Article Text

Abstract
Objectives: To examine the efficacy of a participatory ergonomics intervention in preventing musculoskeletal disorders among kitchen workers. Participatory ergonomics is commonly recommended to reduce musculoskeletal disorders, but evidence for its effectiveness is sparse.
Methods: A cluster randomised controlled trial among the 504 workers of 119 kitchens in Finland was conducted during 2002–2005. Kitchens were randomised to an intervention (n = 59) and control (n = 60) group. The duration of the intervention that guided the workers to identify strenuous work tasks and to seek solutions for decreasing physical and mental workload, was 11 to 14 months. In total, 402 ergonomic changes were implemented. The main outcome measures were the occurrence of and trouble caused by musculoskeletal pain in seven anatomical sites, local fatigue after work, and sick leave due to musculoskeletal disorders. Individual level data were collected by a questionnaire at baseline and every 3 months during the intervention and 1-year follow-up period. All response rates exceeded 92%.
Results: No systematic differences in any outcome variable were found between the intervention and control groups during the intervention or during the 1-year follow-up.
Conclusions: The intervention did not reduce perceived physical work load and no evidence was found for the efficacy of the intervention in preventing musculoskeletal disorders among kitchen workers. It may be that a more comprehensive redesign of work organisation and processes is needed, taking more account of workers’ physical and mental resources.
Statistics from Altmetric.com
Musculoskeletal disorders continue to be a major cause of morbidity, work disability and productivity losses with considerable economic and societal consequences.1–3 Evidence has accumulated for the role of both physical and psychosocial factors at work in the aetiology of these disorders.4–8 Several theoretical models of causal pathways between aetiological factors and musculoskeletal disorders have been presented.8–10 This study was based on the model by Sauter & Swanson (1996).10 We hypothesised that optimisation of biomechanical and mental load would prevent the occurrence of musculoskeletal disorders.
