Article Text

Abstract
Objectives: To investigate the use of multiple health data sources for population-based asbestosis surveillance in British Columbia, Canada.
Methods: Provincial health insurance registration records, workers’ compensation records, hospitalisation records, and outpatient medical service records were linked using individual-specific study identifiers. The study population was restricted to individuals ⩾15 years of age living in the province during 1992–2004.
Results: 1170 new asbestosis cases were identified from 1992 to 2004 for an overall incidence rate of 2.82 (men: 5.48, women: 0.23) per 100 000 population; 96% of cases were male and average (SD) age was 69 (10) years. Although the annual number of new cases increased by 30% during the surveillance period (β = 2.36, p = 0.019), the observed increase in annual incidence rates was not significant (β = 0.02, p = 0.398). Workers’ compensation, hospitalisation and outpatient databases identified 23%, 48% and 50% of the total new cases, respectively. Of the new cases, 82% were identified through single data sources, 10% were only recorded in the workers’ compensation records, and 36% only in each of the hospitalisation and outpatient records. 84% of hospitalisation cases and 83% of outpatient cases were not included in the workers’ compensation records. The three data sources showed different temporal trends in the annual number of new cases and annual incidence rates.
Conclusions: Single data sources were not sufficient to identify all new cases, thus leading to serious underestimations of the true burden of asbestosis. Integrating multiple health data sources could provide a more complete picture in population-based surveillance of asbestosis and other occupational diseases.
Statistics from Altmetric.com
Asbestos exposure is one of the most important occupational health issues worldwide.1 2 It is estimated that currently about 125 million people are exposed to asbestos at the workplace and that at least 90 000 people die from asbestos-related diseases each year.3 Even in countries that have banned or restricted the use of asbestos, the burden of asbestos-related disease is still rising. In the United States during the period 1968–2000, the number of asbestosis deaths increased 20 times from 77 deaths in 1968 to 1493 deaths in 2000 (the annual mortality rate increased from 0.54 to 6.88 per million population).4 In contrast, the mortality rates of silicosis, coal workers’ pneumoconiosis (CWP) and other pneumoconioses steadily declined during the same period. There is a similar temporal trend in Australia: asbestosis mortality rates increased threefold from 1979 to 2002, whereas mortality rates for silicosis and CWP declined substantially during the same period.5 In 2003, the International Labour Organization and the World Health Organization urged that special attention should be paid to the elimination of asbestos-related diseases.2
What this paper adds
Asbestosis surveillance has generally relied on death certificates or workers’ compensation records.
Mortality data may not accurately reflect the incidence of asbestosis and workers’ compensation records may underestimate the true burden of the disease since some affected workers may not seek occupational compensation or some applications may not be accepted.
Single data sources were not sufficient to identify all new cases and thus led to serious underestimations of the true burden of asbestosis in the population.
Integrating multiple health data sources could provide a more complete picture in population-based surveillance of asbestosis and other occupational diseases.
Asbestosis, one of the most common asbestos-related diseases, is a progressive fibrotic lung disease caused by the inhalation of asbestos fibres primarily from contaminated air at the workplace. The fibrotic lung tissues lose their elasticity and thus cannot expand and contract normally, causing the most common symptom of asbestosis, shortness of breath on exertion.6 Although asbestosis is non-malignant, it is associated with an increased risk of lung cancer, especially among smokers.6 7 The severity of the disease depends upon the duration and intensity of exposure as well as possible individual susceptibility.8 9 Asbestosis has a long latency period and may not clinically manifest for several years or even decades after primary exposure.6 10 There is no effective treatment available, and therefore primary prevention of exposure to asbestos is essential.6
Asbestosis surveillance has generally relied on death certificates or workers’ compensation records.4 5 11 However, mortality data may not accurately reflect the incidence of the disease and workers’ compensation records may underestimate the true burden of the disease since a large proportion of affected workers may not seek occupational compensation.12 13 14 Some studies have suggested that hospitalisation data sources are important in asbestosis and other pneumoconioses surveillance.15 16 17 18 19 However, Rosenman and colleagues showed that hospitalisation records cannot identify all asbestosis cases15 because some patients in the early stages of the disease are less likely to be hospitalised and included in this data source. The use of readily available health data sources to collect accurate information about asbestosis and other occupational diseases remains an important research area that deserves further investigation.
