Article Text

Abstract
Aims: Because logistical and financial obstacles impede using large prospective cohort studies, surveillance decisions in occupational settings must often be made without evidence of relative benefits and costs. Using the example of isocyanate induced asthma, the most commonly reported immune mediated occupational asthma, the authors developed a model based approach to evaluate the costs and benefits of surveillance from both an employer and a societal perspective.
Methods: The authors used a mathematical simulation model of isocyanate asthma to compare annual surveillance to passive case finding. Outcome measures included symptom free days (SFD), quality adjusted life years (QALY), direct costs, productivity losses, and incremental cost effectiveness ratio (CER), measured from the employer and the societal perspectives. Input data were obtained from a variety of published sources.
Results: For 100 000 exposed workers, surveillance resulted in 683 fewer cases of disability over 10 years. Surveillance conferred benefits at an incremental cost of $24,000/QALY (employer perspective; $13.33/SFD) and was cost saving from the societal perspective. Results were sensitive to assumptions about sensitisation rate, removal rates, and time to diagnosis, but not to assumptions about therapy costs and disability rates.
Conclusions: Baseline results placed the CER for surveillance for isocyanate asthma within the acceptable range. Costs from the societal and employer perspective differed substantially with a more attractive CER from the societal perspective, suggesting opportunities for employer/societal cost sharing. The analysis demonstrates the value of a model based approach to evaluate the cost effectiveness of surveillance programmes for isocyanate asthma, and to inform shared decision making among clinicians, patients, employers, and society. Such a modeling approach may be applicable to surveillance programmes for other work related conditions.
- CER, cost effectiveness ratio
- QALY, quality adjusted life year
- SFD, symptom free day
- occupational diseases
- screening
- diisocyanates
- asthma
- cost-benefit analysis
Statistics from Altmetric.com
This paper proposes the use of a mathematical simulation model to inform medical decision making and resource allocation for the prevention of isocyanate induced asthma. We believe that this unorthodox approach to clinical programme evaluation is justified by several considerations. Firstly, isocyanate asthma imposes an important health and economic burden on workers, employers, and society. Isocyanate asthma is the most commonly reported cause of immune mediated, occupational asthma1 and frequently persists even after removal from exposure, leading to a disproportionate amount of disability.2
Secondly, although numerous authors recommend surveillance for occupational asthma,3–5 there are limited data on the effectiveness of surveillance or its costs. The case for surveillance is typically founded upon the observation that prolonged exposure correlates with poor clinical outcomes, which in turn makes it likely that early removal from exposure would improve prognosis.6,7,8,9,10,11,12 Retrospective studies using Canadian workers’ compensation data have demonstrated earlier diagnosis, better recovery, and reduced disability among workers who participate in surveillance programmes compared with those who do not.10,13,14 However, it is unclear whether these benefits are attributable to medical surveillance or other factors such as improved industrial hygiene measures or increased awareness of the hazards of isocyanates. Furthermore, none of these studies takes into account the costs of surveillance. Without data on relative benefits and costs, it is difficult to make policy decisions about allocating limited funds, or about how costs should be shared between employers and society.
Thirdly, it is unlikely that direct evidence of the benefits and costs of surveillance will be available in the foreseeable future. In order to demonstrate the effectiveness of surveillance, large, prospective, inception cohort studies would be needed, ideally with a “control arm” without surveillance. There are tremendous practical, ethical, and financial obstacles to mounting such studies.
Model based evaluations have been used successfully to address comparable questions and to guide policy decisions regarding other diseases for which direct data are insufficient,15,16 and cost effectiveness ratios for other commonly used screening programmes are available for comparison.17 We are not aware of similar approaches to address screening or surveillance for work related conditions. Simulation models have two important advantages. Sensitivity analysis can identify those parameters that most influence the effectiveness and costs of different strategies. In addition, modeling can explore the impact of cost allocation. This is of particular relevance to work related conditions, where the employer frequently covers the cost of surveillance, while the benefits extend beyond the employer and may include improved employee health, maintenance of breadwinner income for families, and reduced strain on government health and welfare programmes.
METHODS
Overview
We developed a mathematical simulation model to estimate clinical outcomes and costs of isocyanate asthma in a population of 100 000 otherwise healthy, exposed workers aged 18–65 years. We compared two clinical strategies:
-
Passive case finding, where workers are only diagnosed with occupational asthma if they present to a healthcare provider with symptoms and their asthmatic condition is attributed to workplace exposure.
