Article Text

Abstract
Objectives We investigated the contribution of major coronary heart disease (CHD) risk factors and job strain to occupational class differences in CHD incidence in a pooled-cohort prospective study in northern Italy.
Methods 2964 men aged 25–74 from four northern Italian population-based cohorts were investigated at baseline and followed for first fatal or non-fatal CHD event (171 events). Standardised procedures were used for baseline risk factor measurements, follow-up and validation of CHD events. Four occupational classes were derived from the Erikson–Goldthorpe–Portocarero social class scheme: higher and lower professionals and administrators, non-manual workers, skilled and unskilled manual workers, and the self-employed. HRs were estimated with Cox models.
Results Among CHD-free subjects, with non-manual workers as the reference group, age-adjusted excess risks were found for professionals and administrators (+84%, p=0.02), the self-employed (+72%, p=0.04) and manual workers (+63%, p=0.04). The relationship was consistent across different CHD diagnostic categories. Adjusting for major risk factors only slightly reduced the reported excess risks. In a sub-sample of currently employed subjects, adjusting for major risk factors, sport physical activity and job strain reduced the excess risk for manual workers (relative change = −71.4%) but did not substantially modify the excess risks of professionals and administrators and the self-employed.
Conclusions In our study, we found higher CHD incidence rates for manual workers, professionals and administrators, and the self-employed, compared to non-manual workers. When the entire spectrum of job categories is considered, the job strain model helped explain the CHD excess risk for manual workers but not for other occupational classes.
- Cohort study
- coronary heart disease
- occupational class
- risk factors
- job stress, epidemiology
- cardiovascular
- stress
- longitudinal studies
Statistics from Altmetric.com
- Cohort study
- coronary heart disease
- occupational class
- risk factors
- job stress, epidemiology
- cardiovascular
- stress
- longitudinal studies
What this paper adds
No studies have investigated the relationship between coronary heart disease (CHD) incidence and occupational classes in southern Europe, where CHD rates are low.
Higher CHD rates were observed among manual workers (excess risk 84%), administrators, managers and professionals (excess risk 72%), and the self-employed (excess risk 63%).
The job demand/control model can explain most CHD risk excess (71%) in manual workers, but not in managers, business proprietors, professionals, owners of small businesses or artisans.
The Job Content Questionnaire needs further refinement to detect specific work stressors and health consequences when a wide range of job categories are considered.
Introduction
An inverse association between socio-economic status (SES) and cardiovascular disease (CVD) death rate has been observed since the second half of the 19th century in the UK1 and more recently in most industrialised countries.2–4 However, in many European countries, including Italy, the relative differences in coronary heart disease (CHD) death rates between social classes has not been declining in recent years,5 although one UK study does reveal such a decrease.6 Several studies7–11 have suggested that higher myocardial infarction case-fatality rates in lower social classes are a possible contributor to the observed SES differences in CHD mortality.
Since mortality rate is the combined effect of case-fatality and incidence, it is essential for prevention to investigate SES differences in CHD incidence.
The relatively few studies which have investigated the relationship between CHD incidence and occupational class12–20 all reported higher rates in lower occupational classes, with age-adjusted estimates of risk ratios ranging from 1.4114 to 2.26.17 Most of the studies used locally developed occupational classifications,12 13 16–20 making comparisons across populations difficult. None of these studies was conducted in southern Europe, where CHD incidence is lower21 and smaller social gradients in CHD and CVD mortalities have been reported.22 23 Most of the studies assessed the contribution of behavioural and biological risk factors to explain the observed associations, with only a few exploring the role of work exposures,12 15 the psychosocial work environment or job strain.18–20
Organisational constraints on the job and sedentary activity are the two most common work-related CVD risk factors in post-industrialised societies.24 Belkic et al25 reviewed 17 longitudinal, nine case–control and eight cross-sectional studies, and concluded that in men the evidence was strong and consistent for a link between job strain and CVD. Kivimaki et al,26 in their meta-analysis of cohort studies adopting either the job-strain model27 or the effort–reward imbalance model,28 estimated an overall 50% excess risk among employees with work stress. The evidence to establish these relationships in entrepreneurs, artisans and self-employed workers is lacking at present.
The objectives of our study are to report on occupational class differences in the 12-year incidence of CHD in men and to assess the contributions of major coronary risk factors and job strain. To this end, we examined four northern Italian population-based cohorts with a large variety of job titles in the public and private sectors.
