Article Text

Abstract
OBJECTIVES To update and assess mortality from neoplasms to 31 December 1995 among 10 109 men employed in a job exposed to vinyl chloride for at least 1 year between 1942 and 1972 at any of 37 North American factories. Previous analyses indicated associations between employment in vinyl production and increased mortality risk from cancers of the liver and biliary tract, due to increased mortality from angiosarcoma of the liver, and brain cancer.
METHODS Standardised mortality ratio (SMR) analyses, overall and stratified by several work related variables, were conducted with United States and state reference rates. Cox's proportional hazards models and stratified log rank tests were used to further assess occupational factors.
RESULTS 895 of 3191 deaths (28%) were from malignant neoplasms, 505 since the previous update to the end of 1982. Mortality from all causes showed a deficit (SMR 83, 95% confidence interval (95% CI) 80 to 86), whereas mortality from all cancers combined was similar to state referent rates. Mortality from cancers of the liver and biliary tract was clearly increased (SMR 359, 95% CI 284 to 446). Modest excesses of brain cancer (SMR 142, 95% CI 100 to 197) and cancer of connective and soft tissue (SMR 270, 95% CI 139 to 472) were found. Stratified SMR and Cox's proportional hazard analyses supported associations with age at first exposure, duration of exposure, and year of first exposure for cancers of the liver and soft tissues, but not the brain.
CONCLUSIONS Excess mortality risk from cancer of the liver and biliary tract, largely due to angiosarcoma, continues. Risk of mortality from brain cancer has attenuated, but its relation with exposure to vinyl chloride remains unclear. A potentially work related excess of deaths from cancer of connective and soft tissue was found for the first time, but was based on few cancers of assorted histology.
- vinyl chloride
- angiosarcoma
- liver
- brain
- connective tissue
- soft tissue
- neoplasms
Statistics from Altmetric.com
Vinyl chloride monomer (VCM), a colourless gas under normal temperature and pressure, is used almost exclusively to manufacture polyvinyl chloride (PVC) resin. Vinyl chloride monomer is manufactured by cracking ethylene dichloride in a pyrolysis furnace, and PVC is typically manufactured in a suspension process by addition polymerisation of VCM. Workers who cleaned caked polymer from the PVC reactor vessels, or autoclaves, historically sustained exposures to the highest concentrations of VCM. It was among these autoclave workers that health hazards related to vinyl chloride—such as scleroderma, acro-osteolysis, Reynaud's phenomenon, and angiosarcoma of the liver were first identified and documented.1-3
This study updates mortality to 31 December 1995 for a large cohort of men employed in the North American vinyl chloride industry between 1942 and 1972. The cohort was previously followed up for mortality to the end of 19724 5 and then 1982.6 7 Of particular interest in the current investigation is whether excess mortality from cancer of the liver and biliary tract, due to angiosarcoma of the liver, and brain cancer6 7 persisted with follow up to the end of 1995.
Methods
The study cohort was made up of male employees who worked for at least 1 year in a job exposed to vinyl choride between 1 January 1942 and 31 December 1972, at one of 37 North American factories that manufactured VCM or PVC resins and copolymers.6 7
DATA SOURCES
The data base from the previous update of the cohort served as the primary source of data.6 7 The following variables were available: subject study identification number, name, social security number (SSN), date of birth, date of first employment, date of leaving the plant, date of first assignment to a job exposed to vinyl chloride, plant code, employment status on 31 December 1980, duration of exposure to vinyl chloride, vital status on 31 December 1982, and if dead, cause of death coded to the seventh revision of the international classification of diseases (ICD-7). Many data elements were missing—for example, 847 study subjects were missing both name and SSN, critical personal identifiers needed for tracing vital status. We reviewed plant records and additional data from paper files comprising the study archive to obtain critical identifiers for some of these study subjects. Data on race were unavailable for most of the cohort.
Also, we updated employment status, when such information was available from the current owners of each plant, for those thought to be employed on 31 December 1980, the latest date for which employment status had been determined. However, some plants had closed since the previous update and personnel information was unavailable.
