Article Text

Abstract
Objectives Healthcare workers (HCWs) are at high risk of developing SARS-CoV-2 infection. The aim of this single-centre prospective study was to evaluate the trend of SARS-CoV-2 seroprevalence in HCWs working at the primary referral centre for infectious diseases and bioemergencies (eg, COVID-19) in Northern Italy and investigate the factors associated with seroconversion.
Methods Six hundred and seventy-nine HCW volunteers were tested for anti-SARS-CoV-2 antibodies three times between 4 March and 27 May 2020 and completed a questionnaire covering COVID-19 exposure, symptoms and personal protective equipment (PPE) training and confidence at each time.
Results SARS-CoV-2 seroprevalence rose from 3/679 to 26/608 (adjusted prevalence: 0.5%, 95% CI 0.1 to 1.7% and 5.4%, 95% CI 3.6 to 7.9, respectively) between the first two time points and then stabilised, in line with the curve of the COVID-19 epidemic in Milan. From the first time point, 61.6% of the HCWs had received training in the use of PPE and 17 (61.5%) of those who proved to be seropositive reported symptoms compatible with SARS-CoV-2 infection. Contacts with ill relatives or friends and self-reported symptoms were independently associated with an increased likelihood of seroconversion (p<0.0001 for both), whereas there was no significant association with professional exposure.
Conclusion The seroprevalence of SARS-CoV-2 among the HCWs at our COVID-19 referral hospital was low at the time of the peak of the epidemic. The seroconversions were mainly attributable to extrahospital contacts, probably because the hospital readily adopted effective infection control measures. The relatively high number of asymptomatic seropositive HCWs highlights the need to promptly identify and isolate potentially infectious HCWs.
- occupational health
- viruses
- health personnel
- longitudinal studies
- personal protective equipment
Data availability statement
Data are available on reasonable request. Anonymised participants data were collected in a protected database and are available on reasonable request from LM (laura.milazzo@asst-fbf-sacco.it) and ALR (annalisa.ridolfo@asst-fbf-sacco.it).
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
The reported rates of SARS-CoV-2 infection in healthcare workers (HCWs) in Europe range from 3% to 45%.
HCWs accounted for 12% of the 250 495 COVID-19 cases recorded in Italy as of 10 August 2020, with 176 doctors who have died so far.
Serological surveys are fundamental to estimate the burden of asymptomatic infection in healthcare settings and to determine the factors associated with an increased risk of SARS-CoV-2 seroconversion.
What are the new findings?
SARS-CoV-2 seroprevalence in HCWs working at a COVID-19 referral hospital in Milan rose from 0.5 (95% CI 0.1 to 1.7) to 5.4 (95% CI 3.6 to 7.9) during the first month of epidemic and then stabilised, in line with the curve of the COVID-19 epidemic in Milan, but lower than what reported in other city Hospital settings.
Contacts with ill relatives were independently associated with an increased likelihood of seroconversion, whereas there was no significant association with professional exposure.
How might this impact on policy or clinical practice in the foreseeable future?
High confidence with the use of personal protective equipment together with the early implementation of preventive measures throughout the hospital played a crucial role in containing the spread of the virus and should be largely adopted in any clinical setting.
The relatively high number of asymptomatic HCWs who tested positive to SARS-CoV-2 antibodies highlights the need for the surveillance of asymptomatic HCWs in order to protect both staff and patients from possible nosocomial transmission.
Introduction
SARS-CoV-2, the aetiological agent of COVID-19, was first detected in the city of Wuhan, China, in December 2019, and its rapid spread worldwide has led to a pandemic health crisis.1–3 The first autochthonous case of COVID-19 in Italy was diagnosed on 20 February 2020, and over the following few weeks, Northern Italy (particularly Lombardy) experienced a dramatic rise in the number of COVID-19 cases and deaths that quickly made Italy the second most affected country in the world after China.4–6
The COVID-19 outbreak has been extremely stressful for frontline healthcare workers (HCWs) operating in highly affected areas as they have had to face rapid changes in their operative routine, overcrowding, increased workloads and limited access to personal protective equipment (PPE),7 all of which may have increased their risk of acquiring and transmitting the infection. Data provided by the Istituto Superiore di Sanità show that HCWs accounted for 12% of the 250 495 COVID-19 cases recorded in Italy as of 10 August 2020,8 and it has also been reported that 176 doctors have died so far.9 However, serological surveys are required to clarify the burden of SARS-CoV-2 infection among HCWs, not least because they may contribute to the nosocomial spread of the infection.