Participatory ergonomics is a widely recommended approach to reduce musculoskeletal disorders.2 11–15 It has also been suggested as the most efficient way to improve ergonomics in the workplace.16 However, evidence for the effectiveness of ergonomic interventions is scanty. It is mostly derived from case studies, while controlled trials are sparse and most have severe methodological flaws.17–22
The study was targeted to kitchen work in which workers have a high prevalence of musculoskeletal disorders,23–26 and the work is physically demanding 24 25 27 often involving ergonomic problems.23 27 Little research has been conducted to study this occupational group.
Our aim was to examine, using a cluster randomised controlled trial, the efficacy of a participatory ergonomics intervention in preventing, in terms of both primary and secondary prevention, the occurrence of musculoskeletal disorders among kitchen workers. The main outcomes were musculoskeletal pain, trouble caused by such pain, local musculoskeletal fatigue after the work day, and sick leave.
MATERIALS AND METHODS
Study design
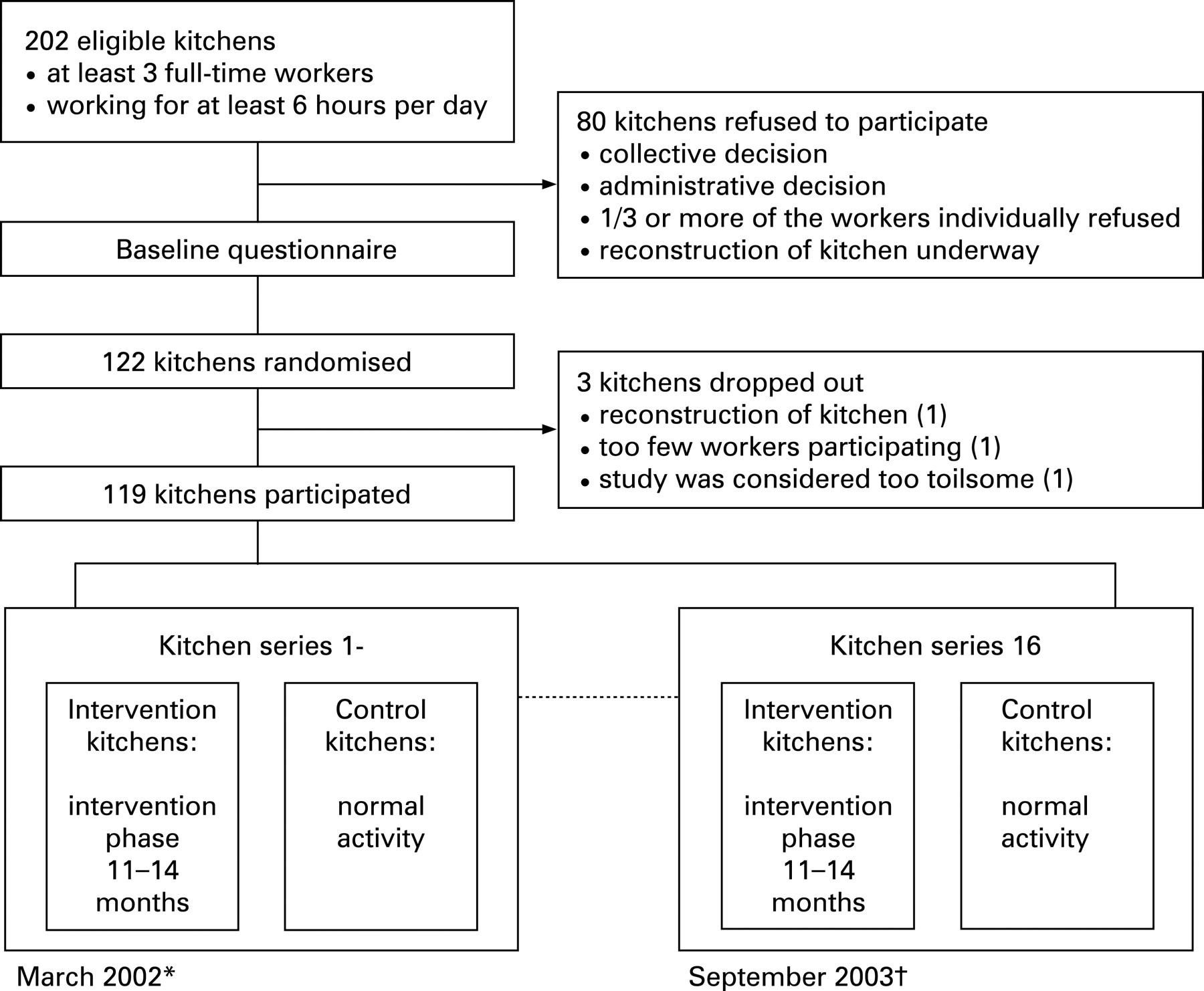
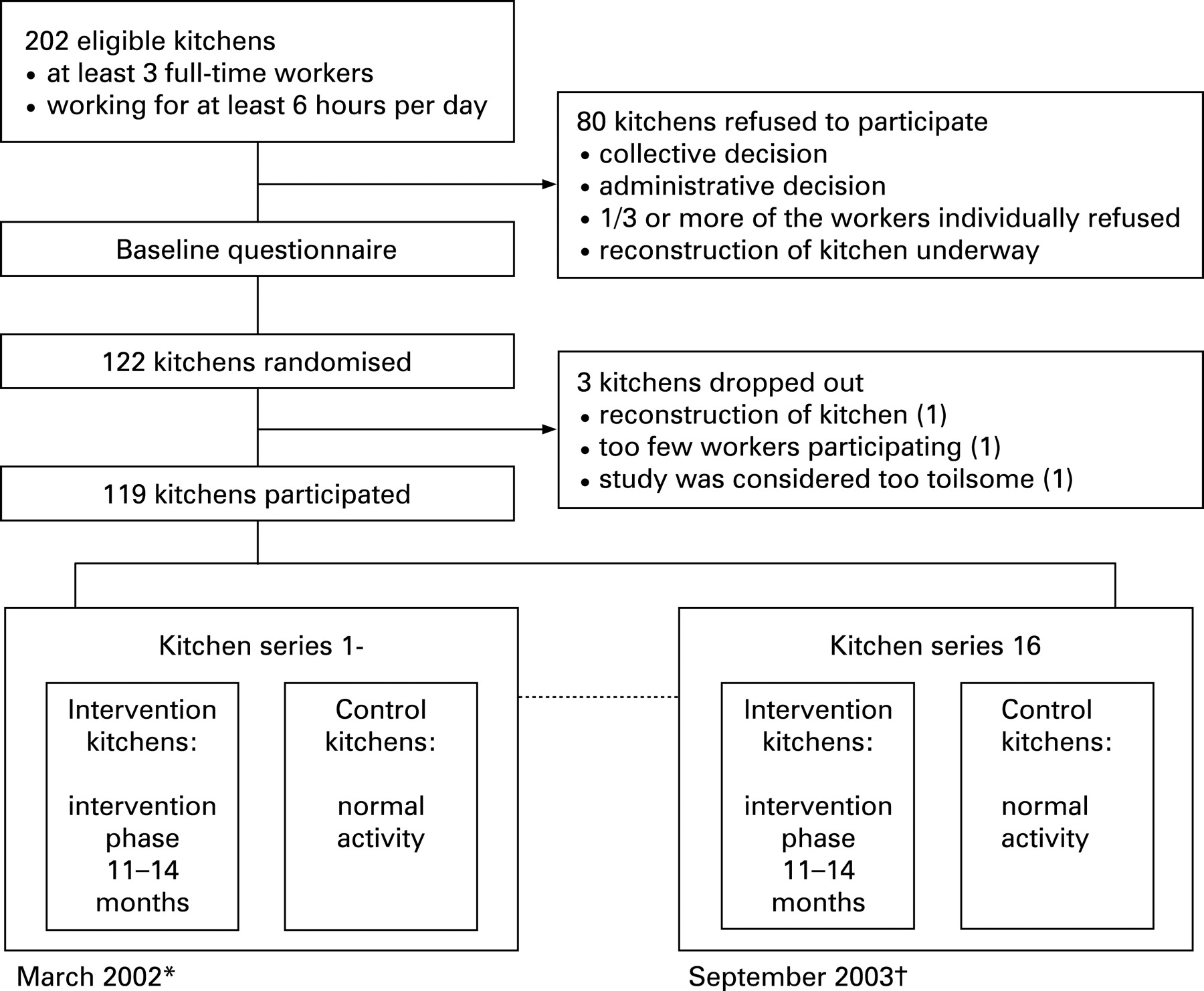
This is a report of a series on a cluster randomised controlled trial regarding the efficacy of a participatory ergonomics intervention in preventing musculoskeletal disorders. Altogether 119 municipal kitchens (60% of the eligible kitchens) in four large cities in Finland were randomised to an intervention (n = 59) and control (n = 60) group. The total number of workers was 504. Eligibility criteria for participation and causes of refusal are presented in fig 1. Written informed consent was obtained from each kitchen and each worker separately. The study started at the beginning of 2002, and by the end of 2004 the intervention phase was completed. The 1-year, post-intervention follow-up continued until the end of 2005.
