Article Text

Abstract
Background: To reduce fatigue-related risk among junior doctors, recent initiatives in Europe and the USA have introduced limits on work hours. However, research in other industries has highlighted that other aspects of work patterns are important in generating fatigue, in addition to total work hours. The Australian Medical Association AMA has proposed a more comprehensive fatigue risk management approach.
Objectives: To evaluate the work patterns of New Zealand junior doctors based on the AMA approach, examining relationships between different aspects of work and fatigue-related outcomes.
Methods: An anonymous questionnaire mailed to all house officers and registrars dealt with demographics, work patterns, sleepiness, fatigue-related clinical errors, and support for coping with work demands. Each participant was assigned a total fatigue risk score combining 10 aspects of work patterns and sleep in the preceding week.
Results: The response rate was 63 1366 questionnaires from doctors working 40 hours a week. On fatigue measures, 30 of participants scored as excessively sleepy Epworth Sleepiness Score >10, 24 reported falling asleep driving home since becoming a doctor, 66 had felt close to falling asleep at the wheel in the past 12 months, and 42 recalled a fatigue-related clinical error in the past 6 months. Night work and schedule instability were independently associated with more fatigue measures than was total hours worked, after controlling for demographic factors, The total risk score was a significant independent risk factor for all fatigue measures, in a dose-dependent manner all p<0.01. Regular access to adequate supervision at work reduced the risk of fatigue on all measures.
Conclusions: To reduce fatigue-related risk among junior doctors, account must be taken of factors in addition to total hours of work and duration of rest breaks. The AMA fatigue risk assessment model offers a useful example of a more comprehensive approach.
- fatigue
- work patterns
- fatigue risk management
- national fatigue survey
- junior doctors
Statistics from Altmetric.com
Hours of work of junior doctors have been the focus of numerous recent articles and editorials in leading medical journals.113 This heightened focus is related to attempts to reduce sleepiness and fatigue among junior doctors by limiting working hours and reducing on-call cover, replacing traditional extended duties with shift work. As of August 2004, doctors working in European Union Member States came under the provisions of the European Working Time Directive, which limits shift durations to 13 hours, followed by a break of at least 11 hours. Maximum weekly work hours had to be reduced to 58 hours in 2004, and to 48 hours by 2009.14 In July 2003, the Accreditation Council of Graduate Medical Education introduced standards restricting the weekly work of residents in all specialties to 80 hours (averaged over a 4-week period), with in-house call limited to 24 hours and no more often than every third night, and a minimum 10-hour rest period between duty periods.15
In New Zealand, the hours of work of junior doctors have been subject to a contractual maximum of 72 hours a week since 1985, with a maximum shift length of 16 hours and breaks of at least 8 hours between shifts.16 In 2002, the average weekly work hours of all active doctors was 47 hours a week, while for doctors aged 24 years or younger, this rose to 59 hours a week.17 Limits on work hours are the traditional approach to managing fatigue-related risk in a number of industries, including medicine.13 18 19
In contrast to these prescriptive approaches, a comprehensive risk management approach is proposed in the Australian Medical Associations National Code of Practice for Hours of Work, Shift Work, and Rostering for Hospital Doctors.20 The Code identifies a range of hazardous aspects of work patterns, provides tools for assessing the risks associated with those hazards, and gives guidance on strategies for reducing them. The Code rests on the joint responsibilities of employers and employees for workplace safety, as embodied in the occupational health and safety legislation in both Australia and New Zealand. Employers must take all practicable steps to provide a safe workplace, including safe systems of work, and consult employees and their representatives on health and safety at work. Employees must report fit for work and cooperate with the employer to provide a safe and healthy workplace.
The present project was designed to document current work schedules of junior doctors in New Zealand public hospitals, and to compare these with the recommendations of the Australian Medical Association (AMA) Code of Practice. The target population included house surgeons (typically in their first 2 years of postgraduate training), senior house officers (typically the third year of postgraduate training in a position designed to lead into specialist training), and registrars (typically specialist training positions).