-
Surveillance, in which workers undergo yearly screening using a symptom questionnaire and spirometry.
In keeping with accepted methods for cost effectiveness analysis, we measured value for money in terms of both dollar per quality adjusted life year (QALY) gained15 and dollars per symptom free day (SFD) gained, and discounted all outcomes at 3%/year.16 Monetary values are reported in 2002 US dollars, adjusted (where necessary) using the medical care component of the consumer price index.19 We compared cost effectiveness ratios from two perspectives. The employer perspective included direct and indirect medical costs as well as disability costs. For the societal perspective, we also included the cost of lost wages.
Model structure
We employed a state-transition framework wherein the progress of disease was characterised as a sequence of transitions through a defined set of health states (Markov model, executed in Excel, see Glossary). At any given time, a patient is assigned to a single health state, such as “healthy, exposed”, “symptomatic”, or “disabled”. It is assumed that patients in a particular state resemble each other with regard to their prognosis and healthcare use. Rates of disease progression and clinical events are captured by assigning probabilities to the monthly transitions between states.
In our model, workers could transition into a different health state each month. Exposed workers could become sensitised to diisocyanates and progress through an acute, more reversible state into a less reversible disease state. If workers were removed from exposure, they could return into an asymptomatic state. If they were not removed from exposure, they could progress into a more chronic state and could eventually become disabled. Diagnosis could modify disease progression by expediting removal from exposure. Health states were further distinguished from one another on a number of dimensions: exposure, symptoms, diagnosis, reversibility of disease, ability to work, and vital status. By running the model for an extended period without surveillance, we estimated the following initial distribution of workers to health states: 93% asymptomatic, 6% symptomatic but undiagnosed, with the remaining 1% symptomatic and diagnosed and in the process of being removed.
Input parameters
To estimate the efficacy and costs of surveillance for isocyanate asthma, we conducted a Medline search using the search terms “occupational diseases”, “asthma”, “toluene 2,4 diisocyanate”, “diisocyanates”, and “isocyanates”. A hand search of the identified articles yielded further references. We identified 107 articles published between 1985 and 2003. The input data varied considerably in exposure setting, type of isocyanate, healthcare system, political and economic setting, and type and extent of data reported. For many input parameters, there was a large range of uncertainty and variability regarding the best estimate. However, models require the selection of an initial point estimate as well as an estimate of the potential ranges for sensitivity analysis. Most studies focused on European and Canadian populations, and did not provide sufficient data on all parameters necessary for the model. We therefore supplemented our dataset by asking a panel of three experts (one of the authors (CR), another physician board certified in occupational medicine, and one industrial hygienist) to provide estimates, ranges, and baseline values for selected parameters. Parameters for which we had to use expert estimates include the time of progression to a less reversible state and the disability rates for workers not removed from exposure (table 1). For parameters for which we had no data on the range such as diagnostic test costs, we chose a range of 50–200% of the point estimate.
Input parameters for model (parameters that were estimated by expert panel are in italics)
Sensitisation
Studies on the incidence of isocyanate asthma are fraught with problems of subject attrition, healthy worker effect, the lack of a simple highly reliable test to diagnose isocyanate asthma,20 and cross sectional design. The few prospective longitudinal studies that have been conducted have focused primarily on workers exposed to toluene diisocyanates in large production plants, reporting low sensitisation rates around 1%/year.21 In such settings, exposure is typically better controlled (and therefore incidence lower) than in the end use of numerous isocyanate-containing polyurethane products such as paints, coatings, and foams. The commonly cited prevalence rates of isocyanate asthma between 5% and 10% are typically based on data from cross sectional studies or production facilities. However, in end users, much higher sensitisation rates of up to 18% in 18 months have been described.22 For some small end users such as spray shops, sensitisation rates as high as 30% have been described.23,38–40 We used a constant sensitisation rate of 2.8%/year based on data from wood product workers exposed to methylene diphenyl diisocyanates.23 We performed extensive sensitivity analysis on the sensitisation rate within the published range of 0.7–4.5%/year to evaluate the impact of different assumptions about the sensitisation rate on the cost effectiveness ratio.