Of the 10 173 study subjects initially included in the study database, we excluded 11 women, one person who had stopped working before 1 January 1942, and the duplicate records of 52 study subjects. After exclusions, 10 109 study subjects were available for vital status update and mortality analysis. Person-years began accruing 1 year after first exposure to vinyl chloride or 1 January 1942, whichever was more recent.
VITAL STATUS UPDATE
To update vital status to 31 December 1995, we conducted searches of the National Death Index and the death records of the Social Security Administration. Also, we searched a mortality registry maintained by the Ontario Office of the Registrar General to determine vital status for 45 study subjects employed at a plant in Ontario, Canada. We were able to assess vital status for 1326 of the 1698 (including 48 duplicates) cohort members previously lost to follow up (table 1). Mortality search results were inconclusive for 201 people (death information from searches was not clearly relevant to the cohort members searched). These 201 cohort members, as well as an additional 123 cohort members missing the minimal information needed to conduct the mortality searches (name and SSN, or name and date of birth), were censored on the date they were last known to be alive.
Vital status for 10109 men employed for at least 1 year at one of 37 vinyl chloride plants between 1 January 1942 and 31 December 1972
Cause of death was found for 3159 (99%) of the 3191 decedents. A nosologist coded the underlying cause of death on the death certificates with the four digit rubric of the ICD-9. For 55 people identified as dead and for whom an ICD-7 code was available from the archive, the state vital statistics office could not locate a death certificate. The ICD-7 code for these deaths was used to assign the death to the appropriate category.8
MORTALITY ANALYSIS
Standardised mortality ratios (SMRs) and 95% confidence intervals (95% CIs) were calculated with ProSMR, a life table analysis module of the ProQuest database system (SoftWhere, Goshen, MA, USA and Applied Epidemiology, Amherst, MA, USA). Of the 3165 men (31% of the cohort) with known race, 96% were white; therefore, reference rates for white men were used for all analyses. Two sets of SMRs were calculated with the cause specific mortalities for the United States population as a whole and the populations of the 15 states in which the plants were located. The state rates were weighted by the distribution of person-years generated by employees at each plant. The use of state rates has the advantage of minimising bias from regional differences in mortality. Referent mortalities compiled by the National Institute of Occupational Safety and Health (NIOSH) for 92 cause of death categories8 were obtained for the United States white male population with CDC WONDER.9 For periods before 1960, mortalities for the white male population of the United States were obtained directly from NIOSH (K Steenland, personal communication). Because state mortalities were not available for years before 1960, rates for 1960–4 were used for the four 5 year calendar periods between 1940 and 1959, during which only 4% of the total study deaths occurred.
The SMR analyses were conducted overall, and stratified by duration of employment, time since first employment, age at first employment, and year of first employment in a job exposed to vinyl chloride, and by vinyl chloride production start date for the plant. This last analysis was conducted to consider the hypothesis that exposures in older plants may have been higher than in newer plants due to older production technology, irrespective of when each subject's first exposure occurred. Finally, Cox's proportional hazard analyses were used to investigate variations in occurrence of selected cancer deaths simultaneously by age at first exposure, duration of exposure, and year of first exposure.10
Results
A total of 3191 deaths had occurred by 31 December 1995 among the 10 109 study subjects followed up for a total of 316 520 person-years (table 1). About 3% of the cohort was lost to follow up.
Mortality patterns based on either United States rates or state rates were similar, although national mortalities were lower than state rates for many causes of death, resulting in higher SMRs. We present results with the state referent populations because these results provide the most appropriate comparison with background risk which may differ due to regional variation in mortalities.