In this study, we used multiple health data sources including workers’ compensation records, hospitalisation records and outpatient records from British Columbia, Canada to: (1) identify new asbestosis cases and determine incidence rates and temporal trends from 1992 to 2004; (2) examine the characteristics of asbestosis cases by demography, industry and occupation; and (3) investigate the relationship between different data sources in identifying new asbestosis cases.
Methods
The detailed methods for the construction and use of the British Columbia Linked Health Database (BCLHD) as a research data resource have been described elsewhere.20 21 Briefly, the BCLHD is a large health data resource that contains multiple electronic administrative health data sources including provincial health insurance registration records, workers’ compensation records, hospital separation records and outpatient medical service records. All these data sources can be linked using anonymous individual-specific study identifiers.20 21 These data sources contain the International Classification of Disease (ICD) diagnosis codes. ICD-9 code 501 (asbestosis) and ICD-10 code J61 (pneumoconiosis due to asbestos and other mineral fibres) were used to identify asbestosis cases.
Data sources
The Medical Services Plan (MSP) of British Columbia managed by the Ministry of Health Services provides universal health care insurance for the residents of the province.22 During the 2004/2005 fiscal year, 4.25 million (over 95%) residents were registered with MSP.23 The population of this study was enumerated from the residents registered with the plan from 1992 to 2004. The registration records provided socio-demographic data including date of birth, sex and health service delivery area.
Workers’ compensation data from the provincial workers’ compensation system included all accepted short-term (at least 1 day of time loss) disability, long-term (permanent impairment) disability or fatal compensation claims in the province from 1992 to 2004. The compensation records provided registration date, claim number, medical diagnosis (ICD-9), and worker’s occupation and industry information.
Hospital separation data included all hospitalisation records for inpatients (at least one overnight hospital stay) in British Columbia hospitals from 1992 to 2004. This data source provided hospital code, admission date, length of stay, separation date, up to 16 diagnoses (ICD-9 before 2001) or 25 diagnoses (ICD-10 since 2001) to describe the reasons for hospitalisation.
Outpatient medical service data included all outpatient medical service records provided by general practitioners, specialists and supplementary health care practitioners for patients with the health insurance plan from 1992 to 2004.22 Records with the specialty services unrelated to asbestosis such as physiotherapy, ophthalmology and orthopaedic surgery were excluded. This data source provided service date, practitioner number, specialty code, service code and one diagnosis code (ICD-9) for each outpatient visit.
Case definitions
Workers’ compensation case: one accepted short-term (at least 1 day of time loss) disability, long-term (permanent impairment) disability, or fatal compensation claim for asbestosis.
Hospitalisation case: one hospitalisation record with the diagnosis of asbestosis.
Outpatient case: two outpatient visits with the diagnosis of asbestosis.
To identify new asbestosis cases, individuals who had a compensation record or a hospitalisation record with the diagnosis of asbestosis before 1992 (based on available data back to 1985) were excluded from the study. For asbestosis cases with multiple records in different data sources, the record with the earliest date was selected as the incident case in the overall analysis.
Statistical analysis
The study population was restricted to adults aged 15 years and older who resided in British Columbia during the surveillance period from 1992 to 2004, as indicated by the provincial health insurance registry. The annual incidence rate was calculated as the annual number of new asbestosis cases divided by the annual number of adults living in the province. The period incidence rate was calculated as the total number of new asbestosis cases divided by the total number of adults living in the province during the surveillance period. Linear regression analysis was used to examine the temporal trends of the annual number of new cases and the annual incidence rates. A p value of less than 0.05 was considered to be statistically significant. All analyses were performed using SAS 9.1 software (SAS Institute, Cary, North Carolina, USA).
Results
At baseline in 1992, there were 2.77 (1.37 men, 1.40 women) million adult residents aged 15 years and older in British Columbia. From 1992 to 2004, the annual number of adult residents increased by 26% to about 3.50 (1.72 men, 1.78 women) million.
From 1992 to 2004, a total of 1170 new asbestosis cases (1121 men, 49 women) were identified using workers’ compensation records (n = 271), hospitalisation records (n = 562) and outpatient records (n = 582). The overall incidence rate was 2.82 (5.48 for men, 0.23 for women) per 100 000 population during the surveillance period. By single data sources, the incidence rate was 0.65, 1.36 and 1.40 per 100 000 population for workers’ compensation, hospitalisation and outpatient data sources, respectively.
The majority (96%) of new cases were male. The proportion of men was higher among workers’ compensation and hospitalisation cases compared to that among outpatient cases. The average (SD) age was 69 (10) years (69 for men, 68 for women) and approximately 80% of new cases were over 60 years of age. On average, hospitalisation cases were older than workers’ compensation cases and outpatient cases (table 1).