Surveillance and diagnosis
The surveillance intervention was assumed to consist of a questionnaire and spirometry,24 conducted yearly. Diagnostic confirmation included an interview with a physician trained in occupational and environmental medicine, peak flow meter monitoring, spirometry, a chest x ray, and, in 50% of cases, a methacholine challenge test to confirm a diagnosis of asthma. Unfortunately, there is currently no highly sensitive/specific immunological or other feasible assay to diagnose isocyanate asthma, and specific inhalation challenge testing is not routinely available in many countries.25 Time to diagnosis with and without surveillance was estimated from a study of surveillance programmes for Canadian workers.10Diagnosis costs: surveillance and diagnosis costs were calculated based on charges from the Yale Occupational and Environmental Medicine Practice, adjusted for the hospital’s cost:charge ratio.26
Disease progression, recovery, removal from exposure, disability
These input parameters were based on European data.7,12 Removal probabilities of undiagnosed workers were assumed to be similar to those of patients with non-occupational asthma. For disability rates, workers who were still exposed were presumed to be twice as likely as removed workers to become disabled (expert panel). We estimated a two year progression time from the acute, more reversible state to the less reversible health state with ongoing exposure (expert panel).
Lost productivity
As a first approximation of productivity costs, we estimated lost wages due to removal from workplace exposure. We combined income estimates from workers exposed to diisocyanates ($50,000/year)27 with Italian data describing a 28% decrease in wages for workers who are removed from exposure.28 We further assumed that the decrease in wages would remain constant over time in order to estimate the net present value of lost income over 10 years.
Medical and absenteeism costs
Disease severity specific costs for isocyanate asthma are not reported in the literature. We developed a method to allocate data on US employer costs from employees with non-occupational asthma29 to patients in the two severity levels described in our model. In brief, we assumed that costs for workers in the irreversible, chronic stage were twice those of the average asthmatic employee. Following a study of Italian workers with occupational asthma, we estimated the monthly healthcare use of a worker who is symptomatic but removed from exposure at 56% of the costs of an exposed worker.28
Outcomes
The model predicts symptom days as well as number of disability cases. In order to calculate incremental cost effectiveness ratios, these clinical outcomes are by convention translated into utility outcomes.16 The US Panel on Cost-effectiveness in Health and Medicine recommends the use of community preferences for health states to value morbidity consequences, wherever feasible.16 However, no studies have considered a sufficiently rich set of symptomatic health states to be suitable for our use. The most frequently used utility outcome in cost effectiveness studies overall is the QALY; however, the SFD has been advocated as an appropriate measure for studies in asthma due to the episodic nature of asthma symptoms.28 Neither of these outcome measures has been described for occupational asthma. In order to make our results potentially more relevant to occupational illnesses, we used an additional outcome measure, the cost per case of disability prevented.
Estimate of SFD for each state
We estimated SFD for the different health states by converting data on weekly symptom frequency scores.7,28 We assumed that the actual frequency of symptom days followed a Power distribution.31 Using commercially available software (Microsoft Excel 1998), we used data from Pisati et al7 to estimate SFD for the states “well and exposed”, “symptomatic, diagnosed, exposed”, and “chronic, undiagosed, not removed”. SFDs for other states were estimated by interpolation. SFDs were converted to QALYs using a conversion formula of 1 QALY = 1800 SFDs gained.30
Sensitivity analysis
In conformity with the recommendations of the US Panel on Cost-effectiveness in Health and Medicine,15 sensitivity analyses were performed on all input parameters over the plausible/estimated range. In order to take into account the range of existing medical costs, costs were varied between 50% and 200% of their baseline values. We varied time to diagnosis as a proxy measure for the accuracy of the screening/diagnostic tests.
RESULTS
Reference case analysis
For 100 000 workers over 10 years and compared with passive case finding, surveillance conferred a benefit over passive case finding of 683 fewer disabled workers, 3.3 million more SFDs, and 1831 additional QALYs at an additional cost of $44 million. About half of the additional costs of surveillance and confirmation ($82 million) were offset by a reduction in medication, absenteeism, and disability costs. Most of the costs for both clinical strategies were related to disability.
We estimated an incremental cost effectiveness of $24,000/QALY ($13.33/SFD; $64,000/case of disability prevented) for surveillance from the employer perspective. Surveillance was cost saving from the societal perspective, which included lost wages (by convention, no CER is reported for cost saving interventions, see Glossary).
Sensitivity analysis
To explore the impact of uncertainty in our input parameters, we conducted a number of one way sensitivity analyses, presented in figures 1–3.