Methods
The northern Italian cohorts
The Brianza area is characterised by high levels of industrialisation and urbanisation, with one of the highest average incomes in Italy. As part of the WHO-MONICA Project, a population survey in this region was carried out in each of the periods 1986–1987, 1989–1990 and 1993–1994 to assess coronary risk factor changes over time.29 In each survey a 10-year age- and gender-stratified random sample was drawn from municipality rolls among the 25–64-year-old residents of five towns. People enrolled in one survey were not included in subsequent ones. The participation rates in men were 69.6%, 67.8% and 69.0% for the three surveys, respectively.
The PAMELA Study was carried out in 1991–1992 to investigate the relationship between clinic and ambulatory blood pressure measurements at the population level.30 Subjects were selected using the same sampling procedures from the 25–74-year-old residents in the city of Monza, the largest town in Brianza. The participation rate in men was 65.4%, with a lower rate in the youngest decade (25–34 years, 54.1%). The current analysis includes men only due to the high prevalence of never-working women in our samples. As reported elsewhere,29 30 participating men did not show statistically significant differences in socio-demographic and major health conditions in comparison to survey-specific random samples of non-responders interviewed by telephone. Both the baseline screening and the follow-up for all the surveys were approved by the ethics committee of Monza Hospital.
Measurement of risk factors at baseline
Information on cardiovascular risk factors was collected at baseline, with strict adherence to the standardised procedures and quality standards of the WHO-MONICA Project (http://www.ktl.fi/publications/monica/manual/index.htm). Trained technicians measured blood pressure in sitting subjects at rest for at least 10 min, using a standard mercury sphygmomanometer equipped with either a 13 cm or a 17 cm cuff bladder. Systolic and diastolic blood pressure measurements were taken at the first and fifth phases of the Korotkoff sounds. The study variable is the average of two measurements, taken 5 min apart. Venous blood specimens were taken from the ante-cubital vein in fasting subjects (12 h or more), using a tourniquet if necessary. Specimens were refrigerated at −4°C and shipped within 4 h to the Department of Clinical Pathology at Desio Hospital, where serum total cholesterol and HDL-cholesterol were measured by an enzymatic method. HDL-cholesterol fraction was separated using the phosphotungstate-Mg2+ method. Blood glucose was determined on the same samples by an enzymatic method. A standardised interview was administered to participants by trained interviewers. Information on cigarette smoking was categorised as current smoker versus past/never smoker. Average daily consumption of wine, beer and spirits was categorised as teetotaller, up to four, four to eight, and more than eight drinks per day. Diabetes mellitus was defined on the basis of self-report, information on insulin and oral hypoglycemic treatment, or fasting blood glucose exceeding 126 mg/dl. Self-reported previous hospitalisation for myocardial infarction, unstable angina pectoris or cardiac revascularisation defined history of CHD. Two educational classes were derived by considering ≤ or > 10-year age group specific median of years of schooling.
A sport physical activity index was derived from the Baecke questionnaire,31 available for the last two MONICA surveys and the PAMELA study only. It was calculated from a combination of the intensity of the sport played (classified in three levels according to average energy expenditure: 0.76, 1.26 and 1.76 MJ/h), the amount of time per week the sport was played, and the proportion of the year in which the sport was played regularly. Job strain was measured using a previously validated Italian short version (13 items) of the Job Content Questionnaire (JCQ).32 Job strain was expressed as the ratio between psychological job demand (PJD, five items, range 12–48) and job control (or decision latitude, DL, six items, range 24–96) scores, dichotomised at the sample median (0.42).
Ascertainment of incident coronary events
The follow-up for fatal and non-fatal events was carried out to the end of 2002 for all cohorts. Vital status was actively investigated for all subjects, including those who moved to different towns. Death certificates were obtained from local health districts and coded according to the International Classification of Diseases, Ninth Revision (ICD-9). Vital status and death certificates were available for 99% of subjects. Cardiovascular mortality was defined by ICD-9 codes 390–459 as the underlying cause of death. Suspected coronary deaths were identified based on underlying cause of death ICD-9 codes 410–414, 798 and 799, or 250, 428 and 440 in association with 410–414 in secondary causes of death. Suspected non-fatal CHD events, with hospital discharge diagnosis codes (ICD-9) 410 or 411 and ICD-9 CM 36.0–9 codes for coronary surgery revascularisation, were ascertained through linkage to hospital records.33 All suspected acute coronary events were validated according to MONICA diagnostic criteria.21 The cohort-specific percentages of subjects lost to follow-up for fatal and non-fatal coronary events ranged between 1.8 and 2.4, with no differences between occupational classes.
