Article Text

Abstract
Background: Wood dust (WD) has been designated a human carcinogen that can cause sino-nasal cancers. However, evidence of its association with other upper aero-digestive tract and respiratory (UADR) cancers is inconsistent.
Objective: To examine the relationship between WD exposure and the risk of different histological subtypes of UADR cancers.
Methods: In a hospital-based case-control study conducted at Roswell Park Cancer Institute, Buffalo, NY, USA, an examination was carried out to determine the effect of self-reported WD exposure on 1522 male UADR cancer cases (241 oral and oropharyngeal, 90 nasal cavity, nasopharyngeal and hypopharyngeal, 124 laryngeal, 809 lung and tracheal and 258 oesophagus and gastric cardia) and 1522 male controls, frequency matched on age and smoking history. Odds ratios (OR) were calculated after adjusting for relevant risk factors including tobacco smoking.
Results: The results show that regular WD exposure was associated with a statistically significant increased risk of 32% for all UADR cancers (OR 1.32; 95% CI 1.01 to 1.77; p-trend = 0.05) and 69% for lung cancer alone (OR 1.69; 95% CI 1.20 to 2.36; p-trend = 0.007). WD was associated with an 82–93% increased risk of squamous cell, small cell and adenocarcinoma of the lung and more than twice the risk of developing squamous cell carcinoma of the nasal cavity, nasopharynx and hypopharynx, with a significant dose–response relationship. Oral and oropharyngeal cancers showed a non-significant increase in risk. A significant increase in risk of laryngeal and lung cancers was noted for subjects regularly exposed to WD for >20 years. Cancers of the oesophagus and gastric cardia did not show any risk associated with WD. WD was associated with a significantly greater risk of UADR cancers among people who had ever smoked than never smokers.
Conclusion: WD exposure is a potential risk factor for UADR cancers, especially for cancers of the nasal cavity, nasopharynx, larynx and lung.
Statistics from Altmetric.com
In 2002, 5.8 million new cancer cases were diagnosed worldwide, 2.5 million of which were collectively accounted for by cancers of the head, neck, oesophagus and respiratory tract.1 For the purpose of this paper, cancers of the upper digestive tract (extending from the oral cavity to the gastric cardia) and the respiratory tract (extending from the nasal cavity to the lung) are collectively described as upper aero-digestive tract and respiratory (UADR) cancers. More than 70% of new UADR cancers occur in males and account for almost 1.4 million cancer related deaths each year worldwide. The male to female incidence ratio varies from 2:1 for oral cancer to almost 7:1 for laryngeal cancer.1 In the USA, UADR cancers contribute about 160 000 new cases and 108 500 male deaths each year, accounting for more than 20% of all new cancer cases and more than 37% of all cancer related deaths in males. Among US males, the 5-year survival rate is about 15% for lung and oesophageal cancers and about 58% for oral cavity and pharyngeal cancers.2 Worldwide, the survival rates are as low as 4% for lung and oesophageal cancers among males in sub-Saharan Africa.1
Tobacco smoke and alcohol are considered to be the primary risk factors for UADR cancers. Almost 30% of all cancer deaths and 87% of lung cancer deaths are accounted for by smoking.3 Worldwide, about 25–40% of all oral, pharyngeal, laryngeal and oesophageal cancers can be attributed to drinking alcohol.4 A synergistic effect of alcohol and smoking has also been reported for UADR cancers.5–7 However, only 10% of smokers and even fewer drinkers go on to develop cancer. This suggests that there may be many other factors which contribute to cancer development, either as independent carcinogens or by interacting with known carcinogens. Genetic predisposition, diet, obesity, environmental and occupational factors are some of the factors associated with carcinogenesis. Among industrial or environmental factors, substances such as asbestos, radon, wood dust (WD) and air pollution are considered to have significant carcinogenic potential.