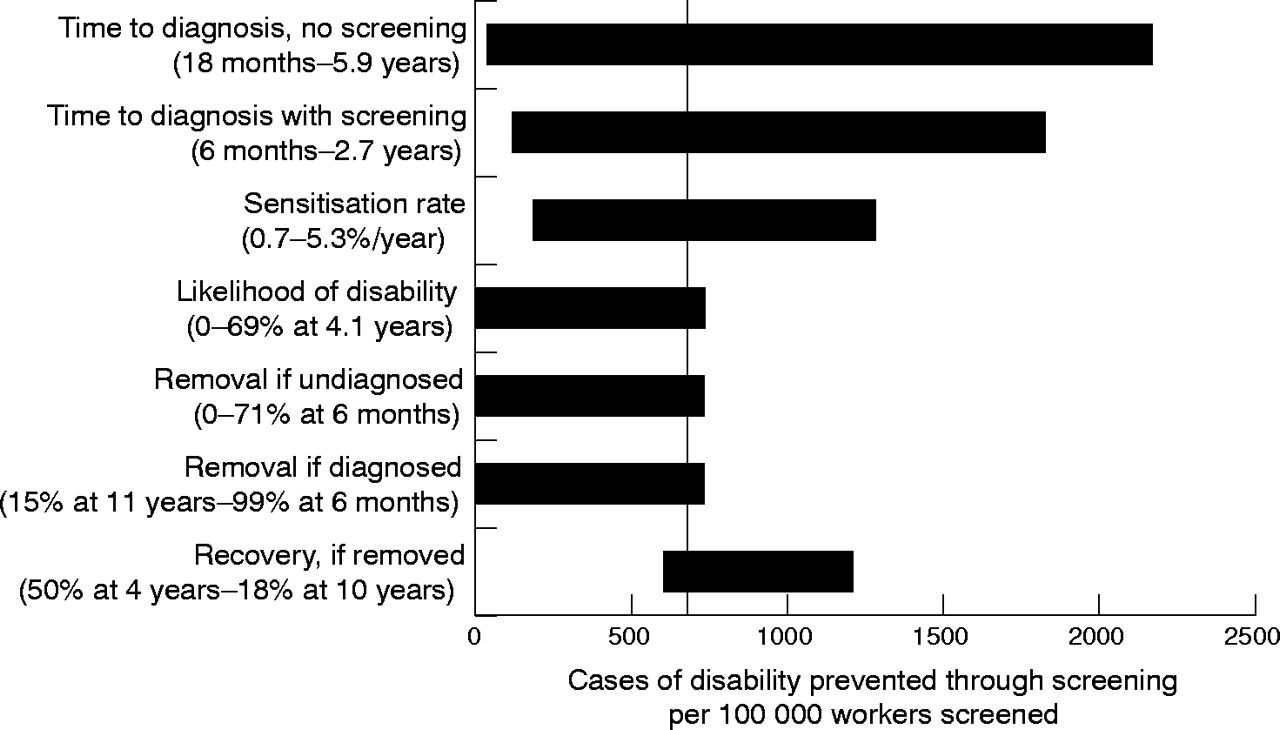
Overview of sensitivity analysis for cases of disability. This “Tornado” diagram summarises a series of one way sensitivity analyses. Each bar represents a model parameter. The vertical axis sits at the base case incremental cost effectiveness estimate (683 cases of disability prevented). The width of a horizontal bar denotes the range of cost effectiveness outcomes produced by varying that parameter over its plausible range.
Figure 1 summarises the effect of changing input parameters on the number of disability cases. The width of the bar corresponds to the magnitude of change in disability cases prevented through surveillance. Surveillance was especially beneficial in settings in which there is a high incidence of isocyanate asthma (that is, a high sensitisation rate), in which there is a high likelihood that workers will become disabled, where workers are removed fast from exposure once they are diagnosed, and where surveillance substantially expedites diagnosis compared to detection through passive case finding. Variations in the input parameters can change the difference in disability cases between the two strategies from close to 0 to as high as 2500.
Figure 2 summarises the effect of varying individual input parameters on the incremental CER from the employer perspective. Our results were very sensitive to assumptions about the time to diagnosis with and without surveillance, the sensitisation rate, and removal times with and without diagnosis. Varying these assumptions can push the CER well beyond the commonly cited threshold of $50,000/QALY and thereby change our policy conclusion that surveillance is a cost effective intervention. However, varying the estimates regarding surveillance costs, confirmation costs, disease progression, and disability rates would have less impact on the CER and would not increase it beyond the commonly cited threshold.