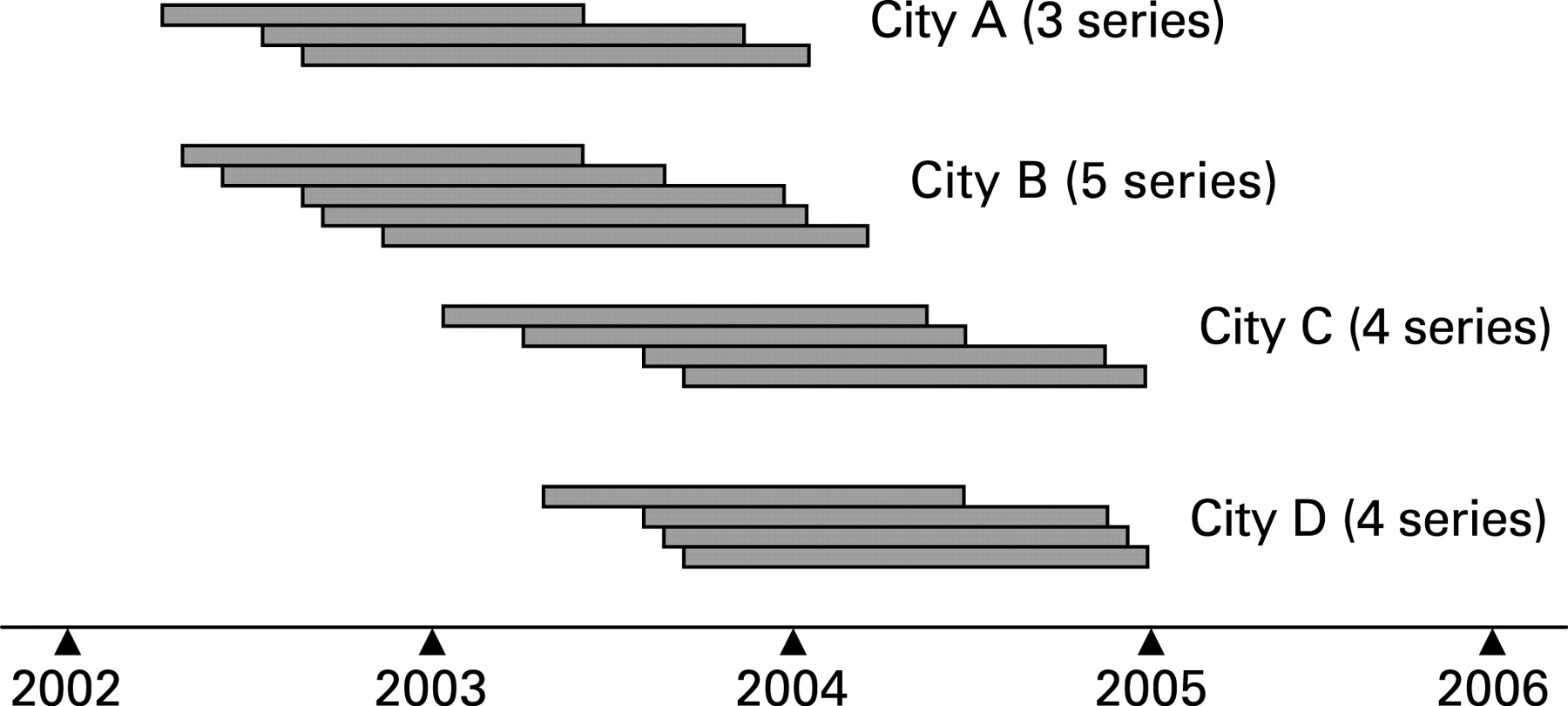
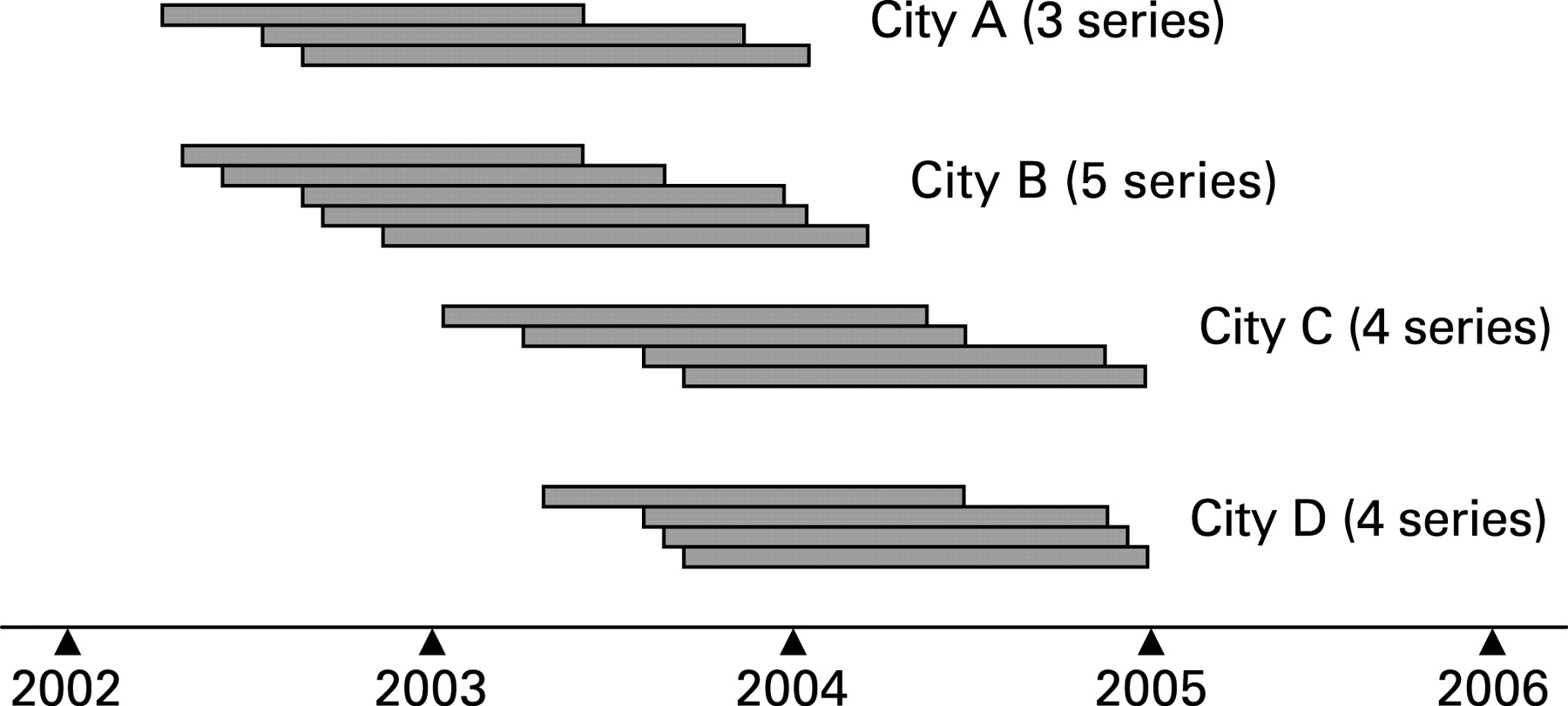
The study was carried out in a series of eight kitchens on average that entered sequentially in time (fig 2). The field study was executed by four teams of two researchers trained in ergonomics and in good practice in kitchen work.
Data collection
Baseline data on morbidity, employment history, and lifestyle were collected before randomisation (fig 1). Information on individual level outcome measures was gathered by a questionnaire every 3 months during both the intervention (I3, I6, I9, I12) and the 1-year, post-intervention follow-up (PI3, PI6, PI9, PI12). A researcher distributed the questionnaires to all participating kitchens. If a worker was on sick leave or vacation, the questionnaire was mailed to her/his home address or she/he was asked to complete it within 1 week of returning to work. Non-responders were reminded by telephone after 2 weeks. The response rates in different surveys varied between 92.0% and 98.5%.
In the control group, during the 3-monthly visits, the researcher distributed the follow-up questionnaires and documented all spontaneously occurred ergonomic changes based on short interviews. There were no other visits and no trainings by researchers at these kitchens.
Randomisation
Randomisation was carried out using an assignment algorithm28 (Alternate Ranks Design (ARD)) and stratification by area (city district) and type of kitchen (school, nursery, home for senior citizens, other institution). Kitchens in each stratum were ranked in descending order by number of staff. A person not otherwise involved in the study during the field phase performed the randomisation. Table 1 shows the baseline characteristics of the kitchens and study subjects.
Intervention
The framework of this participatory intervention was based on the model developed at the Finnish Institute of Occupational Health.29 Experienced researchers modified the final content and practical implementation strategy according to the current state of the art. The intervention was based on active group work. The workers were actors identifying problems, planning and evaluating changes, and implementing them in collaboration with management and technical staff. The researcher acted as a consultant and trainer, promoting, guiding, and training the workers during the development work and taking care of progress of the implementation of changes. The detailed contents of the intervention process and its evaluation are reported elsewhere.30
Pre-implementation phase (2 months)
In all series, the intervention kitchens’ personnel participated in two 1-day workshops (total 10 h). In the first workshop, the workers were taught basic principles of ergonomics and the functioning of the musculoskeletal system. They were trained and encouraged to analyse their work tasks and processes, to identify strenuous tasks and risk factors, and to seek solutions to decrease their physical and mental workload. The kitchens were then allowed 1 month to analyse their work and develop ideas to improve ergonomics. During this period, the researcher visited each kitchen once and made one phone call. In the second workshop, every kitchen decided on their primary targets to improve ergonomics and planned the implementation.