WD has been recognised as a harmful by-product of manufacturing. Saw mills, furniture manufacture, carpentry and cabinet making are some areas identified as having high sawdust exposure.8 A survey conducted in the early 1980s has shown that about 2.1% of the total US workforce was employed in industries related to wood products.9 In 1990, it was estimated that the USA produced 24% of all sawed wood in the world.8 Between the 1970s and 1990s several studies were published establishing the association between WD exposure and nasal cavity and sinus cancers.10–13 Based on this evidence, the International Agency for Research on Cancer (IARC) designated WD as a human carcinogen in 1995.8 In 2002, the National Institutes of Health (NIH) identified WD as a “known human carcinogen”.
As mentioned above, strong evidence has emerged establishing the risk for sino-nasal adenocarcinoma. However, studies examining the effect of WD on other UADR cancers (oral cavity, pharynx, larynx, lungs and oesophagus) have not shown consistent results. Given the possibility that a sizeable percentage of the workforce might have been exposed to occupational WD, it is important to understand the relationship between WD exposure and cancer and its interactions with known risk factors. Therefore, we conducted this case-control study to study the association between WD exposure and different histological types of UADR cancers.
METHODS
Study population
Between 1982 and 1998, all new inpatients and outpatients at Roswell Park Cancer Institute (Buffalo, New York, USA) (RPCI) were asked to voluntarily complete a patient epidemiological data system (PEDS) epidemiology questionnaire at the time of registration. More than 36 500 cancer and non-cancer patients consented and completed the questionnaire, which constituted 50% of all those approached. Participation was unrelated to clinical evaluation or treatment. Informed consent was obtained from all participants and the Institutional Review Board of RPCI approved the procedures for protection of human subjects in this study. If incomplete or missing data were discovered, participants were contacted via phone or mail to complete the forms. Complete information was available on about 27 000 participants. Patients’ data were regularly matched to the RPCI tumour registry data to update the cancer status. Over 15 000 of the cancer patients were linked to histology data from the tumour registry. Controls included people who visited the hospital with a suspicion of cancer and those who were screened as outpatients at RPCI but were not diagnosed with any malignant or benign tumours. The study sample for the current analysis was selected from this database.
Since occupational exposure to WD was uncommon among females, this analysis was restricted to males. The cancers selected included all head and neck cancers including oral cancers (excluding melanoma of the lip and salivary gland cancers), nasal cavity and pharyngeal cancers, laryngeal cancers, lung and tracheal cancers (excluding sarcomas and lung lymphomas) and cancers of the oesophagus and gastric cardia. The cancers were selected based on ICD codes.
The database included 1765 UADR cancer cases and 2590 eligible male controls. About 12% of the cases and 9% of the controls were missing WD exposure information or other important variables such as age and smoking status and were excluded from this analysis. Therefore, 1522 UADR cancer cases were identified for this analysis. The case group included 241 oral or oropharyngeal, 90 nasal cavity, nasopharyngeal or hypopharyngeal, 124 laryngeal, 809 lung or tracheal and 258 cancers of the oesophagus or gastric cardia. Controls were randomly selected and were frequency matched to cases at a ratio of 1:1 based on 10-year age groups and smoking history (never smoked/ever smoked). The controls were diagnosed with conditions distributed across 39 different disease classifications including 4.5% oral or upper GI diseases, 8% respiratory disorders, 22% infectious or parasitic diseases, 12.5% circulatory disorders, 20% digestive and abdominal disorders, 14% genito-urinary diseases and 10% other disorders. The remaining 9% were admitted for observation but received no diagnosis or were outpatients for screening.
Questionnaire
The 16-page comprehensive epidemiological questionnaire covered topics such as lifetime tobacco and alcohol use, diet, personal activity patterns, occupational and environmental exposure, education, residential history, reproductive, medical and family history and many other variables of general epidemiological interest. WD exposure was assessed through several questions about prior exposure at work. The subjects were asked if they were exposed to WD at work. If yes, they were queried about the frequency of exposure and were required to grade it as: usually/occasionally/never/don’t know. However, no further definitions of these exposure levels were provided in the questionnaire. The subject was also asked about the duration of exposure (number of years exposed to WD at work) and the year the occupational WD exposure began. A comprehensive smoking history was also obtained. Subjects who had smoked cigarettes every day for at least 1 year were classified as smokers, while all others were classified as non-smokers.