The project was also designed to examine relationships between the hazardous aspects of work patterns identified in the AMA Code of Practice, and outcomes, including sleepiness and fatigue-related errors, in clinical practice. The Code defines fatigue as tiredness that can result from physical or mental exertion, and it is argued that both lack of sleep and fatigue, individually and in combination, can adversely affect task performance, individual health and safety, and the safety of others. Our working definition is that fatigue is the inability to function at ones optimum level, because physical and mental exertion (of all waking activities, not only work) exceeds existing capacity. Restoration, particularly of cognitive function, requires sufficient good quality sleep. Either definition implies that fatigue is multifaceted. It can be caused by a range of factors including:
-
work duration and intensity (time-on-task fatigue)
-
inadequate recovery sleep, which has cumulative and dose-dependent effects
-
working at inappropriate times in the circadian cycle.
METHODS
The project was approved by the Wellington regional ethics committee (reference 03/02/004). Participation was voluntary and anonymous. Participants had the option to enter a prize draw for a 2-day mystery break for two adults (airfare, meals and accommodation within New Zealand).
A four page questionnaire (available from the corresponding author) was developed. An initial version was piloted in a survey of 192 junior doctors in two local hospitals (50 response rate), as a public health research project by a group of fifth year medical students. On the basis of this project, the questionnaire and survey distribution methods were revised. The revised questionnaire was then completed by a further group of junior doctors in an informal focus group, where their comments and suggestions were elicited. The final questionnaire sought information on demographics and professional activities; work patterns in each of the previous 2 weeks20; sleep habits21 and sleepiness (in daily life in general22 and while driving23); fatigue-related errors in clinical practice24; availability of different types of support, including shift work education, supervision, and access to napping facilities, healthy food, and personal counselling;20 and effects of work patterns on aspects of life outside work.25 Space was also provided for written comments.
Study packages contained a cover letter, a copy of the questionnaire, a work sheet to aid recall of work patterns, and a prepaid return envelope addressed to the Sleep/Wake Research Centre. In August 2003, the Resident Doctors Association (the junior doctors union, the RDA) mailed study packages to all junior doctors (not only its members) nation wide. (When they start employment, junior doctors contact details are forwarded to the RDA so that the Association can mail out invitations to take up membership). This process was used to ensure confidentiality, since the Sleep/Wake Research Centre had no knowledge of names or addresses, and the RDA had no access to completed questionnaires. The only shared information was a unique study ID number for each participant. Non-responders were sent a reminder postcard 3 weeks later, followed by a new study package 4 weeks after the postcard, with all mail-outs conducted through the RDA. Participants were offered the opportunity to have their ID number entered into a prize draw for a commercially available mystery weekend for two people (airfares to a destination disclosed on arrival at the airport, with accommodation and meals).
In December 2003, feedback indicated that some junior doctors had not received study packages, probably as a result of having moved between hospitals. New packages were therefore distributed directly through unit managers responsible for junior doctors in every public hospital (more than 99 of junior doctors work in public hospitals). Participants who had already completed the questionnaire were asked not to respond a second time, but this could not be verified.
The distribution process meant that we could not use the number of packages mailed as the denominator for calculating response rates. We therefore used as the denominator the latest available workforce data from the Medical Council of New Zealand, with whom all medical practitioners must register annually.
All questionnaires were double entered. Statistical analyses were conducted using SAS Version 8.02 (SAS Institute, Inc Cary, NC, USA) and the Statistics Package for Social Sciences (SPSS), version 12.0.1 (SPSS Incorporated Software, Chicago, Illinois, USA).
Each participant was assigned a total risk score according to his/her work patterns in the preceding week, based on the risk assessment guide (page 14) in the AMA Code.20 The only risk factor not included in the present study was the direction of shift rotation, because it is difficult to define in some schedules, particularly where there is on-call work. Table 1 summarises the scoring system (maximum possible score20). For logistic regression analyses, total risk scores were divided into three categories (terciles): lower risk, scores of 06 (37 of participants); significant risk, scores of 79 (31 of participants); and higher risk, scores of 1020 (32 of participants).