Mortality from all causes of death showed a significant deficit of 17% (SMR 83, 95% CI 80 to 86), whereas mortality from all cancers combined showed a non-significant deficit of 4% (SMR 96, 95% CI 90 to 102), relative to the state referent populations (table 2). Cancers previously reported in excess were again found in excess: liver and biliary tract (SMR 359, 95% CI 284 to 446), which remained increased to the end of follow up; and brain (SMR 142, 95% CI 100 to 197), which was not increased in the 13 years of follow up since 1982 (14 observed; 12.2 expected). New excesses, based on smaller numbers, were found for cancers of the tongue (SMR 202, 95% CI 97 to 371), connective and other soft tissue (SMR 270, 95% CI 139 to 472), and peritoneum (SMR 216, 95% CI 93 to 427). Deficits were found for lung cancer (SMR 82, 95% CI 73 to 92) and cancers of the lymphatic and haematopoietic tissue (SMR 86, 95% CI 67 to 108).
Observed and expected deaths,2-150standardised mortality ratios (SMRs) (95% CIs), with state rates for white men as the reference
CANCER OF THE LIVER AND BILIARY TRACT
Mortality from cancer of the liver and biliary tract increased with duration of exposure: the SMRs were 83 (95% CI 33 to 171), 215 (95% CI 103 to 396), 679 (95% CI 483 to 929), and 688 (95% CI 440 to 1023) for 1–4, 5–9, 10–19, and ⩾20 years duration of exposure, respectively. For time since first exposure, the SMRs were 287 (95% CI 131 to 544), 323 (95% CI 200 to 493), and 434 (95% CI 322 to 572) for 10–19, 20–29, and ⩾30 years since first exposure, respectively. Large excesses were found for employees who had been first exposed to vinyl chloride before 1950 (SMR 499; 95% CI 368 to 662) or from 1950 to 1959 (SMR 311; 95% CI 197 to 467).
In Cox's proportional hazards analyses, age at first exposure, duration of exposure, and year of first exposure each were significantly associated with increased risk of mortality from liver cancer in crude analyses (table 3). Of greatest strength and significance was duration of exposure, which was independent of age at first exposure and year of first exposure. Age was of only marginal significance in crude analyses and was no longer significant in a model fitted with duration of exposure and year of first exposure. Stratified log rank analyses identified duration of exposure as the strongest predictor of hazard (stratified log rank test p<0.001, controlling for age; stratified log rank test p<0.001, controlling for year of first exposure).
Crude and adjusted hazards ratios (HRs) (95% CIs) for selected work related predictors of liver and biliary tract cancers (n=80)
ALL KNOWN ANGIOSARCOMAS
Of the 80 deaths from cancer of the liver and biliary tract, 33 (41%) were identified on the death certificate as due to angiosarcoma of the liver. We identified a total of 48 deaths due to angiosarcoma from both death certificates and a registry of cases of angiosarcoma of the liver related to VCM maintained by the Association of Plastic Manufacturers of Europe.11 As of February 1991, the register included 161 men with histologically confirmed angiosarcoma of the liver.12 Cases were registered by vinyl chloride manufacturers, trade organisations, and cancer agencies; however, the extent of coverage is not known. In the multivariable analysis of the angiosarcoma deaths, only duration of exposure significantly predicted death from angiosarcoma (table 4). Moreover, we found no evidence of a modification of the effect of duration of exposure on hazard of mortality by either age at first exposure or year of first exposure (table 4).
Crude and adjusted hazards ratios (HRs) (95% CIs) for predictors of all known angiosarcomas (n=48)
BRAIN CANCER
Although brain cancer showed no apparent trend with increasing duration of exposure, risk was greatest among those exposed for 20 years or more, based on nine deaths from brain cancer (SMR 290; 95% CI 132 to 551). The SMRs for brain cancer were increased for all categories of time since first exposure, but with no clear pattern (results not presented). The greatest excess was found for those who were first exposed before 1950 (SMR 174; 95% CI 97 to 288). Mortality from brain cancer also showed the largest excess for study subjects who had worked at plants beginning production before 1946, based on 22 deaths (SMR 177; 95% CI 111 to 268).
In the Cox's proportional hazard analysis, older age at first exposure and longer duration of exposure were associated with increased risk of mortality due to brain cancer (table 5). The apparent trend of increased risk with earlier year of first exposure was not significant. Stratified log rank analyses of the associations of age and duration of exposure, controlling for each other, suggested that these associations were not confounded and were of independent predictive value (stratified log rank test for age p=0.01 controlling for duration of exposure; stratified log rank test for duration of exposure p=0.08 controlling for age). We found an unexplained lack of excess hazard for the group with 10–19 years duration of exposure.