To ascertain the similarity of working methods between the researcher teams, the project coordinator supervised the workshops and gave feedback to the researchers. The foodservice management and technical staff were invited to participate in the workshops. Moreover, to enhance the exchange of information between foodservice management and the research group, a local steering group was established in two cities.
Implementation phase (9–12 months)
Ergonomic changes were implemented during a period of 9–12 months, promoted by six 3 h workshops (total 18 h) attended by all workers of intervention kitchens in a series. Each workshop had a specific thematic element related to ergonomics (working postures, manual materials handling, repetitive work, hurry, physical risk factors, and work safety), and the progress of the intervention was thoroughly discussed. The personnel of each kitchen kept a detailed diary about the ergonomic changes made. Within each series, the workshops rotated from one kitchen to another to give the workers an opportunity to learn from each other’s solutions and practices. The researcher conducted extra visits on request to give support to the kitchens. The ergonomic changes were targeted at physically strenuous work tasks, those that were repeated often, or which involved a risk of sudden overloading. The changes were implemented within the annual budgets of the kitchens. The municipal authorities agreed to prioritise the intervention kitchens in case of special needs during the intervention phase. Due to summer holidays at schools the implementation period varied between 9 and 12 months. One researcher, responsible for supporting the intervention process, was replaced during the study, but the newcomer had a 1-month training period. Otherwise, the study proceeded according to plan.
Based on the diaries kept by the personnel of the kitchens, the researchers thoroughly described all ergonomic changes and evaluated the significance of the changes with regard to the load on the musculoskeletal system or occupational safety. The changes were classified according to work tasks and by target.
Outcomes
The main outcomes were the prevalence rates of musculoskeletal pain in seven anatomical sites (neck, shoulders, forearms/hands, low back, hips, knees and ankles/feet), a mean score of trouble caused by pain during the past 3 months (1 = “not at all”, ... , 7 = “very much”) and of local fatigue after the work day during the past 7 days (1 = “not at all”, ... , 6 = “very much”), and musculoskeletal sick leave (yes/no) during the past 3 months. The mean scores were calculated only if responses for all sites were available. In the questionnaire, a manikin illustrated the body regions.
The intermediate outcomes were changes in perceived physical workload (1 = “not at all”, ... , 7 = “very strenuous”) and in psychosocial factors, that is stress during the past month (1 = “no stress at all”, ... , 3 = “much stress”), mental strenuousness of work (1 = “not at all”, ... , 3 = “very strenuous”), and job satisfaction (1 = “satisfied”, 2 = “undecided”, 3 = “dissatisfied”).
Sample size
Based on power calculations (assumptions: intraclass correlation 0.50, α 0.05, power 0.80, 15% difference between the compared groups, average of three subjects per kitchen), the number of kitchens needed was 80 per group. The initial aim was to enroll in the study all eligible voluntary kitchens in four cities. At baseline, the empirical intraclass correlations were low for the main outcomes (between 0.03 for sick leave and 0.10 for the mean score of trouble), and the intermediate outcomes (between 0.0 for stress and 0.16 for physical strenuousness of work). Intraclass correlations of workers in the same city area varied from 0.0 to 0.06. Although the number of kitchens was smaller than the power calculation requirement, the sample size was sufficient because the intraclass correlation assumption proved to be overestimated.
Statistical analysis
Data were analysed according to the intention-to-treat principle. Three kitchens were dropped out after randomisation (fig 1) and were not included in the analyses because only baseline data were available. The success of the randomisation was evaluated by comparing the results of the baseline questionnaires between the two groups (table 1).
All the analyses and the results presented in the figures or tables were based on cross-sectional open population data (n = 504). Prevalence rates and mean scores were assessed. Differences between the groups in different cross-sections were studied using mixed and logistic regression models.31 In the mixed model, the kitchen series and individual kitchens were interpreted as random variables, and the study arm, city, and potential covariates (baseline level of the outcome, job satisfaction, age, gender, smoking, physical exercise, body mass index, and permanent vs fixed-term employment) as fixed variables. Effects of covariates on the results were tested at post-intervention assessment (PIA) and at PI12 (the 1-year follow-up). Among the subgroup of subjects that remained working in the same kitchens throughout the study (cohort analysis, n = 307), re-analyses were made using the repeated measures design. All p values were two-tailed. Statistical analyses were performed using the SAS version 9.1 and SPSS version 12.0.1.
Turnover of workers and loss to follow-up
The proportion of workers employed in the same kitchen throughout the intervention phase was 86% in the intervention group and 84% in the control group. During the 1-year follow-up, the proportions were 70% and 71%, respectively.