Characteristics of new asbestosis cases identified from three data sources in British Columbia, 1992–2004
Temporal trends and incidence rates
Overall, the annual number of new cases increased by 30% during the surveillance period (β = 2.36, p = 0.019). Single data sources showed different temporal trends. For workers’ compensation cases, the annual number of new cases tended to decline, but the trend was not significant (β = −0.46, p = 0.254). For outpatient cases, there was a significant increase in the annual number of new cases (β = 2.21, p = 0.002) (fig 1). The observed increase was not significant for hospitalisation cases (β = 1.17, p = 0.053).
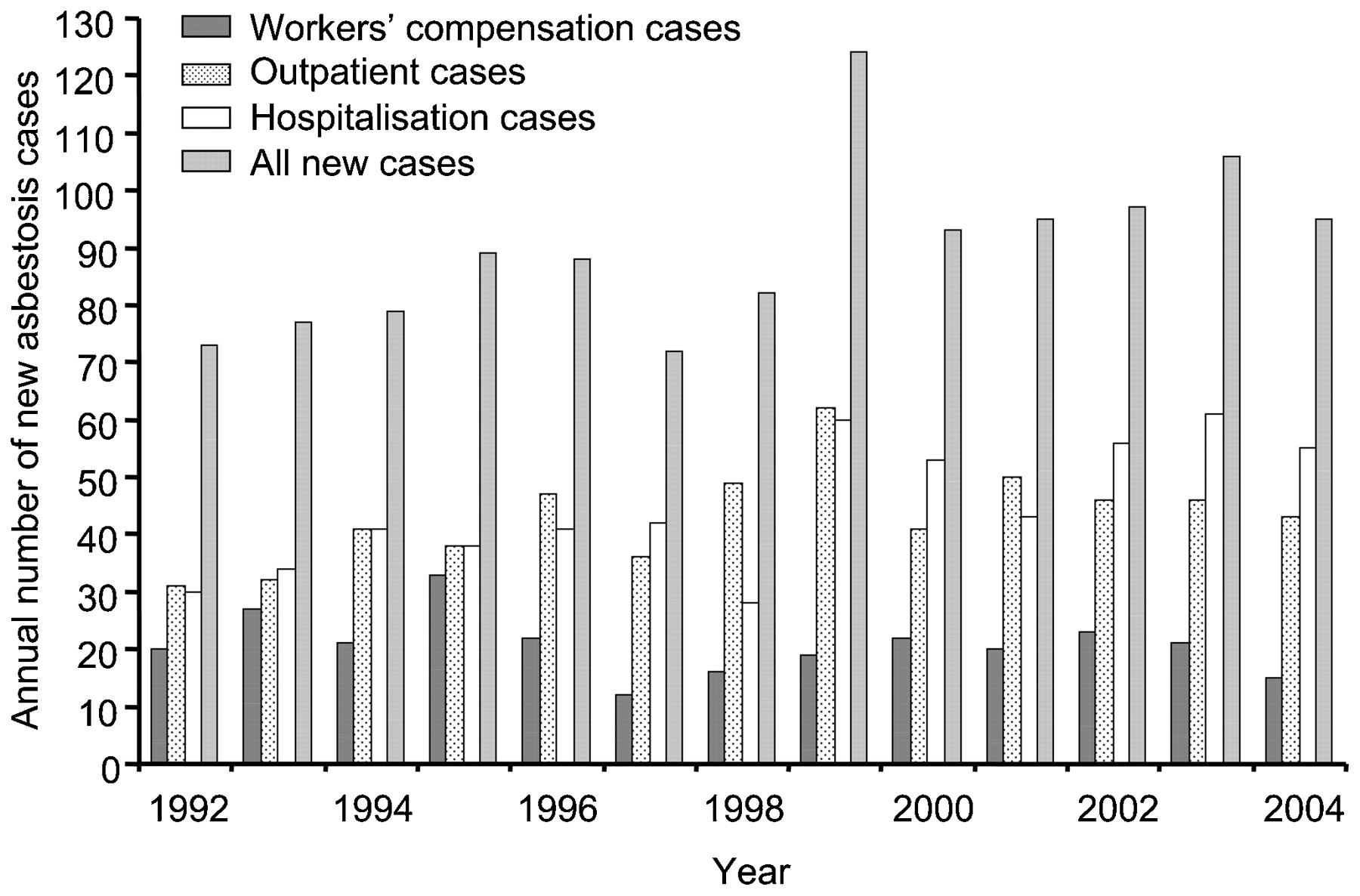
Annual number of new asbestosis cases from different data sources in British Columbia, 1992–2004. For cases with multiple records in different data sources, the record with the earliest date was selected in the category of all new cases.