Classification of occupational classes
The Erikson–Goldthorpe–Portocarero (EGP) class scheme is based on current employment status, or that of the last job (nine categories) and work sector (agriculture, industry, trades, services).34 35 For statistical power considerations, we aggregated the original EGP categories into four occupational groups: professionals, administrators, managers and proprietors, corresponding to EGP I and II; non-manual workers, corresponding to EGP IIIa, IIIb and V (higher and lower non-manual workers and foremen and technicians); manual workers: EGP VI, VIIa and VIIb (skilled, semiskilled and unskilled manual and agricultural workers); and self-employed: EGP IVa, IVb and IVc (small proprietors, the self-employed and farmers).
Statistical analysis
After excluding 40 people who were never employed or employed only in the armed forces (four incident CHD events), 193 people (19 events) with undeterminable occupational class, and 148 people (eight events) with missing values on any covariate of interest, the final study sample for CVD mortality analysis consisted of 3083 subjects (89% of the total sample). Age-adjusted CVD mortality rates among excluded and included subjects were similar at 3.4 and 2.3 per 1000 person-years, respectively (p=0.15). For analysis of CHD incidence, 119 people with a positive history of CHD at baseline were further excluded, reducing the sample size to 2964.
We calculated age-adjusted mean or prevalence values of major cardiovascular risk factors for each occupational group, using standard linear or logistic regression models, respectively.
Age-adjusted incidence rates for each occupational group were obtained from Poisson regression models. Age-adjusted HRs were estimated using Cox proportional hazard models, with the non-manual worker class as the reference group (the group with the lowest event rate). The proportional hazards assumption was formally tested by including an interaction term between occupational classes and the follow-up time, and it was not statistically significant at a 0.05 significance level. Potential cardiovascular risk factors that were associated with CHD in age-adjusted models were included in multivariate Cox models.
The change in age-adjusted HRs due to cardiovascular risk factors has been measured on the logarithmic scale as:
Where beta is the logarithm of the hazard ratio. A secondary analysis was carried out using the same methods on a sub-sample of currently employed subjects, free of CHD at baseline and with no missing data for sport physical activity or job strain (1441 subjects, 48 first CHD events).
Results
Median follow-up time was 12 years, and 95 cardiovascular deaths were observed (crude mortality rate: 2.64 per 1000 person-years). Among individuals free from CHD at baseline, 171 incident CHD events were observed (incidence rate: 5.04 per 1000 person-years): 27 coronary deaths (definite or possible fatal MONICA validated myocardial infarctions and sudden cardiac deaths), 71 MONICA definite myocardial infarctions and 73 MONICA possible myocardial infarctions or coronary revascularisations.