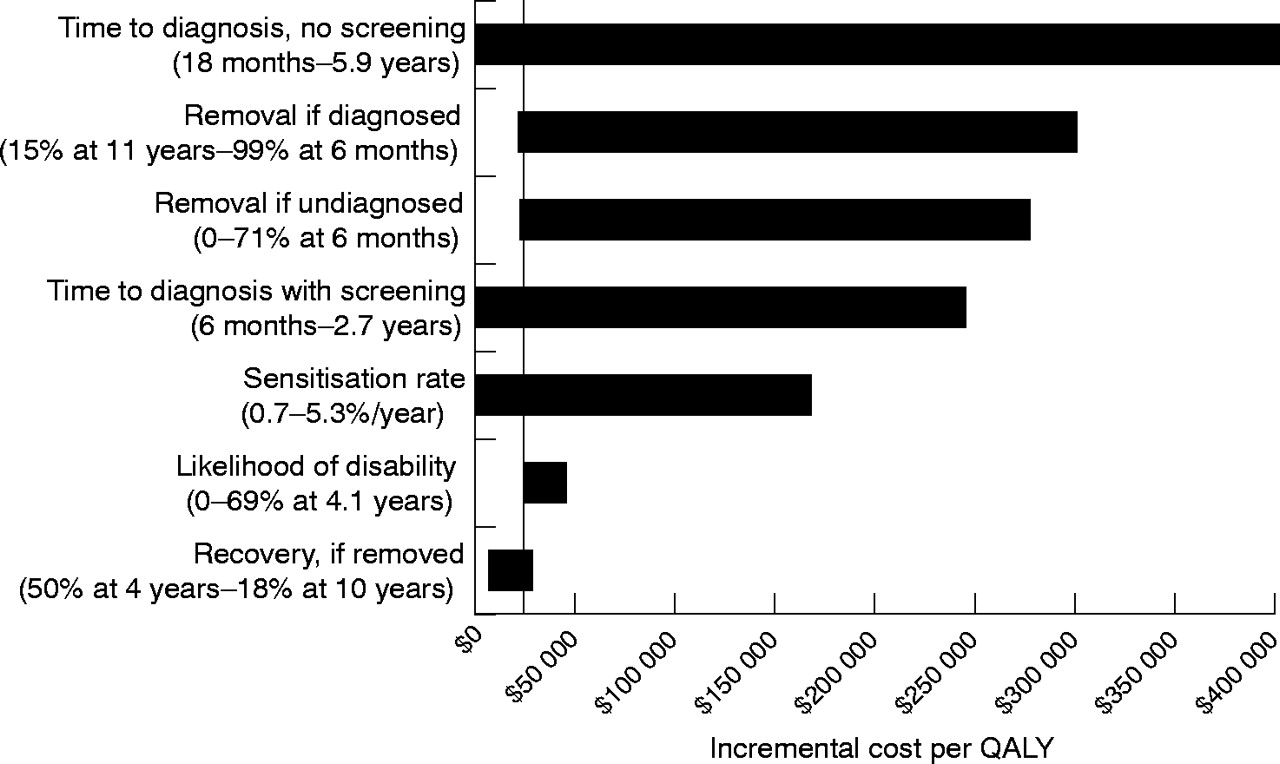
Overview of sensitivity analysis for $/QALY (employer perspective). This is again depicted as a Tornado diagram with horizontal bars representing model parameters and the width of the bar denoting the range of cost effectiveness outcomes produced by varying that parameter over its plausible range. The y axis intersects the x axis at the base case cost effectiveness ratio ($24,000/QALY).