Logistic regression analysis was used to identify independent risk factors for excessive sleepiness (Epworth Sleepiness Score (ESS) >10); feeling close to falling asleep at the wheel in the past 12 months; and recalling fatigue-related error(s) in clinical practice in the past 6 months. The independent variables considered were gender; age (in quartiles); ethnicity (Maori, non-Maori New Zealander, or of other ethnicity)26; whether participants had dependents living with them; commute time (115 minutes, 1630 minutes, >30 minutes); how often participants got enough sleep and woke refreshed (never/rarely/sometimes versus often/always); time spent studying a week; house officer or registrar; and in the past fortnight, the number of days worked (10 or >10); hours worked (no excess5070 hours in 1 week and <50 hours in the other, small excess5070 hours in both weeks or >70 hours in 1 week and <50 hours in the other, large excess>70 hours in 1 week and 50 hours in the other); at least two shifts >14 hours in 1 week (yes/no); shifts longer than rostered (none, 15 days, >5 days); worked 24 hours straight (yes/no); days on call (none, <3 a week, 3 in at least 1 week); night duty (1 night a week, 2 in at least 1 week, 3 in at least 1 week); breaks <10 hours (none, 1 a week, >1 in at least 1 week); 24-hour breaks (2 a week, 2 in 1 week and 1 in the other, 1 in both weeks, 0 in at least 1 week); roster changes (none, in 1 week, in both weeks); sleep 23:0007:00 (1 good (6 nights) week and 1 at least medium (45 nights) week, 2 medium weeks, at least 1 bad (3 nights) week); nights with enough sleep (1 good week and 1 at least medium week, 2 medium weeks, at least 1 bad week); adequate supervision at work (never/rarely/sometimes, often/always); education on coping with shift work (yes/no); and access to a bed at work (yes/no).
Each factor with a significant relationship (p<0.05) to a dependent variable was considered for inclusion in the logistic multiple regression models for that variable. For each outcome measure, two logistic multiple regression models were run. The first model included demographic factors and the work-related variables. The second model included demographic factors and the total risk score, which captures the particular combination of work-related factors experienced by each participant. Only participants with complete data for all variables in the model were included (for ESS >10, n1049; for feeling close to falling asleep at the wheel in the past 12 months, n1053; for recalling fatigue-related error(s) in clinical practice in the past 6 months, n1043).
RESULTS
The 1412 questionnaires returned represent a 66 response rate (denominator based on the 2002 Medical Council Workforce Survey17). Excluding respondents who did not work at least 40 hours a week and primarily in public hospitals, the final analytical data set included 1366 junior doctors (63 response rate) whose average (SD) age was 30.7 (5.8) years. Women were slightly over-represented compared with the 2002 Medical Council workforce survey (49 vs 43, respectively: 211.9, p<0.001). The respondents were 26 house surgeons, 14 senior house officers, and 61 registrars. The distribution of specialties was representative of the workforce as a whole, except for an over-representation of registrars who indicated that their current clinical discipline or run was in intensive care. This may be because registrars from several vocational training programmes spent part of their training time in intensive care.
The total number of hours worked in each week was recorded in three categories: <50 hours (lower risk), 5070 hours (significant risk), or >70 hours (higher risk).20 Figure 1 shows the distribution of participants in these categories across the 2 study weeks. Overall, 13 of the reported working weeks exceeded 70 hours.