Data analysis
The same control group was used for the overall analysis and for the stratified analysis of subsites of UADR cancers. The duration of WD exposure was stratified as never exposed, <20 years of exposure and ⩾20 years of exposure. Pack years of smoking was stratified as 20 pack years or less, >20 pack years to 45 pack years and >45 pack years. These stratification schemes were based on the distribution of exposure among the control group. An analysis of occupation type and industry was not carried out because a majority of subjects had incomplete data for these variables. However, a cumulative variable of intensity and duration of WD exposure was calculated to address the possibility of bias due to inadequate assessment of exposure. The cumulative estimate was stratified into three categories: (1) never exposed group, (2) moderate exposure group (occasionally exposed or regularly exposed for less than 20 years) and (3) high exposure group (regularly exposed for 20 years or more). For this analysis, patients who reported they had quit smoking less than a year before completing the questionnaire were considered current smokers. All dichotomous and stratified data are summarised by group totals and percentages and continuous variables are summarised by mean and standard deviation. Pearson’s χ2 and Student’s t test were used to obtain p values for categorical and continuous variables, respectively. p Values of ⩽0.05 were considered significant. Unconditional logistic regression was used to calculate odds ratios (OR) and 95% confidence intervals (CI). ORs were adjusted for statistically significant covariates in the model and also for potential confounders based on established risk factors. Different models were used for each subgroup analysis based on the above mentioned strategy. All analyses were performed using SPSS version 13.0 (SPSS, Chicago, IL).
RESULTS
Demographic characteristics
The demographic characteristics of all UADR cases and controls are summarised in table 1. Due to successful matching, age is comparable between case and control groups. The mean age for all UADR cases was 62 years and the mean age for the controls was 61.4 years. A majority of the cases and controls (94% and 96%, respectively) were Caucasian (data not shown). A large proportion (89%) of the survey participants were either current or former smokers in both groups. However, more cases were current smokers compared with controls (p<0.001). Lung cancer and head and neck cancer cases had the highest proportion of current smokers (41.4% and 40%, respectively). Furthermore, cases were heavier smokers compared with controls (p<0.001) across packs/day, years of smoking and pack years, with lung cancer patients being the heaviest smokers. Cases were also heavier drinkers, particularly head, neck and oesophageal cancer cases. Lung and head and neck cancer cases had a significantly higher exposure to asbestos compared with controls. On average, controls had a higher body mass index than cases, except for oesophageal cancer cases. Cases were also less educated (p = 0.001) and had a lower family income (p = 0.001) compared with controls.
Association of WD exposure and UADR cancers
Table 2 shows the risk estimates for UADR cancers associated with WD exposure. Subjects who were never exposed to WD served as the referent group for all analysis. The results show a statistically significant 32% increase in risk of all UADR cancers associated with regular exposure to WD (adjusted OR 1.32; 95% CI 1.01 to 1.77; p-trend = 0.05). This risk estimate was adjusted for age, education, body mass index, pack years of smoking, family income and year of completing the questionnaire.
When the risk of WD exposure was assessed among 809 lung cancer patients and 1522 controls, a statistically significant 69% increase in risk was noted for cases regularly exposed to WD (adjusted OR 1.69; 95% CI 1.20 to 2.36; p-trend = 0.007). Oral and oropharyngeal, nasal cavity and nasopharyngeal and laryngeal cancer subgroups showed a statistically non-significant 14–57% increased in risk associated with regular WD exposure. However, cancers of the oesophagus and gastric cardia showed a non-significant 23% increase in risk only among occasionally exposed subjects. As mentioned in the Methods section, different models were used for each subgroup analysis and adjustment was carried out for variables which were significant in each individual model.