Crude and adjusted hazards ratios (HRs) (95% CIs) for predictors of brain cancers (n=36)
CANCER OF CONNECTIVE AND OTHER SOFT TISSUE
Mortality from cancer of connective and other soft tissue showed significant excesses for those employed for 10–19 years (SMR 477; 95% CI 155 to 1113) and for those employed for 20 years or more (SMR 725; 95% CI 197 to 1856). Mortality from cancer of connective and other soft tissue was significantly increased for first exposure before 1950 (SMR 333; 95% CI 108 to 777) and from 1950–9 (SMR 468; 95% CI 188 to 964), with a fourfold excess among workers in plants with vinyl production start up dates during 1946–59, based on nine observed deaths. No deaths due to these cancers were found among cohort members first exposed since 1960. There were too few deaths from cancer of connective and other soft tissue to conduct multivariable analyses.
Discussion
This study updated vital status to 31 December 1995 of a cohort of 10 109 men who worked for at least 1 year in a job exposed to vinyl chloride before 1972 and who were employed in 1942 or later at one of 37 facilities in the United States or Canada. Cause of death was determined for 99% of the 3191 decedents. This study included the largest group of vinyl chloride workers who presumably sustained exposure to the highest concentrations of VCM in North America, as indicated by the substantial number and distribution of deaths due to angiosarcoma of the liver. Also, because of the long period of follow up of cohort members—from 20 to more than 50 years for all of the workers—an adequate latency period has passed for most if not all malignancies. Thus, mortality excesses due to any but the rarest cancers which might be associated with vinyl chloride were probably detectable with this update.
Early studies of vinyl chloride cohorts suggested that those exposed to vinyl chloride may be at increased risk of lung cancer, but relative risk estimates were based on relatively few deaths.13-16Although Infante17 suggested that the lung should be considered a target organ for the carcinogenic effects of exposure to vinyl chloride, Doll18 argued that any risk of lung cancer was small and associated with the oldest cohorts who were possibly exposed to higher concentrations of vinyl chloride. Two recent studies conducted in Italy have again suggested increased risks of lung cancer among vinyl chloride workers.19 20 In this study, however, we did not find evidence of any association between mortality from lung cancer and employment with vinyl chloride overall, nor with any characteristic related to employment (analyses not presented). The lack of any pattern by year of first exposure and year in which production of vinyl chloride started suggests that not even a small risk was present among the oldest subgroups within the study cohort.
Although the reasons for lower than expected mortality from lung cancer are unknown, a likely explanation is that the prevalence (or intensity) of smoking among cohort members was lower than in the general population in the areas the plants operated. This may be due to less smoking at work (because of fire or explosion hazards near VCM), or due to the high prevalence of smoking in the general population in the south east—the region most highly represented in this cohort. The SMR for lung cancer with the United States referent rate (SMR 96, 95% CI 86 to 107) was substantially higher than the SMR with the state rates (SMR 82, 95% CI 73 to 92), indicating that regional lung cancer mortalities were conspicuously high. Further, tobacco consumption habits among cohort members may have favoured oral snuff and chewing tobacco over cigarettes, especially if smoking were prohibited at work. Although this is speculative, the twofold excess in mortality from cancer of the tongue suggests smokeless tobacco may have been used by some cohort members.
Despite the absence of an excess of lung cancer, mortality from cancers of other parts of the respiratory system were moderately increased. This finding, although based on only six deaths, and the finding of a twofold excess in cancers of the peritoneum and other and unspecified parts of the respiratory system, raises the possibility of exposure to asbestos for some cohort members. A review of death certificates coded to these two categories of death, as well as the category for malignant neoplasms of other and unspecified sites, identified malignant mesothelioma as the underlying cause of death for eight decedents, including two deaths from pleural mesothelioma, one death from peritoneal mesothelioma, and five deaths from malignant mesothelioma, site not specified. These eight decedents worked at five different plants, but the likelihood of asbestos exposure at any of the vinyl plants is unknown.