The number of workers participating in different cross-sections is shown in table 2. Due to summer holidays at schools, at least one questionnaire was skipped in each kitchen series. Five series finished the intervention at 9 months (I9, n = 157) and 11 series at 12 months (I12, n = 295). The PIA was thus made either at 9 or 12 months after the start of the implementation phase (combined n = 452). The next questionnaire (PI3) was always 3 months after the PIA.
The number of missing values in the health outcome variables was small and similar in the study arms, being highest in the fatigue score (8%–12% in the intervention group, 4%–13% in the control group). While missing values in psychosocial factors were rare (<3%), in perceived physical workload the missing proportion varied between 3% and 25% in the intervention group and between 2% and 16% in the control group.
RESULTS
On average, 73% of the workers participated in the workshops. Altogether 402 ergonomic changes evaluated by the researchers as significant with regard to load on the musculoskeletal system or occupational safety were implemented. The changes mostly concerned the ergonomics of dishwashing (23%), cooking and baking (18%), and distribution and serving of food (18%). Changes were also made in cleaning and maintenance of room and equipment (15%), packing food for delivery (9%), preparation (8%), receiving and storing of raw material (8%), and office work (1%). When considered by target, the changes were distributed as follows: 41% of the changes were related to work organisation, methods and practices; 27% to machines, equipment, and tools; 13% to layout and furniture (eg, deletion of doorsteps); 10% to physical work environment and safety (eg, removing objects presenting risk of injury); 6% to materials (eg, new package sizes); and 3% to some other targets.
In the control group, 80 ergonomic changes were spontaneously implemented within normal activity. The control kitchens implemented more changes in cooking and baking (39% vs 18%) and less in receiving and storing of raw material (2% vs 15%) than the intervention kitchens. Otherwise, the distribution of changes was similar. In the control group, machines, equipment and tools received most attention (52%), whereas in the intervention group the largest proportion of changes was targeted at work organisation and methods (41%).
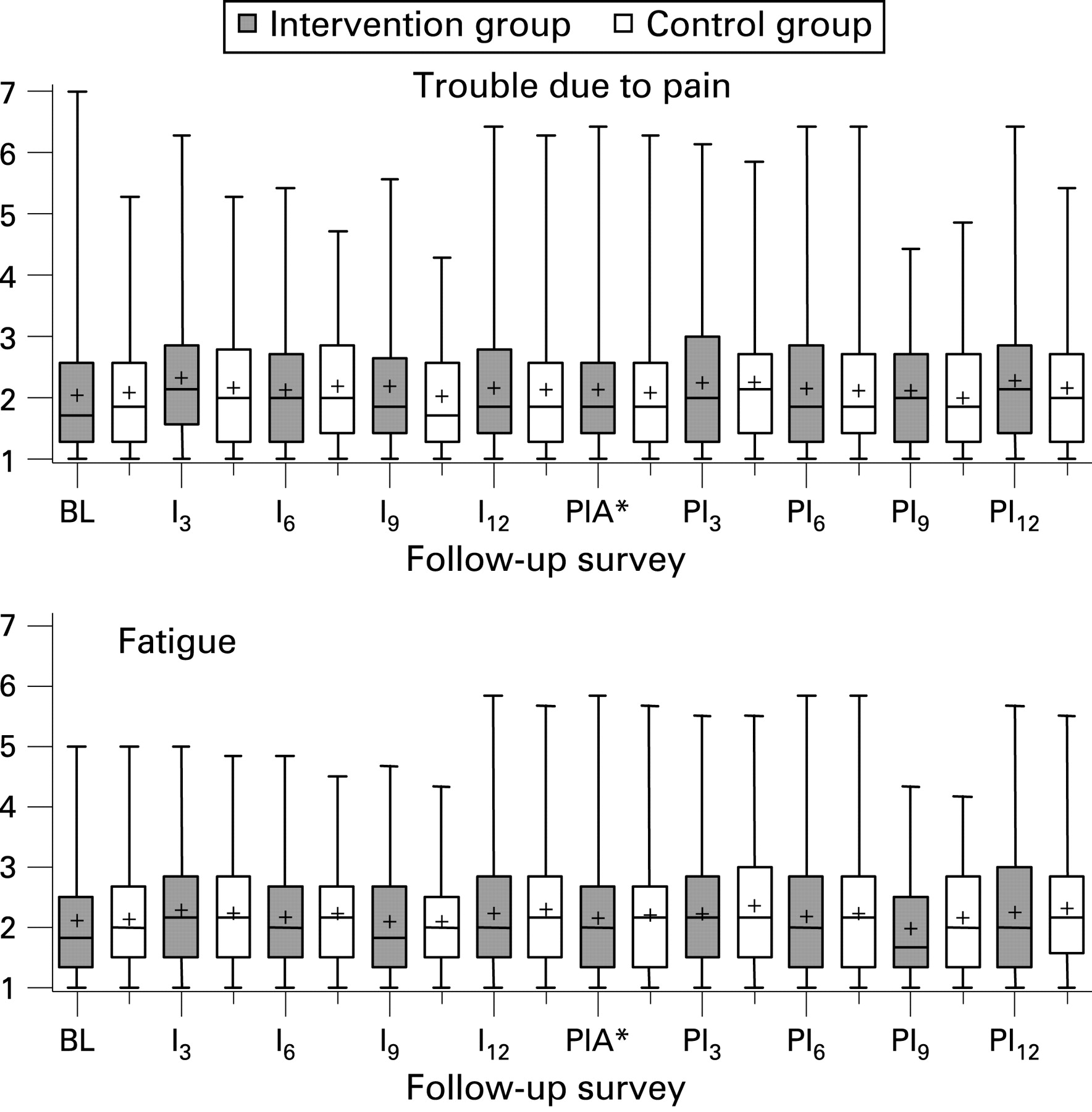
The prevalence rates of musculoskeletal pain and sick leave, the mean score of trouble caused by pain during the past 3 months, and the mean score of local musculoskeletal fatigue after a work day during the past 7 days were similar in the intervention and control group (figs 3–4). Although some statistically significant differences in a direction contrary to our assumption were found between the groups in the cross-sections, no systematic trend was seen in any outcome variable. Inclusion of potential baseline confounders did not change the results. The results did not appreciably change in the cohort analysis, that is among those workers who remained in the same kitchen throughout the study (n = 307).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in the intermediate variables on perceived physical workload showed no effect of intervention (table 3). Job satisfaction declined in the intervention group and was poorer than that in the control group at the PIA and at the 1-year follow-up. Mental strenuousness of work and stress were higher at the 1-year follow-up than at the earlier phases of the study in both the intervention and control group, but no statistically significant differences between the groups were observed.