Duration and intensity of WD exposure and UADR cancer risk
Duration of WD exposure was stratified as less than 20 years of exposure and 20 years or more and was compared with people who were never exposed to WD (data not shown). Results for all UADR cancers combined show that WD exposure of 20 years or more was associated with a non-significant 9% increase in risk. Among the subgroups, lung cancer showed a statistically significant 42% increase in risk associated with at least 20 years of WD exposure (adjusted OR 1.42; 95% CI 1.05 to 1.91). There was also a significant dose–response relationship associated with increasing duration of WD exposure (p-trend = 0.04). Oral cavity, nasal cavity, pharyngeal and laryngeal cancers showed a non-significant 4–8% increase in risk with no significant dose–response relationship.
Table 3 presents the cumulative effects of intensity and duration of WD exposure on the UADR cancers. Overall, all UADR cancers showed a significant 69% increase in risk among the high exposure group, with a significant dose–response relationship (adjusted OR 1.69; 95% CI 1.09 to 2.64; p-trend = 0.04). The high exposure group was associated with more than twice the risk of developing lung cancer compared with the controls (adjusted OR 2.15; 95% CI 1.31 to 3.56; p-trend = 0.009). The maximum exposure group also showed a statistically non-significant 35% increase in risk of nasal cavity and nasopharyngeal cancer and twice the risk of laryngeal cancer. However, the small number of cases in the high exposure category for these cancers limits the interpretation of these results.
WD exposure and risk of different histological subtypes of UADR cancers
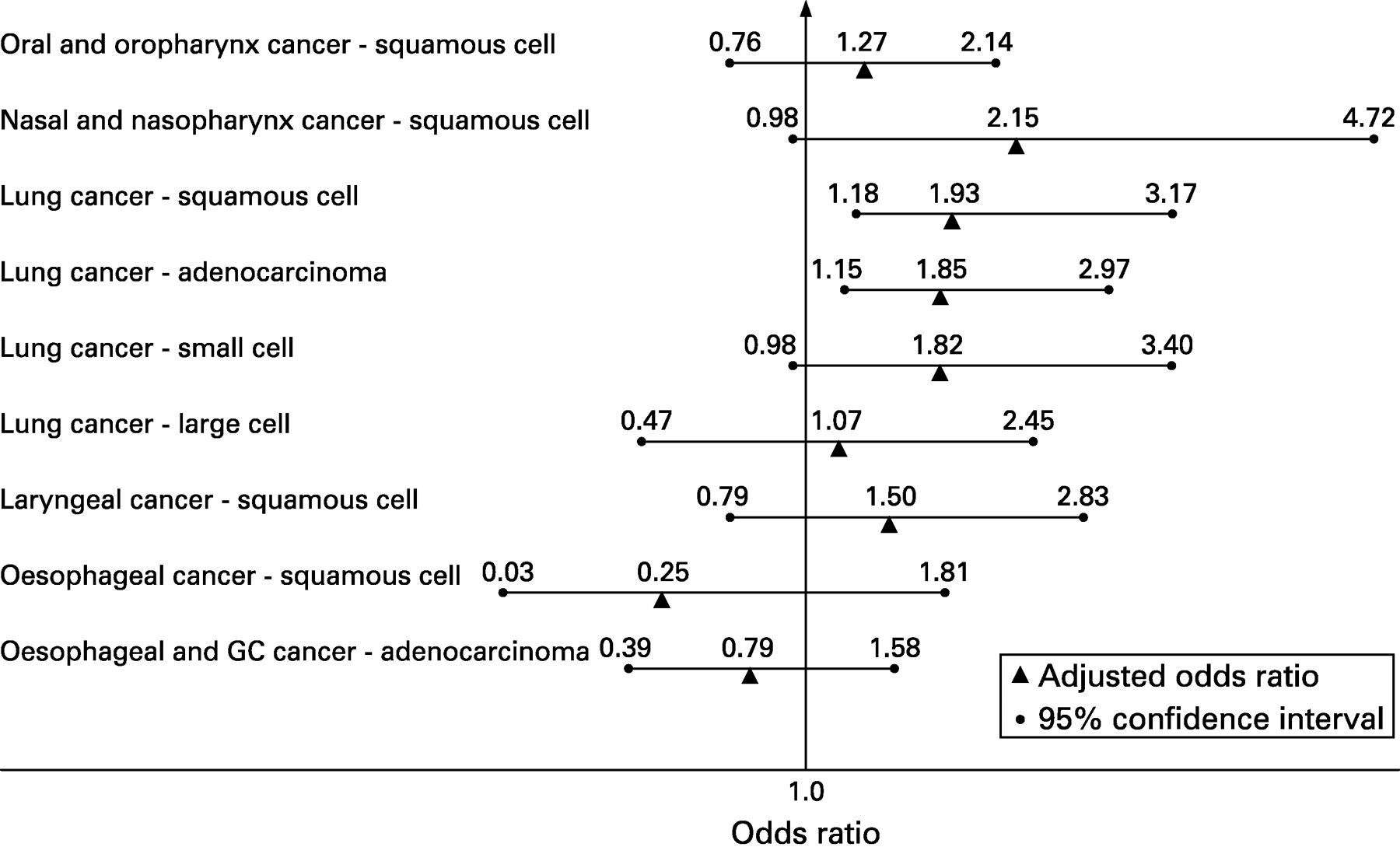
Figure 1 and tables 4 and 5 summarise the effects of WD exposure on different histological subtypes of UADR cancers. Table 4 reports the effect of WD on squamous cell carcinoma of the UADR tract. Regular exposure to WD was associated with a non-significant 33% increase in risk of all squamous cell UADR cancers. Regular exposure to WD was also associated with more than twice the risk of squamous cell carcinoma of the nasal cavity, nasopharynx and hypopharynx, with a significant dose–response relationship (adjusted OR 2.15; 95% CI 0.98 to 4.72; p-trend = 0.02). Squamous cell carcinoma of the lung showed a statistically significant 93% increased risk associated with regular WD exposure (adjusted OR 1.93; 95% CI 1.18 to 3.17; p-trend = 0.003). Laryngeal squamous cell carcinomas showed a non-significant 50% increased risk associated with regular WD exposure. Regular WD exposure showed a non-significant reduction in risk of oesophageal squamous carcinomas. However, the numbers were too small for any valid interpretation. More studies with a larger number of subjects are required to examine the relationship.