CANCER OF THE LIVER AND BILIARY TRACT (INCLUDING ANGIOSARCOMA OF THE LIVER)
Of 80 deaths from cancer of the liver and biliary tracts, 33 (41%) were specified on the death certificate as due to angiosarcoma of the liver. Relying solely on information about cause of death reported on the death certificate, however, resulted in underascertainment of deaths from angiosarcoma of the liver in this study, confirming a finding reported by other investigators.18 21 22 A case report describing two VCM workers diagnosed with primary hepatocellular carcinoma in the absence of known risk factors for the disease, suggests that exposure to VCM may also be associated with primary liver cancers of other cell types.23 Although primary liver cancers other than angiosarcoma of the liver cannot be ruled out as a possible consequence of exposure to VCM, studies that rely on death certificate diagnoses, including this study, may not be able to elucidate this issue.
The risk of cancer of the liver and biliary tracts seems to be decreasing over time for this cohort, after the SMR peaked during the 1970s (SMR 472; 95% CI 288 to 729). Despite the decreasing mortality from cancer of the liver and biliary tract, excesses continued to be found throughout the study period (fig 1).
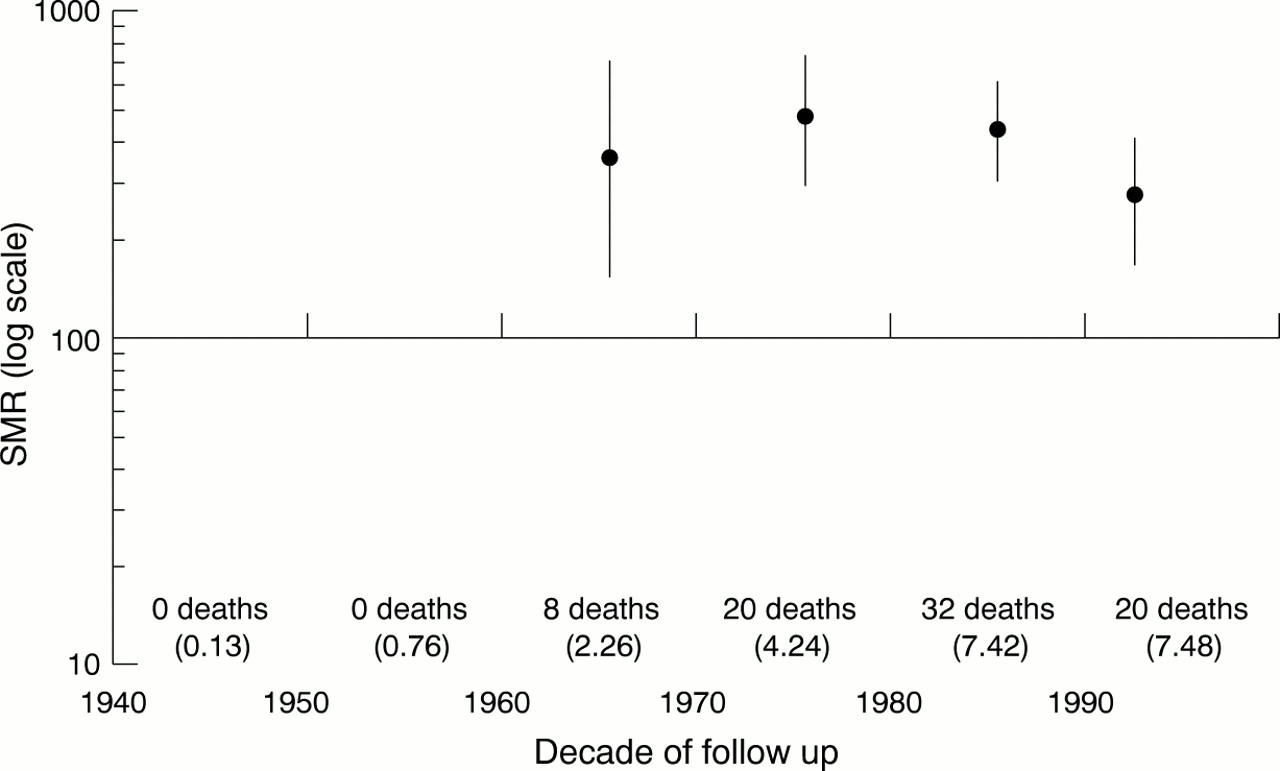
SMRs (95% CIs) for cancer of the liver and biliary tracts (ICD-9 codes 155–156) by decade of follow up (number of expected deaths reported in parentheses under number of deaths observed).