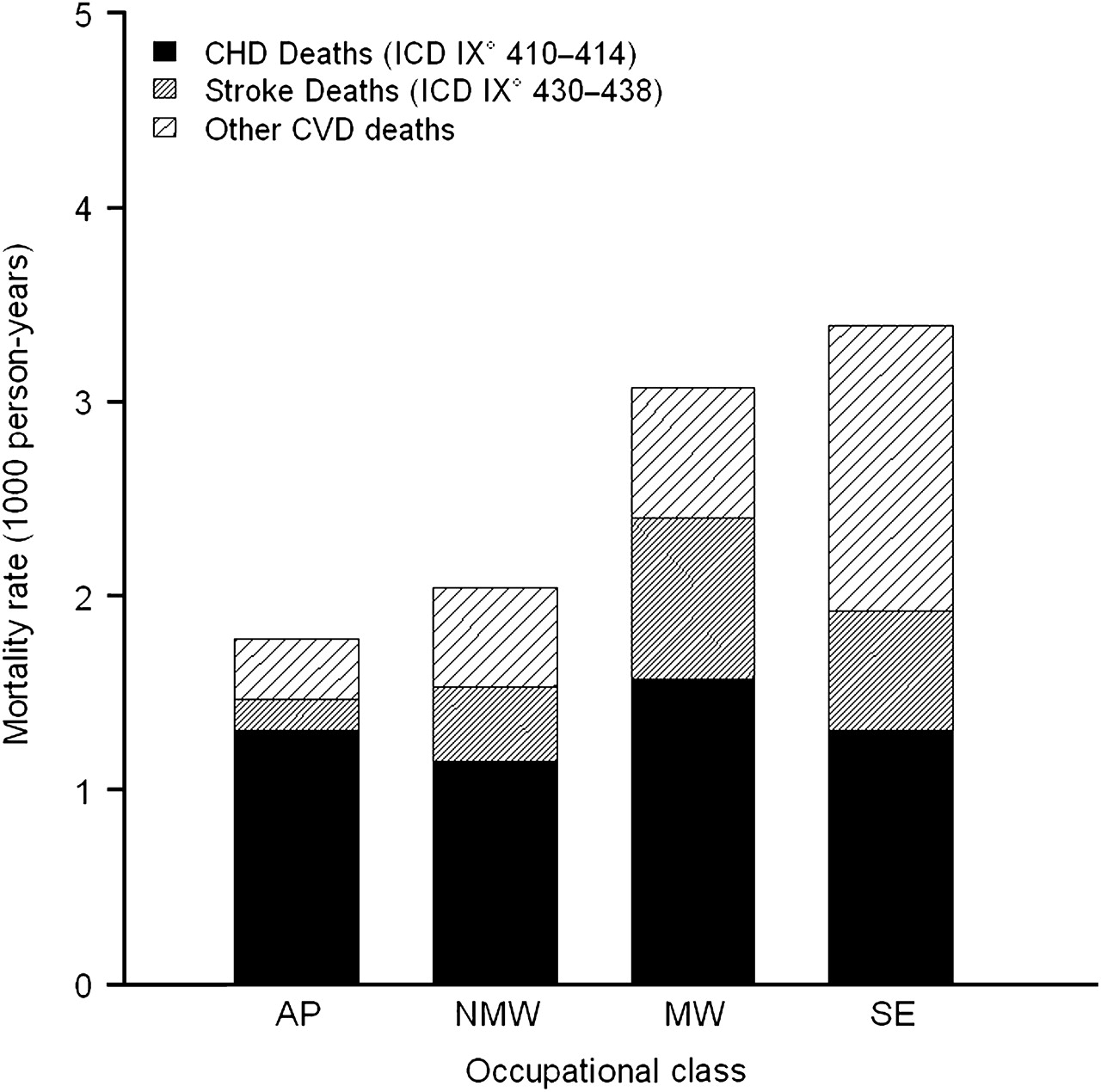
Figure 1 reports age-adjusted cardiovascular death rates according to codes reported on death certificates, in the whole sample (including subjects with a positive history of CHD at baseline) and by occupational group. No statistically significant differences were observed between occupational classes for CVD and CHD death rates, either when the χ2 test for trend or χ2 test for heterogeneity was considered.

Age-adjusted cardiovascular death (CVD) mortality rates (per 1000 person-years), partitioned into coronary heart disease (CHD), stroke and other CVD deaths, in the four occupational classes. AP, administrators and professionals; MW, manual workers; NMW, non-manual workers; SE, the self-employed.
Age-adjusted means and proportions of cardiovascular risk factors by occupational classes are reported in table 1. Statistically significant differences between occupational classes were observed for all investigated risk factors except total cholesterol and diabetes. Only systolic blood pressure mean values showed a clear increasing gradient from professionals and administrators to manual workers and the self-employed. Lower HDL-cholesterol means were found for the professional and administrator group. Higher prevalences of cigarette smokers and heavy alcohol drinkers were found in manual workers and the self-employed. Mean levels of the sport physical activity index were lower and the job strain ratio higher among manual workers in comparison to professionals and administrators and non-manual workers. The self-employed group had lower values for both the sport activity index and the job strain ratio. Systolic blood pressure, total cholesterol, HDL-cholesterol, current cigarette smoking, diabetes mellitus and alcohol intake were included in Cox models for multivariable adjustment. The above reported differences in CVD risk factors between occupational classes were confirmed in the sub-sample of currently employed subjects. In addition, the sport index showed a negative association with CHD incidence rate (age-adjusted HR=0.64) and the PJD/DL ratio showed a positive association (HR=1.4).