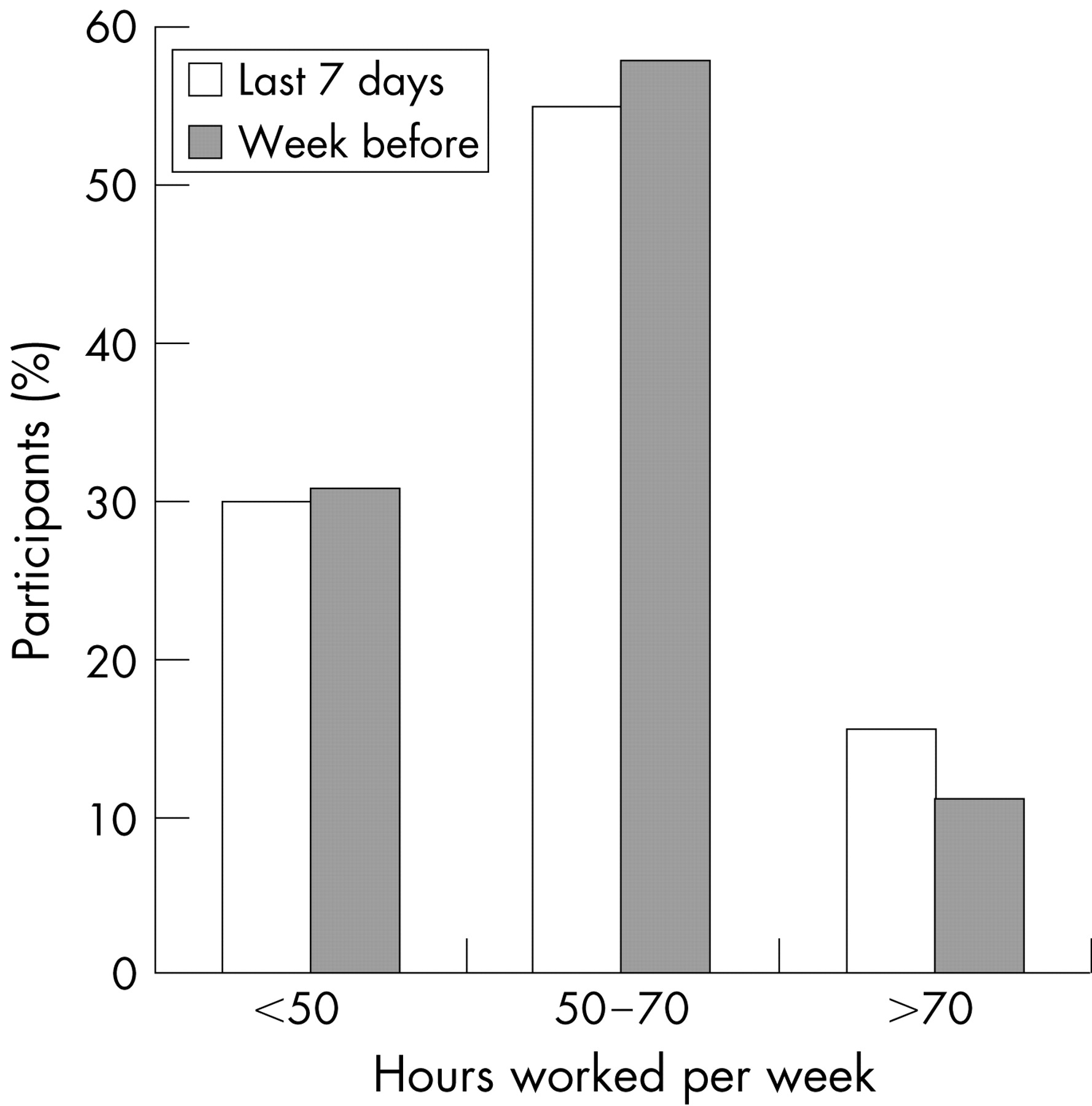
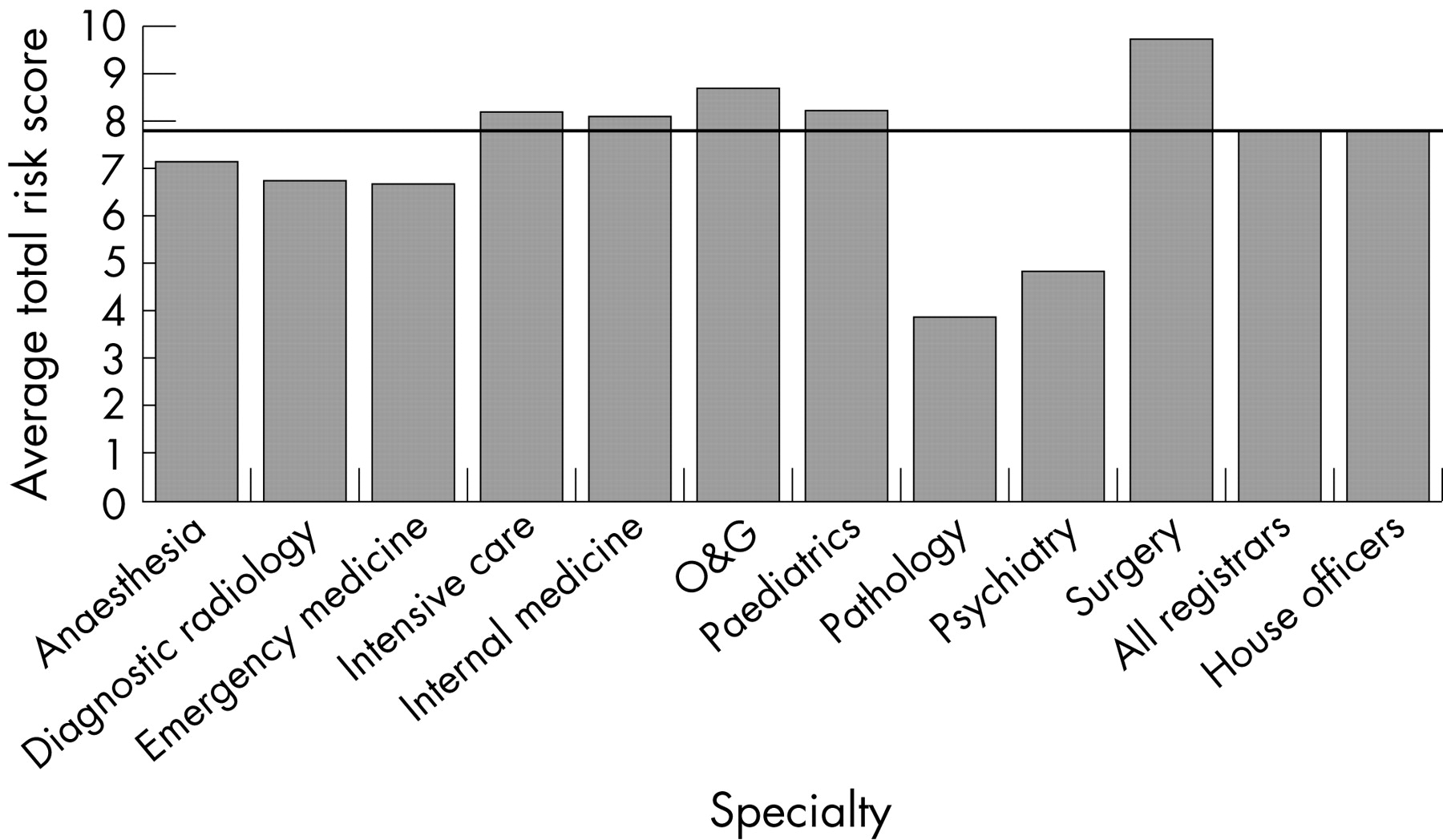
Figure 2 depicts the average total risk score for each specialty group, based on their work patterns in the preceding week. To protect confidentiality, only those specialties represented by at least 20 participants were included in this breakdown.

{kind=link}
{kind=link}
The mean (SD) ESS was 8.2 (4.2), and 30 of participants scored as excessively sleepy (ESS >10). Of these, 5 scored as having a severe sleepiness problem (ESS 16). About a quarter (24) indicated that, since becoming a doctor, they had fallen asleep driving home from work. Two-thirds (66) had felt close to falling asleep at the wheel in the past 12 months and 21 indicated that this had happened at least five times. Two-thirds of participants (66) could recall having made a clinical error owing to fatigue at some time in their careers, and 42 could recall having made a fatigue-related clinical error in the past 6 months. Error reporting rates in the past 6 months, broken down by specialty, were as follows: anaesthesia 46; diagnostic radiology 37; emergency medicine 57; intensive care 38; internal medicine 41; obstetrics and gynaecology 28; paediatrics 35; pathology 27; psychiatry 23; surgery 32; all registrars 36, all house officers 50.
Table 2 summarises the significant independent risk factors for reporting excessive sleepiness, feeling close to falling asleep at the wheel in the past 12 months, and recalling a fatigue-related clinical error in the past 6 months, as identified by the logistic multiple regression analyses.
For each dependent variable, two separate models were run that included the same demographic variables and either the work pattern variables or the total risk score. For the demographic variables, there were minor differences in the odds ratios between the two models, but no changes in the significance of the relationships.