CANCER OF CONNECTIVE AND OTHER SOFT TISSUE
Mortality from cancer of connective and other soft tissue showed a significant excess that was more than twofold. Four of the 12 deaths reported were recorded as angiosarcoma on the death certificate, but no anatomical site was specified. The exclusion of these four deaths from angiosarcoma—presuming they are deaths misclassified as from angiosarcoma of the liver—from the category of cancers of connective and other soft tissue still resulted in an excess for the category based on eight deaths (4.4 expected). Other cancers of connective and soft tissue reported in this category included two liposarcomas, two malignant fibrous histiocytomas, and one (each) fibrosarcoma, leiomyosarcoma, and neurogenic sarcoma. A death certificate could not be found by the state vital statistics offices for one of the 12 deaths but this death had been coded to ICD-7 197 (malignant neoplasm of connective tissue) by the previous investigators. The only other study of workers who worked with VCM or PVC to have published mortality results for cancers of connective and soft tissue reported that none was found (1.4 expected).24
Sarcomas included in the category of cancer of connective and other soft tissue may arise in various tissues, but due to their extreme rarity, are often aggregated across histological types for study. Because the rules for coding underlying cause of death are based on anatomical site, many histological types (angiosarcoma, liposarcoma, leiomyosarcoma, etc) of cancer of connective and other soft tissue may be coded as a cancer occurring in parenchyma of specific organs, such as stomach or pancreas, rather than the category of cancer of connective and other soft tissue. Thus, estimates of the percentage of soft tissue sarcomas that are classified to ICD categories for anatomical sites rather than the ICD category of cancer of connective and soft tissue range from less than 10% (for liposarcomas) to more than 90% (for dermatofibrosarcoma).25 In a review of deaths occurring among 6716 workers exposed to dioxin and 10 240 workers exposed to chlorinated naphthalene, only 53% of soft tissue sarcomas identified from death certificates were coded to the ICD category malignant neoplasms of connective and other soft tissue.26 In our study, we know of four sarcomas of cell types other than angiosarcoma that were coded to a cancer of a specific organ.
Rhomberg27 reported that out of 21 adult cases with vascular soft tissue sarcomas (five angiosarcomas, 10 malignant hemangioendotheliomas, and seven malignant hemangiopericytomas) diagnosed between 1975 and 1995, four patients had long lasting exposure to vinyl chloride either alone or together with other polymers. There was no case of angiosarcoma of the liver. Other case reports of vascular sarcomas induced by vinyl chloride occurring at sites outside the liver have included the thyroid gland,28maxillary antrum,29 bladder,30 and genitals.31 From 1983 to 1987, the surveillance epidemiology and end results (SEER) programme of the United States National Cancer Institute reported an age adjusted incidence for angiosarcoma (all sites) of 1.5/million/year in the white population.25 Just over half of all angiosarcomas occur in parenchymal sites, with the most common sites being the breast, the liver, and the skin.25
Very little is known about the aetiology of soft tissue sarcoma, despite several recent studies, nearly all of which were based on fairly small sample sizes. Excess mortality from soft tissue sarcoma has been reported among workers exposed to phenoxy herbicides contaminated with 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD), although the excesses were based on 11 or fewer deaths.32-34 Self reported exposure to chlorophenols and cutting oils has been associated with increased risks of leiomyosarcoma and malignant fibrohistiocytic sarcoma and self reported herbicide use has been associated with increased risks of malignant fibrohistiocytic sarcoma.35
BRAIN CANCER
Although several studies have reported excess mortality from brain cancer among workers exposed to VCM or PVC, most of the increased SMRs were found in earlier studies of this cohort,4-7 or in studies with cohorts that are subsets of or overlap with this cohort.13 14 36 Two studies of workers exposed to VCM or PVC in other countries have reported no excess mortality from brain cancer,24 37 whereas three studies have reported excesses based on six or fewer deaths from brain cancer.15 38 39A multicentre study of such workers in four countries (United Kingdom, Italy, Sweden, and Norway) identified a total of 14 deaths from brain cancer (13.1 expected), with the largest excess occurring among workers with 30 years or more since first exposure (SMR 407; 95% CI 111 to 1041), based on four deaths.24 There was no clear pattern with duration of employment, ranked level of exposure (low, medium, or high) or cumulative exposure to vinyl chloride, but the exposure level was not known for six of the 14 deaths from brain cancer.