DISCUSSION
In this cluster randomised controlled trial we evaluated the efficacy of a participatory ergonomics intervention in preventing the occurrence of musculoskeletal disorders among an open population of kitchen workers. No systematic differences between the intervention and control group were found in the health outcomes. Neither did changes in the intermediate variables on perceived physical workload show any effect of the intervention. The effects of the ergonomic changes on objectively assessed workload will be reported later. A trend towards increased stress, mental strenuousness of work and job dissatisfaction in the intervention group was observed.
We chose a target group in which the occurrence of musculoskeletal disorders is high and which would therefore be a fruitful subject for ergonomic improvements. We consider this study to be an efficacy-oriented trial, conducted under randomised and experimentally near-ideal conditions. To our knowledge, this is the first, large, cluster randomised controlled trial on the effects of participatory ergonomics. We detected only one study with a similar design32 in which no effect of participatory ergonomics was found in reducing physical work demands in construction companies.
Participatory ergonomics is a complex and ambiguous concept. There is a range of ways and models of doing participatory ergonomics and no general agreement about the term exists.33 Although not cluster randomised, a similar approach as ours has been used earlier.34–36 In these studies the intervention was based on participatory ergonomics teams, whereas in our model the role of the workers as actors was emphasised and the role of the management was to organise resources and support to implementation of changes.
Despite our intensive intervention of about 1 year’s duration and with eight workshops (total 28 h), no effect on musculoskeletal health was found. In the intervention group the prevalence of pain seemed to be stable or even rising, and especially the sick leave increased compared to the control group. This was contrary to our hypothesis. The intervention, regardless of its burden, was well received by both the workers and management. None of the kitchens dropped out during the intervention, and response rates and participation in the workshops were excellent, indicating good compliance and commitment to the study.
Based on research diaries, questionnaires, and focus group interviews, the participatory approach and intervention process as such were successful, well accepted and perceived as motivating. The workers’ ergonomics knowledge level increased and, in the workers’ own words, they developed an “eye for ergonomics” regarding their own work and that of others.30 37 On the other hand, the workers expected more support from the researchers, technical staff and management. The more satisfied the kitchens were with the support from management, the better were the effects of the intervention as evaluated by the workers.30 The major observed obstacles in improving kitchen ergonomics were passivity and resistance to change,37 and the most general reasons for non-completion of changes were lack of motivation or time.30
Among the strengths of our study were sufficient power (80%) and good comparability between the groups. Stratification by area and type of kitchen ensured balanced clusters with respect to baseline characteristics. Despite the staff turnover, the groups remained similar through the intervention phase with regard to assessed potential confounders. In both groups, about 70% of the baseline population was employed in the same kitchen throughout the study. Strict quality control was applied to ensure similarity of working methods between the researcher teams in different cities.
Baseline data collection was made blinded to the group status, and the researchers had no access to the questionnaire data during the data collection. Otherwise blinding and the use of placebo treatment are practically impossible in studies of ergonomics. All the participating workers were asked not to talk about the study process in case they changed kitchen. Only two workers were transferred from an intervention to a control kitchen during the intervention, so that contamination was probably minor.
Personal visits of a researcher to each of the kitchens to motivate answering may have been one reason for the excellent response rates. The researcher also documented changes in the control kitchens based on short interviews. The visits can be interpreted as a kind of intervention for the control kitchens, but any contribution to the results is speculative. The visits may have increased awareness of musculoskeletal disorders also in the control kitchens, which could have reduced information bias regarding musculoskeletal outcomes. Documentation of the changes during the visits may have activated the workers in the control kitchens to carry out more changes, which could have diluted the overall effect. Nevertheless, the difference in the number of changes made in the intervention kitchens and those that occurred spontaneously in the control kitchens (402 vs 80) is considerable.