Overall, there was a small increase in the annual incidence rate of asbestosis during the surveillance period, but the increase was not significant (β = 0.02, p = 0.398). By data sources, there was a decline in the annual incidence rate for workers’ compensation data (β = −0.03, p = 0.055), an increase for outpatient data (β = 0.04, p = 0.025) and a non-significant increase for hospitalisation data (β = 0.01, p = 0.414) (fig 2).

Annual incidence rates of asbestosis for adults aged ⩾15 years in British Columbia, 1992–2004.
Multivariate linear regression analysis including the cases from the three data sources showed that at baseline (1992) there were more outpatient cases (β = 5.23, p = 0.355) and hospitalisation cases (β = 11.00, p = 0.057) compared to workers’ compensation cases, but the differences did not reach statistical significance. However, there was a significant increase in the annual number of outpatient cases (β = 2.67, p = 0.001) and hospitalisation cases (β = 1.63, p = 0.027) compared to the annual number of workers’ compensation cases during the surveillance period.
Industries and occupations
Industry and occupation information was only available in the workers’ compensation data source. The most frequently recorded industries were construction and renovation; ship building and repair; pulp and paper mill; and plumbing, heating, ventilation installation and repair. The most frequently recorded occupations were carpenters, plumbers, electricians, welders, insulation workers and asbestos workers (table 2).
Most frequently recorded industries and occupations in the workers’ compensation data source in British Columbia, 1992–2004
Capability of different data sources in identifying new asbestosis cases
A Venn diagram of asbestosis cases by data sources shows that the workers’ compensation data identified only 23% of total new cases; the hospitalisation data and outpatient data identified 48% and 50% of total new cases, respectively (fig 3). Most new cases (82%) were identified through single data sources; 10% of new cases were only recorded in the workers’ compensation data source, and 36% only in each of the hospitalisation and outpatient data sources (fig 3).

{kind=link}
{kind=link}
{kind=link}
Relationship between workers’ compensation (n = 271), hospitalisation (n = 562) and outpatient (n = 582) data sources in identifying new asbestosis cases (n = 1170) in British Columbia, 1992–2004.
Both outpatient and hospitalisation databases included a field to identify if a third party was responsible for the medical expenses. A total of 39 cases (7%) identified through the outpatient data source and 21 cases (4%) identified through the hospitalisation data source were flagged as the responsibility of the workers’ compensation system but did not appear in the workers’ compensation data source. These cases might represent health care only compensation claims that had not yet progressed to a work disability claim as captured in the workers’ compensation data source.
Discussion
Asbestos exposure in British Columbia has been, in most ways, typical of the experience in Canada and other Western industrialised nations where asbestos was used extensively for insulation and in cement until restrictions on its use starting in the early 1970s. Asbestos had also been used in construction and other industries.24 The province was once the home of a large ship building industry with 25 000 workers during the Second World War.25 In addition, until the early 1990s there was a chrysotile asbestos mine in the northern part of the province.26 During our surveillance period from 1992 to 2004, the most frequently recorded industries and occupations in the workers’ compensation data source (table 2) were consistent with those reported in other countries.27 28 29
Exposure to asbestos fibres may cause multiple respiratory diseases including asbestosis, pleural plaque, lung cancer and mesothelioma.30 Among these diseases, mesothelioma can be readily captured by cancer reporting systems and is often used to represent asbestos-related diseases in population-based disease surveillance. There is little information about population-based asbestosis incidence levels and temporal trends. In this unique study, we sought to integrate workers’ compensation records, hospitalisation records and outpatient medical service records to undertake population-based asbestosis surveillance in British Columbia.
From 1992 to 2004, the annual number of new asbestosis cases increased by 30%, but the observed increase in the annual incidence rates was not significant. While these cases are largely due to exposure to asbestos fibres several decades ago,6 10 a total of 1170 new cases represents a heavy social and economic burden for these workers and their families as well as for the health care system and the workers’ compensation system in British Columbia.