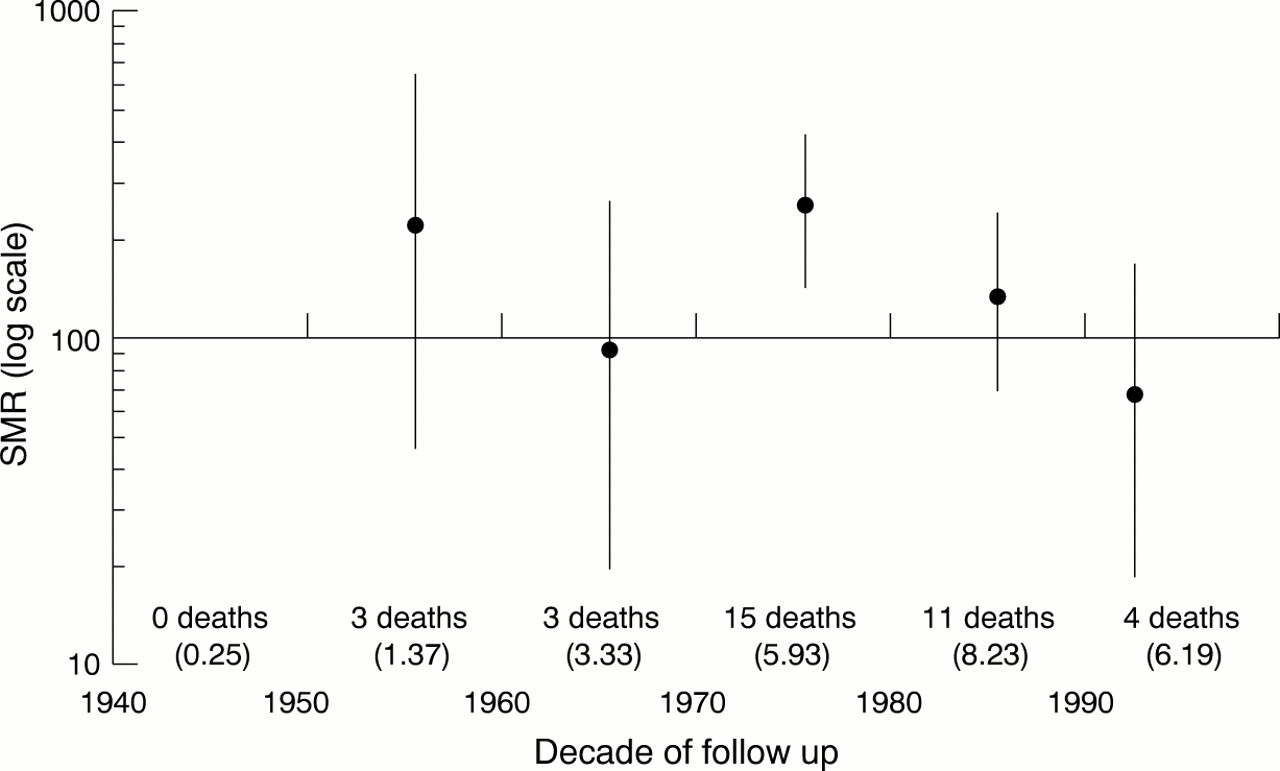
In our study, there was no clear trend in the SMRs for brain cancer over the study period (fig 2). However, mortality from brain cancer showed a concomitant peak with mortality from cancer of the liver and biliary tracts, with the greatest excess occurring in the decade 1970–9 (SMR 253, 95% CI 141 to 417). Between 1983 and 1995, 14 additional cases occurred (12.2 expected), suggesting that any risk of brain cancer associated with employment in the vinyl chloride industry has tapered off. Twenty one deaths from brain cancer occurred among employees at two of the oldest plants in which vinyl chloride production began before 1946. It is not known if these employees were exposed to carcinogens other than VCM.

