited the possibility to investigate dose-response relationships. The fact that we observed associations with asthma mainly in the subgroup classified as exposed according to the JEM suggests that personal care workers (auxiliary nurses) and cleaners in hospital may constitute a high risk group for asthma related to cleaning products compared with other hospital workers. The highly specific assessment provided by the JEM (only jobs with high probability of exposure to industrial cleaning products were classified as exposed) may have favoured the detection of associations with asthma.23 Alternatively, the observed associations may be related to specific cleaning tasks and work environment3 associated with these jobs. A previous study in healthcare workers found similarly that nurses (with a large definition including for instance nurses’ aides) had an increased risk of asthma related to cleaning compared with other healthcare professionals.10
Multiple exposures are a complicating issue, which is particularly present in studies of occupational hazards in healthcare workers.43 Some of the associations we found might be inter-related with other exposures or observed by chance, and low numbers limited the possibility to address this point. However, as shown above, most of the observed associations are consistent with previous studies or with hypotheses formulated in the literature.
Conclusion
In conclusion, this study adds evidence to the burden of work-related asthma due to cleaning products. We have shown that female hospital workers, in particular personal care workers and cleaners, are exposed to numerous cleaning products, some of which were associated with current asthma. We used a combination of three methods to evaluate exposure (self-report, expert assessment, both based on responses to a detailed specific questionnaire and an asthma-specific JEM). The results strengthen evidence of a deleterious role of some agents (sprays, ammonia) previously observed in studies based only on self-reported exposure, and suggest associations not previously reported (decalcifiers). This study underlined the need for objective and more accurate estimates of occupational exposure to cleaning products, that take into account the specificity of each cleaning job and task, in order to progress in the understanding of the adverse respiratory effect of cleaning products.
Acknowledgments
EGEA cooperative group:
Coordination: F Kauffmann; F Demenais (genetics); I Pin (clinical aspects).
Respiratory epidemiology: Inserm U 700, Paris M Korobaeff (Egea1), F Neukirch (Egea1); Inserm U 707, Paris: I Annesi-Maesano; Inserm CESP/U 1018, Villejuif: F Kauffmann, N Le Moual, R Nadif, MP Oryszczyn; Inserm U 823, Grenoble: V Siroux
Genetics: Inserm U 393, Paris: J Feingold; Inserm U 946, Paris: E Bouzigon, F Demenais, MH Dizier; CNG, Evry: I Gut , M Lathrop.
Clinical centres: Grenoble: I Pin, C Pison; Lyon: D Ecochard (Egea1), F Gormand, Y Pacheco; Marseille: D Charpin (Egea1), D Vervloet; Montpellier: J Bousquet; Paris Cochin: A Lockhart (Egea1), R Matran (now in Lille); Paris Necker: E Paty, P Scheinmann; Paris-Trousseau: A Grimfeld, J Just.
Data and quality management: Inserm ex-U155 (Egea1): J Hochez; Inserm CESP/U 1018, Villejuif: N Le Moual, Inserm ex-U780: C Ravault; Inserm ex-U794: N Chateigner; Grenoble: J Ferran.
The authors thank all those who participated to the setting of the study and on the various aspects of the examinations involved: interviewers, technicians for lung function testing and skin prick tests, blood sampling, IgE determinations, coders, those involved in quality control, data and sample management and all those who supervised the study in all centres. The authors are grateful to the three CIC-Inserm of Necker, Grenoble and Marseille who supported the study and in which subjects were examined. They thank M-A Denis (Hospices Civils de Lyon, Groupement hospitalier Est, Médecine du Personnel, Bron, France) and R Magis (Service Central de Medicine du Travail, AP-HP, Paris, France) for the expert assessment of exposure in hospital workers; J Fevotte (Institut de Veille Sanitaire, Département Santé Travail, Saint Maurice, France) and N Massin (INRS, Département Epidémiologie en Entreprise, Vandoeuvre-lès-Nancy, France) for the expert assessment of potential exposure to cleaning/disinfecting tasks in all subjects; and G Vasseur (Inserm U780, Villejuif, France) for job coding. They are indebted to all the individuals who participated without whom that study would not have been possible.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors OD, NLM and FK were involved in the conception, hypotheses delineation and design of the analysis strategy of the study. NLM and FK participated in the acquisition of the data. NLM, CD, DJJH and MH were involved as experts in the occupational exposure assessment. OD, CD, DJJH, MH, DC, NLM and FK participated in the data analysis and interpretation. OD, NLM and FK wrote the paper. CD, DJJH, MH and DC reviewed the paper and revised it critically. All authors approved the final version of the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval CPP Necker Hospital, Paris.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Funding French Agency of health safety, environment and work (AFSSET-EST-09-15); Hospital programme of clinical research (PHRC)—Paris; National Research Agency—Health environment, health-work programme (ANR-SEST 2005); Merck Sharp & Dohme (MSD); Isere committee against respiratory diseases (COMARES); French Ministry of foreign and European affairs/Netherland organisation for scientific research (NWO) Van Gogh programme for French Dutch cooperation; and the University Paris Sud 11 - ED420 doctoral grant.