The independent odds ratios (iORs) in Table 2 suggest a dose-dependent relationship between the total risk score and each of the outcome measures. This trend was confirmed in additional logistic multiple regression models that included the same demographic factors and total risk score as a continuous variable (for ESS >10, iOR1.76, 95 CI 1.48 to 2.10, p<0.001; for feeling sleepy at the wheel in the past 12 months, iOR1.53, 95 CI 1.29 to 1.81, p<0.001; for recalling a fatigue-related clinical error in the past 6 months, iOR1.36, 95 CI 1.16 to 1.59, p0.001). This trend is also evident in the unadjusted comparisons across the terciles of the total risk score (table 3).
DISCUSSION
By international standards, the weekly work hours of these junior doctors were relatively moderate, with only 13 of documented working weeks exceeding 70 hours. Nevertheless, only 30 of documented working weeks were less than 50 hours (approaching the EU Working Time Directive limit of 48 hours14), and the outcome measures suggest that fatigue-related risks remain a concern.
Participants were twice as likely as the general adult population to score as excessively sleepy on the ESS (30 vs 15 of a representative sample of New Zealanders aged 3059 years26). Since becoming doctors, 24 of participants recalled falling asleep at the wheel while driving home from work, compared with 31 of doctors at a UK district general hospital who drove home after night call.27 Compared with a structured random sample of 4621 British male car drivers (mean age 48 years, 51 response rate),23 participants were more than twice as likely to report feeling close to falling asleep at the wheel in the past 12 months (66 vs 29).
Participants were more likely to recall a fatigue-related clinical error in the past 6 months (42) than a representative sample of all anaesthetists practising in New Zealand (32; respondents were 19 trainees and 81 specialists).24 The latter survey indicated that the perception of what constitutes an error may alter as doctors become more experienced. In both the present survey and the anaesthetists survey, the question asked was In the past 6 months, have you made an error in clinical practice that you consider was due to fatigue?. No definition of error was provided and the proportion of errors with the potential to harm patients is unknown. The relationship between work patterns and error is likely to vary by specialty, and merits more detailed investigation.
Working excessive hours in the past 2 weeks was an independent risk factor for one outcome measure: excessive sleepiness (ESS >10). Having schedule changes in both weeks (compared with no schedule changes) was a significant independent risk factor for two outcome measures: excessive sleepiness, and having felt sleepy at the wheel in the past year. Night work (3 nights in one or both weeks, compared with 1 night in either week) was a significant independent risk factor for all three outcome measures: excessive sleepiness, having felt sleepy at the wheel in the past year, and recalling a fatigue-related clinical error in the previous 6 months. Moving up a tercile in the total risk score (which combines 10 aspects of work and sleep patterns in the past week) independently increased the risk of all outcome measures, in a dose-dependent manner. On the other hand, having adequate supervision at work often or always (compared with never, rarely, or sometimes) independently reduced the risk of all outcome measures.
Main messages
-
In a national survey of junior doctors working 40 hours a week, night work and roster instability (but not total weekly work hours or short breaks between shifts) were independently associated with reporting fatigue-related clinical errors and sleepiness while driving.
-
Regular access to adequate supervision moderated the perceived impact of work patterns, and may therefore represent a useful fatigue countermeasure.
-
To reduce fatigue-related risk among junior doctors, account must be taken of factors in addition to total hours of work and duration of rest breaks.
The response rate (66) and the extent to which study participants were representative of the entire workforce were assessed relative to the 2002 Medical Council workforce survey data (the latest dataset available). However, the present survey was conducted between August 2003 and February 2004. From 2002 to 2003, the total number of medical practitioners increased by 4.6. If a similar increase in the number of junior doctors meeting the study inclusion criteria is assumed, the estimated response rate for the study would reduce to 63. Regarding the possible direction of response bias, several participants commented that junior doctors with the most demanding work patterns would not have the time or energy to fill in the survey. On the other hand, it might be argued that those who wished to complain, or who experienced greater difficulty coping with their work patterns, would be more likely to complete the questionnaire.