{kind=link}
{kind=link}
SMRs (95% CIs) for cancers of the brain and central nervous system (ICD-9 codes 191–192) by decade of follow up (number of expected deaths reported in parenthesis under number of deaths observed).
Some argue that excesses of brain cancer found in this and other occupational cohorts are explained by a diagnostic sensitivity bias, due to health insurance benefits and better access to diagnostic techniques enjoyed by employed groups relative to the general population.40-43 Of the 36 deaths from cancer of the brain and central nervous system found to the end of 1995, there were 28 gliomas (15 glioblastomas, seven astrocytomas, five gliomas not otherwise specified, and one ependymoma). Gliomas, particularly glioblastomas and other astrocytic tumours, are aggressive, have a poor prognosis,44 and are unlikely to require sensitive diagnostic techniques for detection. Brain cancer mortalities have increased concurrently over the entire study period for the general population as well.45 Thus, a diagnostic sensitivity bias seems an unlikely explanation for the excess of brain cancer.
Further, because rates of cancer of the brain increase substantially with age, numerous new cases of brain cancer are likely to occur among this cohort. However, based on the available evidence, it is unlikely that new cases will be related to exposures to vinyl chloride, as the excess rates found in the 1970s seem to have returned to expected levels. Whether the excess found during the earlier decades was due to exposure to VCM or other exposures sustained while employed in the vinyl industry is unclear.
Conclusions
Consistent with all previous reports, deaths from liver cancers have occurred in excess, due to the well documented association between VCM and angiosarcoma of the liver. This excess mortality continued in the 13 years of follow up since the end of 1982, as about three times the number of deaths from liver cancer were found than were expected (41 observed; 13.2 expected).
A significant excess of mortality from brain cancer was found at baseline and on follow up; however, the size of that excess has decreased with time, and has decreased substantially during the most recent follow up period. Stratified analyses showed that the greatest risk occurred among those first employed earliest and for longest. This is supportive of a cumulative occupational risk factor. Unfortunately, no firm conclusion may be made about an association with vinyl chloride.
A significant excess (albeit based on relatively few cases) of cancers of connective and soft tissue was found. This group of cancers have several interesting patterns in the stratified analyses, similar to those found for liver and biliary cancers. By contrast with mortality due to liver and biliary cancers, mortality risk due to cancer of connective and other soft tissue was greatest among those older than 35 when first employed in a job with exposure to vinyl chloride. Although the association between mortality from cancer of connective and other soft tissue and vinyl chloride is a provisional finding, the epidemiological evidence of an association is compelling and will require additional investigation.
Acknowledgments
We thank Drs Harvey Checkoway and Kristan Aronson for their many helpful comments on this manuscript. We also thank Robert Bilgrad, who provided technical advice, and the staff of the National Center for Health Statistics (National Death Index). This study could not have been completed without the assistance of staff from the respective state vital statistics offices; due to space limitations, we are unable to acknowledge each state separately. Dr Susanne May and Elizabeth A Smith provided technical assistance. Dr Kyle Steenland assisted us in acquiring mortality rates for the years between 1940 and 1959. This work was funded by the Chemical Manufacturers Association (Arlington, Virginia).