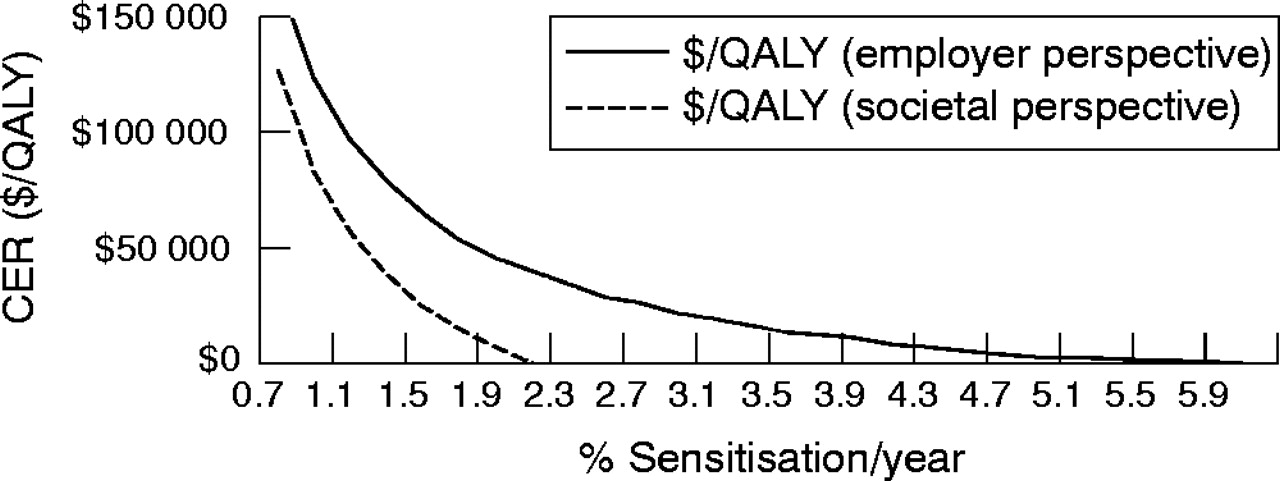
Figure 3 illustrates the results of a one way sensitivity analysis of the sensitisation rate from both the employer and the societal perspective. At a sensitisation rate of 0.7%/year, surveillance has an unattractive CER beyond $50,000/QALY from both the employer and the societal perspective and would not be considered cost effective. As the assumed sensitisation rate increases, the CER for surveillance becomes more and more attractive. From the employer perspective, surveillance crosses the commonly cited threshold of $50,000/QALY if the sensitisation rate is assumed to be around 1.9%/year; surveillance becomes cost saving only at higher sensitisation rates above 5.3%/year (as would be likely in the first two years of employment). From a societal perspective, surveillance has an attractive CER below $50,000/year with sensitisation rates above 1.1%/year and becomes cost saving at sensitisation rates around 2.1%/year.

{kind=link}
{kind=link}
{kind=link}
One way sensitivity analysis of the sensitisation rate from the employer and societal perspective (CER<0 equals cost saving).
DISCUSSION
Surveillance decisions in occupational disease must often be made in the absence of a firm evidence base, as logistical, ethical, and financial obstacles greatly impede the use of large, prospective, randomised inception cohort studies that could provide more definitive data regarding the effectiveness of screening programmes. Using the example of isocyanate induced asthma—the most commonly reported cause of immune mediated occupational asthma—we aimed to demonstrate the value of a model based approach to estimate the benefits and costs of surveillance, as well as examine the impact of current cost allocation.
Using a state-transition model with input parameters within the published range, surveillance resulted in decreased numbers of disabled workers and decreased days with symptoms. Although surveillance increased net overall costs from the employer perspective, it was cost saving once the societal costs of lost productivity were included.
We estimated an incremental CER of $24,000/QALY ($13.33/SFD and $64,000/case of disability prevented) when evaluated from the employer perspective. Our results compare favourably to cost effectiveness findings in a range of secondary prevention interventions17 and are below the CERs of other commonly recommended surveillance tools (including mammography for breast cancer,33 flexible sigmoidoscopy for colon cancer,34 and fasting plasma glucose for diabetes mellitus35). Although voluntary and mandated surveillance programmes exist for workers exposed to a number of different hazards, we are not aware of any published CERs related to these. One could argue that different and higher cost effectiveness thresholds should apply for occupational diseases, because these diseases would not occur without work related exposure. With higher cost effectiveness thresholds, screening for isocyanate asthma would be cost effective even under very conservative assumptions.
We found large differences in the CER comparing the employer and societal perspectives, with a more attractive CER from the societal perspective. The issue of perspective is particularly critical for work related diseases, where surveillance typically occurs only if an employer is willing to implement and finance it, or in those instances in which surveillance is mandated by law. Our finding that surveillance for isocyanate asthma is cost saving from the societal perspective but not from the employer perspective is important in designing and implementing effective preventive strategies for work related diseases. Such findings, which may be applicable to other work related conditions, suggest why employers sometimes have little financial incentive to implement effective surveillance strategies, even if society benefits greatly from preventing cases of chronic disease and disability. Our model provides a framework for exploring alternative cost sharing arrangements and highlights why mandatory regulatory surveillance may be the most effective way to implement screening for certain occupational diseases.