Age-adjusted mean or prevalence of major CHD risk factors at baseline, by occupational class (N=2964 subjects CHD-free at baseline)
Table 2 shows occupational group-specific age-adjusted and multivariable-adjusted CHD incidence rates and HRs. Compared to non-manual workers, administrators and professionals had the highest age-adjusted rate and HR, followed by the self-employed and manual workers. The estimated age-adjusted excess risks for administrators and professionals, the self-employed and manual workers were 84% (p=0.02), 72% (p=0.04) and 63% (p=0.04), respectively, with p=0.097 for the heterogeneity χ2 test of the overall association. Adjustment for systolic blood pressure, total and HDL-cholesterol, cigarette smoking, diabetes and alcohol intake reduced the HR of manual and self-employed workers, but the excess in risk remained statistically significant for the administrator and professional class.
Age-adjusted event rates and age- and multiple risk factors-adjusted HRs with 95% CI, of first CHD event, by occupational class (N=2964 subjects CHD-free at baseline)
As shown in figure 2, the excess risk of administrator and professional, self-employed and manual workers was mainly due to non-fatal CHD events, and the contribution of the validated CHD death rates was minimal.

{kind=link}
{kind=link}
Age-adjusted coronary heart disease (CHD) incidence rates (per 1000 person-years), partitioned into different event types: CHD deaths, definite non-fatal (NF) myocardial infarction (MI), possible myocardial infarction and coronary revascularisation, in the four occupational classes. AP, administrators and professionals; MW, manual workers; NMW, non-manual workers; SE, the self-employed.
In an additional age-stratified analysis to further control for the relatively younger age of the reference group, among those aged 55 years or less we found higher HRs for professionals and administrators (2.0; 95% CI 0.9 to 4.8), manual workers (2.4; 1.2 to 4.9) and the self-employed (2.4; 1.0 to 4.9). The HRs in the older age group (aged 55 or more) were reduced and not statistically significant.
In the sub-sample of currently employed subjects with data on sport physical activity and job strain (table 3), the number of CHD events was substantially smaller, with a wider 95% CI, but the pattern of the relationship between occupational classes and the incidence of CHD was similar, with higher rates and HR among administrator and professional, self-employed and manual workers. When adjustment for coronary risk factors also included the sport physical activity index, this reduced the HRs only in the manual worker class (−57.8%). When the PJD/DL ratio was further added to the model, the estimate of reduction in excess risk attributable to major CHD risk factors and job strain among manual worker was 71.4%, but again no changes occurred in the excess risks found among professionals and administrators and self-employed workers.
HRs of first CHD event, by occupational class
Discussion
In this northern Italian, population-based, prospective pooled-cohort study, CHD incidence rates in ever-working men were higher among administrator and professional, self-employed and manual workers in comparison to non-manual workers, with excess risks of 84%, 72% and 63%, respectively. This pattern was consistent across different CHD diagnostic categories, but was less evident when only fatal events were considered, a finding similar to those of other Italian studies.22 23 Thus our results confirm the CHD risk excess among manual workers reported by other studies, but we also found increased risks among administrators and professionals and the self-employed.
Among other prospective cohort studies assessing the association between occupational class and CHD incidence in men, two12 14 contrasted only manual and non-manual workers, and observed an excess risk of CHD of about 40% for manual workers. Such an approach with only two aggregated occupational classes is perhaps designed to identify large social strata to address specific population-based prevention strategies. That the observed excess risk was strongly attenuated after controlling for major CHD risk factors led the authors to conclude that there is no real need to consider social strata in primary preventive strategies.
On the other hand, Chandola,13 adopting a larger number of occupational classes in a British population-based sample, found a much higher RR (RR=2.16 and 2.15) in the incidence of CHD for skilled and semiskilled/unskilled manual workers when compared to service class higher. In comparison to the same reference group, many EGP categories had higher relative risks: foremen and technicians (2.00), farmers and smallholders (1.98), self-employed workers in industry (1.61), routine non-manual higher workers (1.60) and service class lower workers (1.71). In Chandola's study, as also observed by others,14 16 only a small amount of the excess risk was explained by known risk factors. Our findings were the same and are consistent with the distributions of CVD risk factors among the occupational classes. In fact, unskilled and skilled manual workers and the self-employed showed higher mean values of systolic blood pressure and higher prevalences of cigarette smokers, diabetes mellitus and heavy alcohol drinkers; higher administrators and professionals had higher mean levels of total cholesterol, lower mean levels of HDL-cholesterol, and lower administrators and professionals had a higher prevalence of diabetes.