Women were over-represented compared with the 2002 Medical Council workforce survey (49 vs 43). This may have inflated the combined estimates of the prevalence of excessive sleepiness (reported by 32 of women and 27 of men, p (2)<0.05), and having felt close to falling asleep at the wheel in the past 12 months (reported by 70 of women and 64 of men, p (2)<0.05).
Policy implications
The traditional regulatory approach to reducing fatigue among junior doctorsnamely, limiting work hours and minimum breaks between shifts, ignores key aspects of work patterns that affect fatigue, including night work and roster predictability.
An important limitation is that all information is retrospective and subjective. To aid accurate recall of work patterns, the study package included a work sheet designed to enable participants to reconstruct their work patterns over the preceding 2 weeks. Nevertheless, the possibility cannot be excluded that there might have been some tendency to over-report extreme eventsthat is, memorable events that actually occurred before the study time frame might have been unconsciously brought into the reporting frame. Some confusion may also have been engendered by the different time frames referred to in the questions on outcomes (likelihood of dozing in recent times, fatigue-related errors in the past 6 months, having felt sleepy at the wheel in the past year). The questions dealing with outcomes were standard questions chosen to enable comparisons with data collected in previous national surveys, and the likelihood of these events occurring in a 2 week period is extremely low. On the other hand, the 2 week time frame for analysis of duty periods was based on the AMA Code of Practice, and the reliability of retrospective recall of work patterns over a longer time frame was a concern. Ideally, both sets of measures would be collected simultaneously and prospectively across an extended period of time. The work patterns of registrars are fairly stable once they are in a training programme, but the house officers undergo rotations about every three months, and their work patterns can change considerably from one run to the next. Because of these limitations, the significant odds ratios reflect relationships between recent work schedules and participants general perceptions about their sleepiness and fatigue-related clinical errors.
A cross-sectional study such as this provides limited evidence that relationships between work-related factors and outcomes are causal. However, based on sleep restriction studies, it is expected that aspects of work patterns that restrict sleep will cause increased sleepiness and degraded performance and mood.2832
There is no definitive risk matrix for this type of assessment, and the matrix used is only one possible example based on the Risk Assessment Guide developed by the AMA.20 It is acknowledged that the factors included in the total risk score, and the precise definitions of risk categories (lower, significant, higher) are somewhat arbitrary, although the dose-dependent relationships between the total risk score and the outcome measures suggest that it captures important aspects of the work patterns. Different aspects of the work patterns are weighted equally when calculating the total risk score, and workload is not explicitly considered. A more rigorous approach would be to undertake detailed risk assessments for different groups of junior doctors, particularly since work patterns differ by specialty. Using the present matrix, detailed analyses have been undertaken to identify which aspects of the work patterns make the greatest contribution to fatigue risk scores in each specialty. These analyses are reported elsewhere.32 Uptake of the Code in Australian hospitals has been limited.
We conclude that long work hours are not the only aspect of work patterns that needs to be managed to reduce sleepiness and fatigue-related clinical errors among junior doctors. Other aspects of work schedules captured in the total risk score in this study had consistent, dose-dependent relationships to reports of sleepiness and fatigue-related clinical errors, after controlling for a range of demographic variables. Interestingly, regular access to adequate supervision moderated the perceived impact of work patterns, and may therefore represent a useful fatigue countermeasure. The findings support the view that a more comprehensive risk management approach is needed to reduce doctors sleepiness and improve patient safety.4 13 19 20 33 34
Acknowledgments
We are indebted to the participants for their time and commitment in completing questionnaires and providing written commentary. Margo van den Berg and Erich Janssen (formerly of the AMA) had important input to the early stages of this project. Invaluable support was provided by the staff at the Resident Doctors Association, Te Ohu Rata o Aotearoa, the Medical Council of New Zealand, and Resident Medical Officer Unit Managers nation wide.
REFERENCES
Footnotes
-
Funding: This project was funded by the Health Research Council of New Zealand, project grant 02/249. The Medical Assurance Society provided the incentive prize.
-
Competing interests. None to declare.
- Abbreviations:
- AMA
- Australian Medical Association
- ESS
- Epworth Sleepiness Score
- iOR
- independent odds ratio
- RDA
- Resident Doctors Association