Our sensitivity analysis was very helpful in identifying those parameters which most influence the efficacy and costs of surveillance for isocyanate asthma, most importantly sensitisation rate, likelihood of diagnosis and removal without surveillance, and accuracy of diagnostic test. In contrast, changes in surveillance, diagnosis costs, or test costs did not significantly change our estimated CER. Identification of high impact parameters can focus further research on the cost effectiveness of surveillance for isocyanate asthma, as well as identify those settings in which surveillance will be most cost effective. For example, our sensitivity analysis demonstrates the large impact of baseline detection rates (detection without screening) of isocyanate asthma on the number of disability cases prevented. Our baseline detection rates of 2.7 years to diagnosis without screening versus 1.7 years to diagnosis with screening were based on a Canadian study because of the lack of any such US data. However, in the US, the diagnosis of occupational asthma is typically long delayed36,37 and often never made.37 Therefore, our baseline time of 2.7 years to diagnosis of isocyanate asthma without surveillance is likely a substantial underestimate of the true time in the US and other countries. As demonstrated by the sensitivity analysis, a less conservative and more realistic time to diagnosis would result in a substantially greater reduction in the number of disabled workers with screening and a more favourable cost effectiveness ratio.
An especially important issue and one of the key drivers of our results is the sensitisation or incidence rate. Despite a more extensive literature than for most other agents that cause occupational asthma, there remains substantial variability and uncertainty regarding the incidence and prevalence rates of isocyanate asthma. Reported rates vary greatly, depending on various factors including the specific isocyanate and process, extent and route of exposure, industry, healthy worker effect, and study design, with most studies reporting prevalence rather than incidence rates. In addition, the majority of workers probably develop isocyanate asthma within the first one to two years of exposure.2 Our sensitivity analysis enables us to examine the impact of varying the sensitisation rate on the cost effectiveness ratio and the number of disability cases. Our reference case was based on a sensitisation rate of 2.8%/year. Over 10 years, this would result in a prevalence of isocyanate induced asthma around 25%. Prevalence rates as high as 30% have been described in the literature, mainly for small end users (such as spraying and coating operations),38–40 with lower rates in production facilities.21 Our sensitivity analysis suggests that in settings of sensitisation rates below 1%/year, surveillance may not confer sufficient incremental value to justify the cost. Furthermore, most studies suggest high sensitisation rates within the first two years with lower subsequent sensitisation rates. Using a constant sensitisation rate therefore inflates the apparent value of surveillance. Again, sensitivity analysis permits us to explore at which sensitisation rate the CER of surveillance exceeds commonly used thresholds. Further study of variable surveillance frequency and shorter surveillance times is possible with adaptations of the model and is an important next step in further analysis.
Main messages
-
Model based analysis may provide a valuable tool for evaluating the cost effectiveness of surveillance programmes for occupational diseases.
-
Yearly screening for isocyanate asthma has an attractive cost effectiveness ratio and compares favourably to other frequently recommended surveillance tools.
-
Sensitivity analysis identifies those parameters that most influence the cost effectiveness of surveillance for isoycanate asthma.
-
The cost effectiveness ratio of screening for isocyanate asthma was more favourable from the societal than from the employer perspective, which has important implications regarding cost sharing.
Our study has several limitations. First among these is the paucity of clinical and economic data upon which to base the input parameters. Furthermore, we have assembled clinical data from a variety of sources, reflecting not only varying quality and individual design limitations, but—even more importantly—different worker populations, workplace systems, and national health systems. For all these input parameters, we attempted to identify the best estimate for each parameter through a careful review of the literature and consultation with an expert panel. We therefore urge caution in using the point estimate for the CER we found without taking the results of the sensitivity analysis into account. The potential inaccuracy of the input parameters is an important limitation, it also highlights a potential strength of our analysis. The sensitivity analysis performed over a greater range of potential input parameters identifies those critical variables (such as sensitisation rate) whose uncertainty could result in a policy reversal as well as those that are not central to the decision at hand.