The Luigi Sacco University Hospital (LSUH), ASST Fatebenefratelli-Sacco became the first COVID-19 referral centre in Milan because it has a large department of infectious diseases (IDs) and an intensive care unit (ICU) capable of dealing with epidemiological emergencies in Northern Italy. However, the rapid surge in the number of COVID-19 cases between February and March 2020 required an urgent and profound reorganisation that involved other medical and surgical wards in order to increase capacity. At the same time, a large number of HCWs were moved from general to newly created COVID-19 wards.
The aim of this study was to evaluate the dynamics of the seroprevalence of SARS-CoV-2 antibodies in a cohort of HCWs working at LSUH during the first 3 months of the COVID-19 epidemic and determine the factors associated with an increased risk of SARS-CoV-2-seroconversion that may be helpful to implement adequate prevention and control measures. It also assessed the extent to which asymptomatic infections occur in a high-risk healthcare setting, where they may contribute to the nosocomial spread of the infection.
Methods
Hospital setting
LSUH is a 550-bed university hospital located in the metropolitan area of Milan, Italy, that admits an average of 20 000 patients per year. It is a referral centre for infectious diseases and has a dedicated 90-bed department that is also equipped to handle infectious disease emergencies occurring in Northern Italy.
On 21 February 2020, the hospital admitted two patients with SARS-CoV-2 pneumonia who were transferred from the small Lombard town first affected by the epidemic. Over the following 2 weeks, the hospital had to close down its routine activities because a dramatic surge in the number of cases meant that it could only accept patients with COVID-19, which soon required radical structural changes to its organisation, including the creation of a new ID area, the conversion of the eight-bed general ICU into a strictly isolated 30-bed ICU located in the ID department, and the transformation of some medical and surgical wards into COVID-19 wards. These changes increased the number of beds for patients with COVID-19 from 109 to 328 (figure 1) and led to the recruitment of 168 doctors and 838 nurses/health service assistants to manage the emergency between March and May 2020.

Reorganisation at Luigi Sacco University Hospital (LSUH) to increase the number of COVID-19 dedicated beds and wards (in black) during the the first weeks of the epidemic in Lombardy. ER, emergency room; ID, infectious diseases department.
Study design and participants
This cohort study evaluated the dynamics of SARS-CoV-2 seroprevalence among the hospital’s HCWs between 21 February and 27 May 2020. All of the hospital personnel (696 nurses, 346 doctors, 205 health service assistants including cleaners, 188 administrative staff and 115 healthcare technicians) were invited to participate in the 3-month serological survey on a voluntary basis and those who agreed gave the written informed consent to the storage of their anonymised data in a protected database.
The three serum samples were collected from each participant: one during the very early phase of the epidemic in Italy (4–12 March), and the others approximately 1 and 2 months later (14–22 April and 20–27 May). At the same times, the participants were asked to complete a questionnaire that, in addition to demographic and occupational data, included questions concerning whether they had worked in COVID-19 wards, had otherwise been exposed to patients with COVID-19 during their work and/or been in contact with relatives or friends with suspected or ascertained COVID-19 during the preceding 30 days; whether they had experienced symptoms possibly related to SARS-CoV-2 infection (fever, myalgia, fatigue, sore throat, conjunctivitis, gastrointestinal symptoms, anosmia/dysgeusia, cough and dyspnoea) during the preceding 30 days; whether they had ever been trained in the use of PPE use and how confident they were about its use; and whether they had had any problems with PPE during the preceding 30 days.
Their occupations were categorised as doctors, nurses, other healthcare service workers (radiologists, physiotherapists and laboratory staff), other health service assistants (including cleaners) and socioadministrative personnel.