In previous studies25 27 the number of portions prepared per staff making them has been associated with musculoskeletal symptoms. According to the research diaries, in about one-third of both intervention and control kitchens the amount of portions increased during the study. A decrease in the number of personnel was recorded in four intervention and 11 control kitchens. This may have led to a somewhat higher intensification of work in the control kitchens. Simultaneously with the intervention, major organisational reforms in foodservice occurred in two of the participating cities. It is possible that in the middle of organisational changes and tightened work demands the participatory implementation of the ergonomics intervention was overly straining to the employees. The increased proportion of subjects dissatisfied with their work, and the trend towards increased mental stress and strenuousness of work in the intervention group, deserve further attention, and results of more detailed stratified analyses will be reported elsewhere. It is to be noted, however, that the comparability of the intervention and control groups persisted in spite of the organisational reforms, because the study design guaranteed that within each series the kitchens of both study arms proceeded parallely in time.
Our female-dominated, middle-aged target group with high physical work demands, musculoskeletal pain prevalence and disability pension incidence in Finland38 was challenging. At baseline, 53% of the women reported pain in at least the axial (neck and low back) and upper limb areas, and 48% in at least the axial and lower limb areas. Further, 36% reported concurrent pain in all three areas.39 Multiple-site pain seems to be prevalent among manual handling workers40 particularly in women. Multiple-site pain generally increases with age41 and seems to be persistent.42
The high prevalence of multiple-site pain observed among the current study subjects39 could be connected with workload being rather uniformly distributed on the musculoskeletal system in kitchen work. Several risk factors for the development of musculoskeletal disorders can be identified in daily kitchen work and many tasks include exposure to a combination of these risk factors. For example, in long-lasting dishwashing frequent bending and twisting of the trunk, lifting, repetitive movements of the hand, non-neutral wrist and shoulder postures, and use of hand force often occur. Our results on physical risk factors based on expert assessment showed for some, but not all work tasks, reduction of the level of exposure (results will be reported elsewhere). It seems that the changes were not strong enough to influence the health outcomes. In some kitchens, acquisition of expensive new equipment and extensive structural changes would have been needed. While no extra funding was available, most of the changes were low-cost solutions.
Thus, it may be that the intervention was not intensive enough, or that a longer follow-up would have been needed to note impacts on the musculoskeletal system. Given the episodic nature of musculoskeletal disorders, our 3-month prevalence measures may not have been optimal to capture a change in the frequency of spells of musculoskeletal disorders. The measures of local musculoskeletal fatigue during the past 7 days were more sensitive. However, no effect was detected using the fatigue measure either. A source of bias in our results might arise from the fact that the workers had an active role in implementing the ergonomic changes and the outcome assessments were based on their subjective reports. It is conceivable that their involvement in an intervention programme increased the workers’ awareness of both ergonomics as well as musculoskeletal problems.
The results may reflect the difficulty of affecting the heavy overall physical and mental load in kitchen work without redesigning work processes and making structural changes in the kitchens. Developing the work environment and work processes requires smooth collaboration between architects, planners and management, as well as the technical staff and kitchen workers themselves as the best experts in their own work.
In conclusion, while this participatory ergonomics approach was successful in engaging the kitchen workers to evaluate and improve the ergonomics of their daily work, no effect of the intervention on musculoskeletal health was found. The ergonomic changes did not reduce perceived physical workload. The intervention and simultaneous organisational changes external to the intervention in some of the municipalities might have increased mental strenuousness of work and decreased job satisfaction. There was no possibility to affect the basic design of the kitchens or the amount of work by the intervention. It may be that a more comprehensive redesign of work organisation and processes is needed, taking more account of workers’ physical and mental resources.
Main messages
While this participatory ergonomics intervention was successful in engaging the kitchen workers to evaluate and improve the ergonomics of their daily work, no evidence was found for the efficacy of the intervention in preventing musculoskeletal disorders.
There is a need for further trials to elucidate the issue.
Policy implications
The findings do not support implementation of participatory ergonomics intervention as studied in the present trial.
It may be that to obtain favourable effects on the musculoskeletal health of the employees, a more comprehensive redesign of work organisation and processes in the kitchen setting is needed, taking more account of workers’ physical and mental resources.
Acknowledgments
The authors thank members of the ERGO research group: Samuel Dadzie, Tomi Järvinen, Ritva Lehto, Mika Nyberg, Jarmo Sillanpää, Anne Ranta and Riikka Ranta. We would like to express our warmest gratitude to the collaborating parties, the municipalities of Espoo, Tampere, Turku, and Vantaa. We are indebted to Richard Burton, BSc, for his language review of the manuscript. The Academy of Finland (Health Promotion Research Programme), the Finnish Work Environment Fund, the Ministry of Labour, and the Local Government Pensions Institution financially supported this work.
REFERENCES
Footnotes
Funding: The Academy of Finland (Health Promotion Research Programme), the Finnish Work Environment Fund, the Ministry of Labour and the Local Government Pensions Institution.
Competing interests: None.
Ethics approval: The Ethics Committee of the Finnish Institute of Occupational Health approved the study proposal.
Patient consent: Obtained.