Further limitations are created by simplifications used to build the model. Examples are the use of a linear relation between sensitisation and disease development or the necessary simplification of asthma disease progression into two states. Furthermore, we were not able to separately adjust our model for false negatives and positives tests, nor could we base our model on a definitive, readily available diagnostic test for isocyanate asthma. However, we accounted partially for imperfect test characteristics through the use of a time to diagnosis which is longer than the surveillance interval. Improved surveillance and/or readily available definitive diagnostic tests for isocyanate asthma, an active area of research, would likely further improve the CER of surveillance. Although it would have been possible to avoid some of the simplifications through adding additional states to the model, it is not clear that sufficiently accurate data exist to support such a refinement. Another limitation inherent in the model is the challenge common to all cost effectiveness analyses on asthma: how best to translate SFDs into QALYs or other commonly used outcome measures. We tried to mitigate this difficulty by presenting our results using a variety of outcomes, including purely clinical (cases of disability prevented) as well as those traditionally used in cost effectiveness analysis. Furthermore, because we did not do multiple way sensitivity analysis, we cannot predict how our results would change with simultaneous variation of several input parameters. Lastly, because of lack of data, we did not include other employer or societal costs such as decreased productivity, costs of replacing and retraining workers, shifting of costs from workers’ compensation onto health insurance and government health and welfare programmes, and other costs to workers and workers’ families. Including these costs would have further improved the cost effectiveness of surveillance. Future model based approaches will hopefully be able to address some of these limitations.
Policy implications
-
Model based analysis may provide valuable tools to evaluate screening strategies for isocyanate asthma and other work related diseases.
These cautionary notes notwithstanding, this study is the first we are aware of to provide a model based approach to surveillance for occupational asthma or other occupational diseases. Despite the limitations, we believe a model based approach can provide important insights and guidance into developing rational strategies for surveillance of isocyanate asthma. Model based approaches can also focus further investigation on those parameters most likely to impact the effectiveness and costs of surveillance for occupational diseases, and highlight the importance of considering societal and employer perspectives in assessing and sharing such costs and benefits. Our initial model based approach provides a possible template for other cost effectiveness analyses in the field of occupational medicine, as well as a framework by which the important issue of cost sharing between employers and society might be better understood.
APPENDIX: GLOSSARY
-
State-transition model. A framework that characterises the progression of disease as a sequence of transitions between fixed health states.
-
Markov model. A subclass of state-transition models, in which state-to-state transition probabilities depend only upon the current state and are otherwise independent of prior history.
-
Quality adjusted life year (QALY). A health outcome measure that combines quality and length of life as determined by eliciting and quantifying strength of preference. One year in perfect health equals 1 QALY. One year in a health state that is rated as 40% of perfect health equals 0.4 QALYs.
-
Symptom free day (SFD). Day without any symptoms of asthma. Used as a health outcome measure for asthma.
-
Cost effectiveness ratio. The added cost of gaining a unit of benefit by substituting one policy or intervention for another. The numerator represents the cost difference between the healthcare intervention and its alternative, whereas the denominator is the difference in benefits (that is, QALYs or SFDs).
-
Direct medical costs. Costs of resources consumed by directly providing medical care—for example, medications, hospital bills, and imaging studies.
-
Indirect costs. Other costs associated with illness, such as lost productivity or informal caregiving costs.
-
Annual discount rate. A measure of the time-value of health and economic outcomes. The discount rate is used to estimate present values of future cost and health effects.
-
Sensitivity analysis. A set of techniques to evaluate how robust (or sensitive) analysis results are in the face of parameter uncertainty. Key input parameters are varied to estimate how estimates and policy recommendations are influenced by changes over the plausible range.
-
Cost saving. A strategy is said to be cost saving if it produces both greater benefits and lower costs than an alternative allocation of resources. By convention, cost saving programmes are noted as such and no cost effectiveness ratio is reported. The reasoning behind this recommendation is that the ratio of savings to benefits is meaningless: although lower CE ratios typically imply more favourable programmes, their behaviour in the face of cost savings is ambiguous.
-
Key states of the model:
-
– Symptomatic, more reversible. In the first two years after becoming symptomatic, workers are assumed to have a high likelihood of reverting to the asymptomatic state if they are removed from exposure.
-
– Symptomatic, less reversible state. After two years of continued exposure, workers are assumed to have a lower rate of returning to the asymptomatic state if they are removed from exposure
-
– Removed, asymptomatic. State of workers who have been sensitised to isocyanates and then removed from exposure. These workers are healthy and able to work, but not with diisocyanates.
-
REFERENCES
Footnotes
-
Funding sources: CDC/NIOSH Grant 1R01OH03457, NIH/NIEHS grant K24-ES00355
-
Results of our model have been presented as an oral presentation at Medical Decision Making 2003 and ATS and are published as an abstract in
and in the . -
As this study did not involve direct patient contact, we did not need institutional ethics committee approval.