Serological assays
All of the blood samples were stored at −20°C until we had the serological assay available (end of May 2020). The presence of SARS-CoV-2 antibodies was qualitatively determined using a Wantai SARS-CoV-2 Total Ab ELISA (Beijing Wantai Biological Pharmacy Enterprise, Beijing, China) in accordance with the manufacturer’s protocol. This assay, European Conformity marked, is based on the principle of a double-antigen sandwich and detects antibodies binding to the SARS-CoV-2 spike protein receptor binding domain in human serum or plasma. It has been validated in previous studies on series of patients hospitalised with COVID-19 and its reported sensitivity and specificity are, respectively, 93%–98% and 99%–100%.10 11 We also validated the assay in our laboratory using plasma samples taken from 144 consecutive inpatients with RT-PCR confirmed COVID-19 and 100 samples collected between 2003 and 2010 for research purposes and obtained a sensitivity of 78% and a specificity of 100%.
Statistical analysis
The descriptive analyses are expressed as median values and IQR, or absolute numbers and percentages. The raw frequency of seropositive HCWs at the different study time points was expressed as a proportion with its exact binomial CI, after which the estimates of SARS-CoV-2 seroprevalence were adjusted for the diagnostic performance of the test using the following formula

where the raw prevalence was the proportion of the positive tests using the test kit, and sensitivity and specificity were estimates obtained from local cases and controls.12 13 Variations in the characteristics of the cohort and SARS-CoV-2 seroprevalence over time were assessed using a generalised linear multilevel model, with the SAS PROC GLIMMIX procedure being used to correlate repeated measures.
Univariate and multivariable logistic regression analyses were used to evaluate the odds of seroconverting between two consecutive SARS-CoV-2 antibody tests during the period in which the number of COVID-19 was increasing by including all of the subjects with both serological test results who were negative at the time of the first assessment. The data used to build the regression logistic models were obtained from the questionnaires completed until the second determination in order to use the information pertaining to the seroconversion interval. All variables deemed to be potentially associated with the likelihood of seroconversion (age, sex, professional status, contacts with infected relatives, professional contacts with patients with COVID-19, symptoms, training in PPE use and confidence with PPE use) were introduced in the multivariable model by adjusting each variable for all the others.
All of the statistical analyses were made using SAS V.9.4 software, and differences with p values of <0.05 were considered statistically significant.
Results
Six hundred and seventy-nine HCWs (513 women (75.6%) women and 166 men (24.4%) with a median age of 45 years (IQR 34–53)) were enrolled, all providing a first serum sample between 4 and 12 March 2020. The overall response rate was 44% (679/1550 employees). There were 247 nurses, 206 doctors, 86 health service assistants (including cleaners), 75 healthcare service workers and 65 socioadministrative employees. Table 1 shows their main characteristics and the results of the SARS-CoV-2 antibody tests at the different times.
Characteristics of the study population
There was an increase in the proportion of HCWs in contact with patients with COVID-19 (from 30.5% in March to 66% in April and May; p for trend <0.001) or having had contacts with infected relatives or friends (p for trend=0.006). There was also significant increase in the percentage of participants reporting that they had trained in the use of PPE and were highly confident with it between the first and second time points.
The number of HCWs who tested positive for SARS-CoV-2 antibodies increased from three (0.4%) at the first time point to 26 (4.2%) at the second time point, including 23 subjects (3.8%) who seroconverted between the two. At the third time point, 29 subjects (4.6%) were seropositive, including three who seroconverted between the second and the third time points.
Of the 29 HCWs who tested positive during the study period, 16 (61.5%) reported that they had had symptoms suggesting SARS-CoV-2 infection during the 30 days preceding the test: asthaenia and anosmia/ageusia were the most frequently reported (34.6%), followed by cold-like symptoms, fever and cough (15% each), and myalgia and conjunctivitis (7.7% each). Two of the symptomatic subjects required hospitalisation. The remaining 13 seropositive HCWs remained asymptomatic throughout the study period. Fifteen of the 29 seropositive HCWs underwent a SARS-CoV-2 RT-PCR nasopharyngeal swab (NPS) test during the 30 days preceding the detection of serological positivity, eight of whom were positive; the remaining 14 did not undergo an NPS test during the study period.