Single data sources showed different temporal trends in the annual number of new cases and annual incidence rates. Workers’ compensation data showed that these two measures tended to decline from 1992 to 2004, whereas outpatient data showed that these two measures significantly increased during the same period. These three data sources might reflect different aspects of the disease. The outpatient data source was more likely to capture younger cases in the early stages of disease, whereas the hospitalisation data source was more likely to capture older cases in the later stages of disease. The workers’ compensation data source captured the cases who sought occupational compensation and could prove historical work exposure. This study demonstrated that each single data source played an important role in identifying new asbestosis cases, but each single data source was not sufficient to identify all new cases. Relying on only one data source such as the workers’ compensation records would lead to serious underestimations of the true burden of asbestosis in the population. Integrating the three data sources will provide a more complete picture in population-based asbestosis surveillance.15 18
It is striking that 84% of the hospitalisation cases and 83% of the outpatient cases were not present in the workers’ compensation data source (fig 3). One possible reason is that some affected workers did not seek occupational compensation due to a lack of awareness of historical work exposure or a lack of knowledge about the workers’ compensation procedure (health care providers might not inform the cases that the disease was compensable), especially once they had retired from the workforce. In addition, among those still in the workforce job insecurity and discouragement from supervisors and coworkers are also possible reasons for not seeking occupational compensation. Secondly, because of the long latency between primary exposure and clinical manifestation, some affected workers might be not able to prove historical work exposure. Therefore they might be less likely to seek compensation or their applications might not be accepted.12 13 31 In our study, the fact that about 80% of these cases were over 60 years of age may lend some support to this possibility. Thirdly, the workers’ compensation data source was limited to accepted short-term (at least 1 day of time loss) disability, long-term (permanent impairment) disability or fatal compensation claims. Health care only compensation claims were not included in this data source. We observed that about 7% of the outpatient cases and 4% of the hospitalisation cases were flagged as the responsibility of the workers’ compensation system but did not appear in the workers’ compensation data source during the surveillance period. Finally, British Columbia is the preferred retirement destination in Canada, and about 75% of the retired residents were not born in the province.32 Affected workers who were exposed to asbestos in other provinces and even in other countries might not be recorded in the provincial workers’ compensation system. We had no data to assess the impact of these retirees on the study findings.
In Canada, provincial workers’ compensation systems are insurance providers for workers who contract occupational diseases. The coverage percentages for workforces vary from 70% to 100% across different provinces and territories. In British Columbia, WorkSafeBC is the only institute responsible for workers’ compensation under the Workers Compensation Act. In theory, for those who contracted asbestosis in British Columbia, the medical expenses should be paid by WorkSafeBC, whereas for those who contracted the disease in other provinces, including retirees from other provinces, the medical expenses should be paid by the respective workers’ compensation systems in the other provinces. Apparently, the prerequisite condition is that these affected workers have to first make a successful compensation claim from their respective workers’ compensation systems. Otherwise, their medical expenses will be paid by the MSP in British Columbia; as a universal health insurance plan for the residents in the province, there are no restrictions on disease history, occupational history or residential history. Although it is unclear in practice how the medical expenses are paid for asbestosis therapy, this study indicates the cost-shift from workers’ compensation systems to the provincial health insurance system may be a serious problem that deserves further investigation.
The Venn diagram (fig 3) shows that 44% (n = 118) of the workers’ compensation cases and 74% (n = 418) of the hospitalisation cases were not included in the outpatient data source (fig 3). Two reasons may partly explain this discrepancy. Firstly, we used a stringent case definition of at least two outpatient visits with the diagnosis of asbestosis to reduce possible misdiagnosis for outpatient cases. A total of 21 of the 118 workers’ compensation cases and 41 of the 418 hospitalisation cases had only one outpatient visit with the diagnosis of asbestosis and thus were excluded from the outpatient cases. Secondly, the outpatient data were collected for administrative billing purposes. For each outpatient service, only one diagnosis can be recorded in the database. In clinical settings, asbestosis may coexist with other chronic diseases such as chronic obstructive pulmonary disease (COPD), pneumonia, diabetes, asthma and cardiovascular disease. As these coexistent chronic diseases may be more likely to be recorded for billing purposes, asbestosis information may thus be missed from this data source. This situation also demonstrates that the outpatient data source itself is not sufficient to identify all asbestosis cases.