In our sub-sample of currently employed subjects, when job strain and sport physical activity were added to the multivariate model, we observed a 71.4% reduction in the excess risk for manual workers, but no change in the excess risk for administrators and professionals and the self-employed. The reduction in risk in manual workers is consistent with the results reported by Marmot,18 in which the major contribution to job strain was job control. Andersen et al19 analysed data from three cohorts of both genders in Denmark, using a job-exposure matrix to estimate psychosocial work exposures. They found that only skill discretion was an independent explanatory variable of the occupational differences in CHD risk. Huisman et al20 investigated a large population-based Dutch sample of men and women, and reported a higher risk of hospitalisation for myocardial infarction in manual workers when compared to non-manual workers, but no excess risk in the small group of self-employed workers. The excess risk among manual workers was reduced substantially when job control was introduced into the model, but did not change when smoking habits and alcohol consumption were taken into account. Thus it seems that analysis of a wide range of occupational classes is essential to explore the effects of work environment and work organisation on health outcome, and also that in different socio-cultural contexts different components of job strain may explain the differences across occupational categories.
The results of our study, which was carried out on population-based samples representing a large variety of working conditions, including self-employed workers (artisans mainly involved in wood manufacture and service activities), indicated that the job strain model substantially explained the excess risk in manual workers only, but explained little of the excess risk in administrators, professionals and the self-employed.
The job strain model, developed in the 1970s,27 is still suitable for describing the work stress conditions of manual workers. However, it is likely that in its present form the JCQ fails to detect the strain conditions of administrators, managers and the self-employed, since their decision latitude is mainly determined by the constraints of rapidly changing markets and the more frequent financial crises; skill discretion is challenged by new and more complex technologies, and psychological demand is determined by self-made imposed pressures in an increasingly competitive worldwide market.
Huisman et al20 identified a dichotomised educational attainment score as an independent and strong predictor of CHD. In our study educational classes were derived from age-specific years of schooling in order to avoid spurious associations with CHD due to poor control for age.36 Our educational index was not an independent predictor of CHD incidence, nor was the interaction with occupational classes statistically significant. Educational classes may be of some importance when addressing prevention strategies in different social strata, but contribute poorly to the investigation of additional risk factors.
The major limitation of our study is that it was based on men only. We could not pursue a separate analysis for women because of the small number of CHD events among ever-working women (n=10). We did not perform a combined analysis of men and women together as this may have led to bias due to the higher frequency of CHD events among women in lower occupational and educational classes, which reduces the CHD social differences.
Another limitation of our study is that we used a subject's last job position to classify occupational class for a retired or unemployed man at baseline. However, Sundquist15 showed that occupation at retirement is an important predictor of CHD also for elderly subjects (≥65 years old). Moreover, restricting the analysis to currently employed subjects did not change our overall findings.
Finally, as in most other studies, we did not have information that allowed for control for changes over time in subject occupation, risk factors and job strain levels. One study that considered occupation at baseline and 20 years later reported a smaller increase in HR estimate after correction for changes in occupation.14
In conclusion, our study did not find a monotonic gradient in CHD incidence across occupational classes, but higher CHD rates were observed among manual workers as well as among administrators and professionals and the self-employed. The JCQ model needs further refinement so it can detect the specific work stressors and health consequences of business managers, entrepreneurs, professionals, owners of small business and artisans, occupations that are increasing in prevalence in post-industrialised societies.
Acknowledgments
The authors thank Mrs Lauretta Bolognesi and Dr Maria Teresa Gussoni for their accurate data collection and diagnostic validation of coronary heart disease events.
References
Footnotes
Funding The MONICA Brianza Study was mainly supported by the health administration of the Lombardy Region. The follow-up was partially supported by grants from the Italian Ministry of Health and was carried out in collaboration with the Centro di Epidemiologia, Sorveglianza e Promozione della Salute of the Istituto Superiore di Sanità, Rome.
Competing interests None.
Ethics approval This study was conducted with the approval of the Ethic Committee of the University Hospital of Monza.
Provenance and peer review Not commissioned; externally peer reviewed.