{kind=link}
Table 5 shows the effect of WD exposure on non-squamous UADR cancers. Regular exposure to WD was associated with a statistically significant 85% increase in risk of adenocarcinoma of the lung (adjusted OR 1.85; 95% CI 1.15 to 2.97; p-trend = 0.03). A borderline significant 82% increase in risk was also noted for lung small cell carcinoma. However, no significant association was noted for undifferentiated large cell carcinoma or for non-lung adenocarcinoma of the UADR tract. Our database contained very few adenocarcinoma of the nasal cavity and paranasal sinuses, so they were not analysed separately.
Figure 1 summarises the adjusted OR and 95% CIs for risk of different histological subtypes of UADR cancers associated with regular WD exposure. Seven of the nine histological subtypes of UADR cancers showed an increased risk associated with WD exposure, with five of the nine showing an increased risk of 50% or more compared with controls.
Combined effect of smoking and WD on UADR cancers
Smoking is a well known risk factor for UADR cancers. To assess the potential confounding effect of smoking on the relationship between WD and UADR cancers (data not shown), smoking effect was examined based on smoking status (never, former or current smokers) and also quantified by pack years of smoking (non-smokers, ⩽20 pack years, >20 to 45 pack years and >45 pack years). The models based on groups stratified on smoking status were adjusted for age, pack years, education, family income, year of enrolment and the models for pack year groups were adjusted for the same variables after replacing pack years with smoking status.
Regular WD exposure was associated with a 47–49% increase in risk among both former and current smokers and former smokers showed a significant dose–response relationship (p-trend = 0.04). However, the risk increase was not statistically significant in non-smokers, probably due to the small number of non-smokers in the study population. Regular WD exposure was associated with a 40–41% increase in risk among all three pack year strata (⩽20, >20 to 45 and >45 pack years) compared with non-smokers. Only the ⩽20 pack years group showed a significant dose–response trend (p-trend = 0.05).