Although there is no consensus concerning individual susceptibility to asbestosis, the notion is plausible since not all workers or laboratory animals exposed to common sources of asbestos eventually develop the disease, indicating that individual susceptibility may play a role in the development of occupational asbestosis.8 9 Several studies have provided convincing evidence on individual variation in asbestosis susceptibility. A cross-sectional study with 658 carpenters occupationally exposed to asbestos found that workers deficient in glutathione S-transferase mu (GSTM1) gene were more likely to develop asbestosis than those who were not deficient.33 Another similar study with 145 asbestos insulators exposed to high levels of asbestos found that workers with N-acetyltransferase 2 (NAT2) slow-acetylator genotype were 2.3 times more likely to develop both malignant (mesothelioma) and non-malignant (asbestosis and/or pleural plaques) pulmonary diseases compared to those with NAT2 fast-acetylator genotype. Workers with both GSTM1 null genotype and NAT2 slow-acetylator genotype were 5.1 times more likely to develop malignant and non-malignant pulmonary diseases and 4.1 times more likely to develop non-malignant pulmonary diseases compared to those who had the GSTM1 gene and a NAT2 fast-acetylator genotype.34 Individual anatomical characteristics are also associated with individual susceptibility to asbestosis. Becklake and colleagues reported that compared to equally exposed controls, asbestosis cases were shorter in height and had smaller intrathoracic tracheal lengths and narrower transthoracic diameters.35 In an interesting experimental study, Bégin and colleagues found that after 2 years of exposure to equal doses of chrysotile fibres, 10 out of 15 sheep developed asbestosis. The sheep with asbestosis retained more fibres in bronchoalveolar lavage and lung tissue than those who did not develop asbestosis.36 The excess retention of asbestos fibres preceded the appearance of asbestosis.37 The above evidence demonstrates that there may be individual susceptibility to asbestosis.
This study has some limitations. Firstly, the outpatient and hospitalisation data were collected for administrative billing rather than research purposes. As mentioned above, for each outpatient visit, only one diagnosis was recorded in the database and so asbestosis information might be missed from this data source.
Secondly, it was possible that some asbestosis cases might have come from other provinces or countries in which causative exposure to asbestos occurred. However, on the other hand, it was also possible that some cases originating in British Columbia might have emigrated to other provinces or countries. In addition, some cases may have died of asbestosis prematurely and thus would not have been recorded by these data sources. The former situation might cause the severity of asbestosis in British Columbia to be overestimated, whereas the latter situations might cause it to be underestimated. No data are available to evaluate the impact of these uncertainties.
Thirdly, clinical misdiagnosis of asbestosis was possible for the outpatient and hospitalisation cases. In outpatient clinical settings, people might consult physicians for many reasons such as previous asbestos exposure, screening for asbestos-related disease, and evaluation for specific symptoms or impairment. Even though the final diagnosis might exclude the possibility of asbestosis, a temporary diagnosis of asbestosis might have been entered for billing purposes before the final results were available. Moreover, since the 1980s the use of asbestos has been banned or restricted in Canada, intensive exposure to asbestos is uncommon and severe forms of asbestosis are rarely observed.6 38 It was more difficult to distinguish asbestosis from other interstitial lung diseases by clinical, physiological and radiological findings. Misdiagnosis was thereby possible for the outpatient cases and hospitalisation cases.8 39 Nevertheless, as we used a stringent case definition for outpatient cases, misdiagnosis should not be a serious issue for outpatient cases.
Finally, we were unable to contact cases or access their original medical records because of privacy concerns. As a result, we were unable to evaluate the quality of these data sources such as the consistency between the original medical records and the electronic records in our databases. Therefore, it was possible that some relevant diagnoses such as asbestos-related pleural plaques were mistakenly coded as asbestosis in the electronic databases.
Conclusions
This study found that the annual number of new asbestosis cases increased by 30% during the surveillance period from 1992 to 2004; the annual incidence rates tended to increase but the temporal trend was not significant. Although the new cases were largely due to exposure to asbestos fibres several decades ago, a total of 1170 new cases represents a heavy social and economic burden for British Columbia.
This study also demonstrated that each single data source played an important role in identifying new asbestosis cases, but that each single data source alone was not sufficient to identify all new cases, which could lead to serious underestimations of the true burden of asbestosis in the population. Integrating multiple health data sources including workers’ compensation records, hospitalisation records and outpatient medical service records could provide a more complete picture in population-based surveillance of asbestosis and other occupational diseases.
REFERENCES
Footnotes
Funding This research was funded by WorkSafeBC (the Workers’ Compensation Board of British Columbia) through the WorkSafeBC-CHSPR Research Partnership. MK was supported in part by a Michael Smith Foundation for Health Research Senior Scholar Award.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.