DISCUSSION
Mechanism of cancer risk
About 58% of wood harvested worldwide is hard wood and is mostly used for fuel. On the other hand, more than two-thirds of wood used for industrial purposes is soft wood (conifers). Exposure to soft WD has been reported to cause a variety of conditions such as dermatitis, respiratory ailments (eg, asthma), mucosal and non-mucosal effects, and possibly cancers.8 However, most of the available scientific literature associates risk of sino-nasal adenocarcinoma mainly with hard rather than soft wood.14
WD is generated in the industry during the process of drilling, chipping, sawing or shaping wood. When a person breathes in WD it can be deposited in the nose, throat and airways. The location of particle deposition is determined by the size, shape and density of the dust particle and also the strength of airflow. Particles larger than 5 μm are deposited in the nose, while the smaller particles are deposited in the smaller airways.8 15 16 Cancer aetiology could be driven by decreased muco-ciliary clearance and increased deposition, leading to increased inflammatory response and cellular changes, or DNA damage.8 Celik et al have shown that exposure to WD was associated with increased frequency of micronuclei and nuclear changes in buccal epithelium, leaving the epithelial tissue of people exposed to WD at a greater risk of genetic damage.16
Several studies have examined the risk effects of WD on different cancers. Case-control studies involving industrial exposures showed increased relative risks for nasal cancer among furniture workers (relative risk 4.4; 95% CI 1.3 to 15.0) and among “other” wood workers (relative risk 4.0; 95% CI 1.5 to 11.0).17 18 Outcome data for both studies were collected by reviewing local death certificate information. Blot et al summarise the results from several cohort and case-control studies examining occupational exposures to WD both in Europe and in North America.19 Interestingly, there was great variation in the increased sino-nasal adenocarcinoma risks between both continents, possibly explained by variations in wood types or by occupational safety measures having been implemented earlier in North America.
Cancer mortality data from the American Cancer Society’s Cancer Prevention Study-II were used to investigate the associations between WD exposures and multiple cancer types.20 Several cancers showed a small but statistically significant increased risk when subjects had been exposed to WD through employment. For example, lung cancer incidence was positively associated with overall duration of WD exposure; however, only in the 10–19-year exposure group was this association significant.
A retrospective cohort study of Estonian furniture workers did not find a statistically significant increased UADR cancer risk, but other cancers such as colon and rectal cancers did have a significantly increased risk, particularly for those subjects who were exposed to WD for 10 years or more.21
In a case-control study carried out between July 1995 and October 2002 to investigate occupational exposure to WD and risk of lung cancer, a fairly large population (1368 cases and 1192 controls) was evaluated through an epidemiological questionnaire. Results from this study showed significant elevated adjusted odds ratios based on longer employment in WD related industries (OR 3.15; 95% CI 1.45 to 6.86).22 A recently published cohort study in Finland followed census-based occupational exposure to eight different organic dusts, including WDs, between 1908 and 1945. Although organic dusts were not found to be major risk factors for respiratory cancers (including lung cancer), they were associated with a slightly increased risk of nasal cancer (standardised incidence ratio 1.42; 95% CI 0.79 to 2.44).23
Gustavsson et al conducted a case-control study to analyse the occupational exposure and risk of cancers of the oral cavity, pharynx, larynx and oesophagus. They noted that WD exposure was associated with a decreased risk of squamous cell carcinoma of these sites.24 A Swedish cohort study also found that WD exposure was associated with an increased risk of gastric cardia cancers, whereas no relationship was noted with squamous cell carcinoma of the oesophagus.25
Thus, while some published reports on the association of WD exposure and UADR cancers suggest an increased risk, the evidence has mostly been inconsistent.
Summary of results
Our results show that regular WD exposure is associated with an increased risk of UADR cancers. The association is statistically significant for lung and tracheal cancers. Squamous cell carcinoma and adenocarcinoma of the lung showed a statistically significant 85–93% increase in risk and small cell carcinoma showed an 82% increased risk, which was borderline significant. Large cell carcinoma of the lung did not show any association. Nasal cavity, pharyngeal and laryngeal cancers showed a non-significant increase in risk. Regular WD exposure was associated with more than double the risk of squamous cell carcinoma of the nasal cavity, nasopharynx and hypopharynx, and also showed a significant dose–response relationship. Oesophageal and gastric cardia cancers do not show any increase in risk associated with WD exposure. Regular exposure over a 20-year period was associated with more than double the risk of laryngeal and lung cancers. The risk of UADR cancer associated with regular WD exposure was significantly greater in smokers but not among non-smokers, suggesting a co-carcinogenic effect between smoking and WD.
Main messages
-
Wood dust exposure is a potential risk factor for upper aero-digestive and respiratory cancers, especially of the nasal cavity, nasopharynx, larynx and lung.
-
An increase in risk associated with wood dust exposure was noted among all histological subtypes of lung cancer.
-
The risk of upper aero-digestive and respiratory cancers increased with increasing intensity and duration of wood dust exposure, showing a clear dose–response relationship.
Policy implications
WD exposure is well recognised as a carcinogen, especially for nasal cavity and sinus cancers. Our results show that wood dust is a potential carcinogen not only for sino-nasal cancers but also for other upper aero-digestive and respiratory cancers.
Strengths and limitations
A few methodological issues should be considered in interpreting our study results. One limitation, as in most case-control studies, is recall bias that could affect the validity of the current findings. The subjects in our control group included people who visited our hospital with a suspicion of cancer but were found to be free of any cancer. All patients were approached for participation at the time of registration. The subjects who did not consent were not followed up for this study, so their eventual disease status could not be verified. While the possibility of bias exists, it is difficult to estimate if the response rate would be lower or higher in the case or control group. The subjects were requested to grade their frequency of exposure as never/occasional/regular. However, no clear definition of these levels was provided on the questionnaire, introducing a possibility of misclassification. Also, the exposure information was not substantiated by detailed occupational history, making it difficult to validate the self-reported exposure assessment. One other limitation is that there was no information on the type of WD that the subjects were exposed to. Most of the subjects were Caucasian, limiting any analysis of the effect of race on this relationship.
In spite of these limitations, our study has a substantial sample size which made it possible to examine the effect of WD exposure among different histological subtypes of UADR cancers and also to compare the degrees of exposure. It is true that many of the cancer patients knew they had cancer at this time. However, the questionnaire was also provided to most of the control subjects at the time of registration before they were evaluated and found to be free of cancer. It is therefore possible that the controls were very similar to the cases in their concern about the disease. A strength of the study design is that all patients were systematically approached at registration. Among the subjects who consented for the study and filled in the questionnaire, about 10% of the cases and 9% of the controls failed to answer the WD exposure question. So, there does not appear to be any difference in response rate for the WD exposure question among the subjects who consented. We also examined the interaction effect of smoking status and the intensity (pack years) of smoking on the relationship between WD exposure and cancer.
Our results consistently show that regular WD exposure was associated with an increased risk of cancers of the lung and squamous cell cancers of the nasal cavity, pharynx and larynx. There was a consistent dose–response relationship associated not only with long term exposure but also with a combination of regular and long term exposure.
CONCLUSION
In spite of the limited exposure information, our results consistently support the hypothesis that regular exposure to WD is associated with an increased risk of cancers of the nasal cavity, pharynx, lung and larynx. The more regular and longer the exposure, the greater is the risk of UADR cancer. However, WD exposure is not associated with risk of developing oesophageal or gastric cardia carcinoma. Smoking possibly acts as a co-carcinogen increasing the carcinogenic effect of WD.
Since UADR cancers constitute 25% of all newly diagnosed cancers, more research is warranted to identify and control the risk factors for these cancers. Given that a sizeable percentage of the worldwide work force has been employed in the wood industry, it is possible that a large number of people have been exposed to WD and are at a greater risk of developing UADR cancers. Future research should aim to clearly establish the carcinogenic dose and type of WD that is related to these cancers. Based on those results, a high risk cohort of wood workers could be identified and screened for early cancer diagnosis and treatment.
REFERENCES
Footnotes
-
Competing interests: None.