Estimates of SARS-CoV-2 seroprevalence
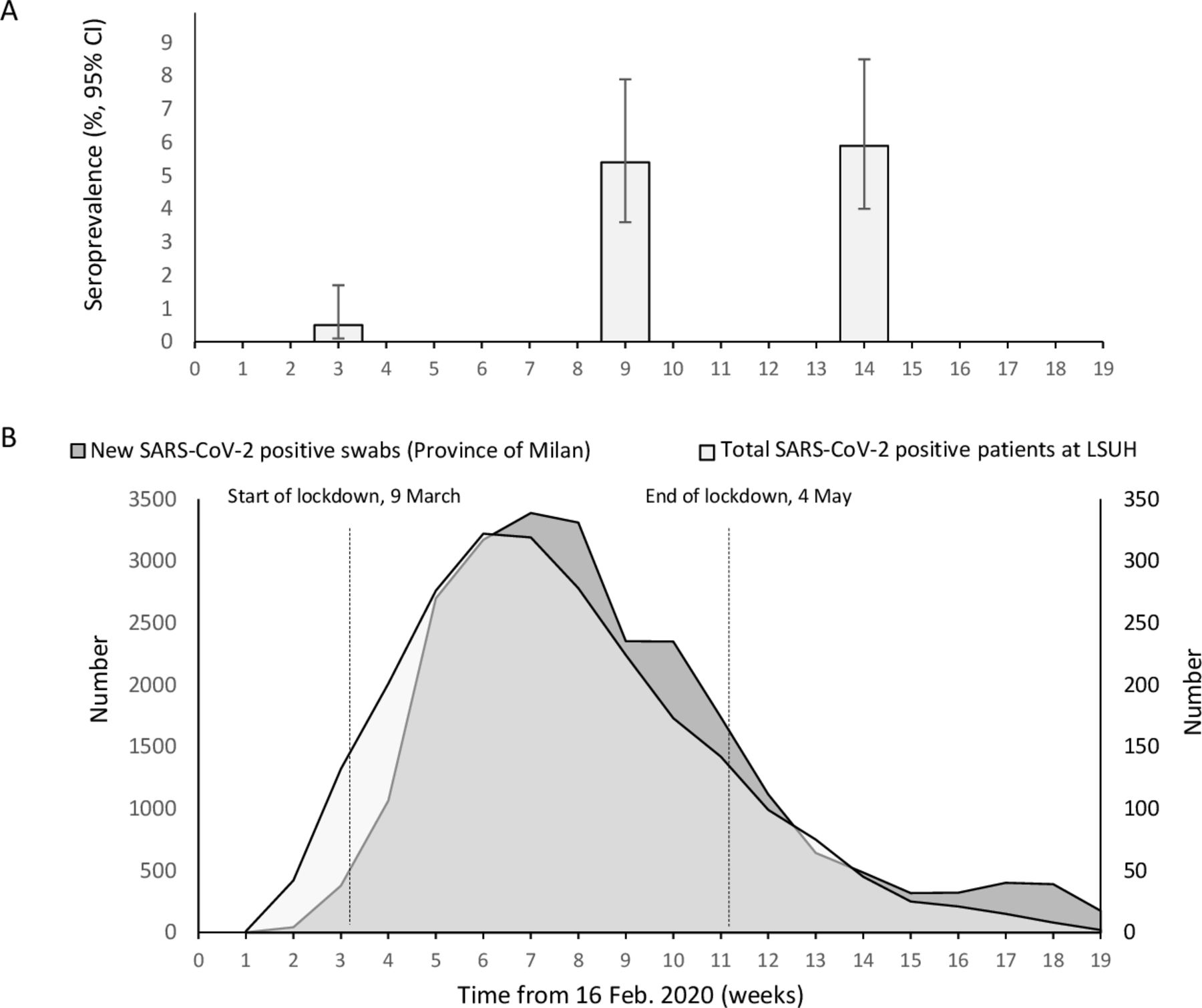
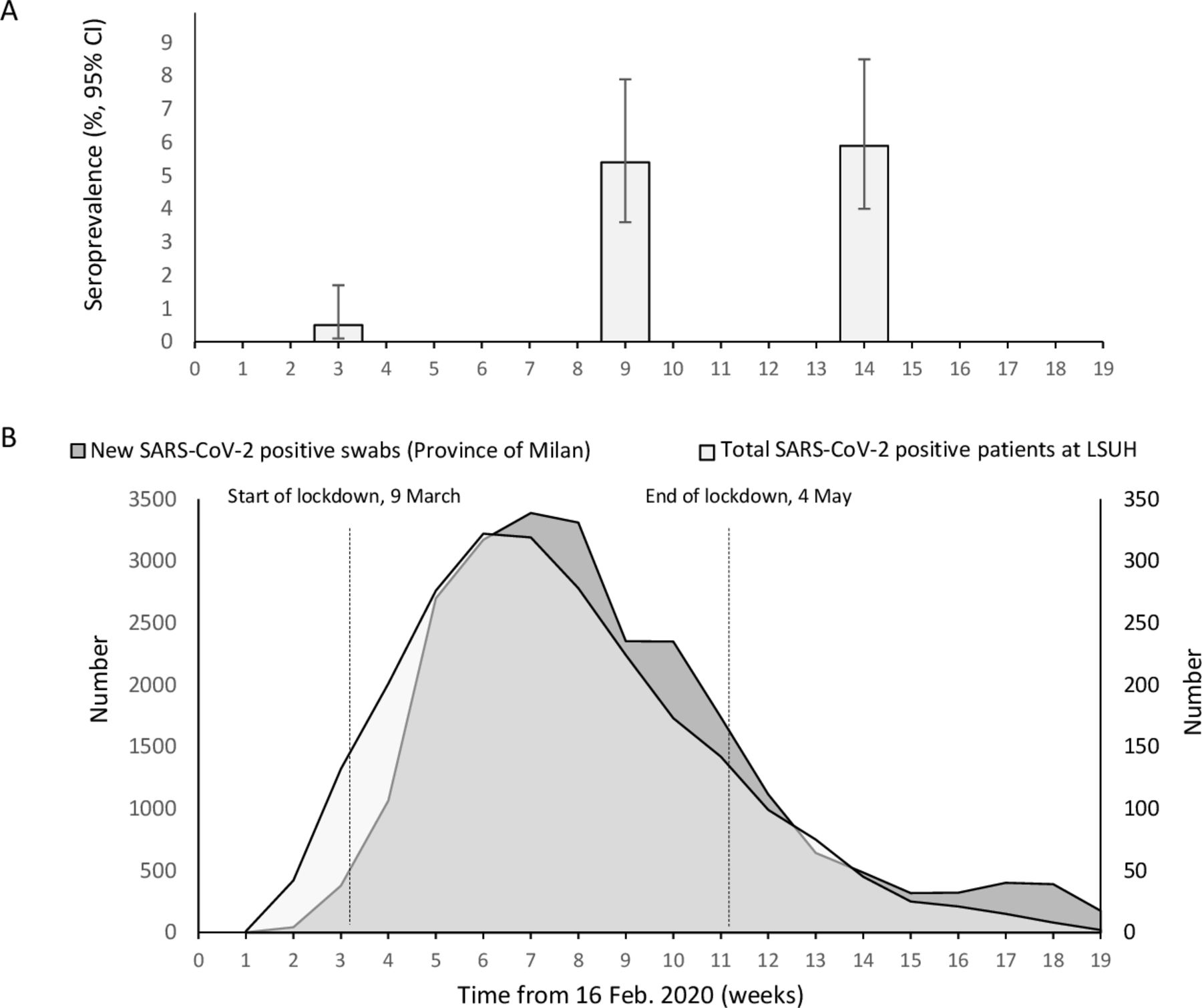
As shown in figure 2, this survey was conducted during the exponential growth of the epidemic in Lombardy, which peaked between 25 March and 10 April; the lockdown in Italy started on 9 March and lasted until 4 May, leading to a progressive decline in the number of new cases.
{kind=link}
{kind=link}
(A) Estimated SARS-CoV-2 seroprevalence (95% CI) among HCWs at Luigi Sacco University Hospital (LSUH) in Milan, Italy. (B) Number of new RT-PCR confirmed cases of SARS-CoV-2 infection in Milan Province (dark grey) and of ascertained patients with COVID-19 at LSUH (light grey). The y-axes show the weekly number of new SARS-CoV-2 positive patients in the province of Milan (left; data from the Istituto Superiore della Sanità) and the weekly number of SARS-CoV-2 positive in-patients at LSUH (right).
The adjusted seroprevalence in our cohort significantly increased from 0.5 (95% CI 0.1 to 1.7) in March to 5.4 (95% CI 3.6 to 7.9) in April and 5.9 (95% CI 4.0 to 8.5) in May (figure 2A), overlapping the trajectories of the weekly number of new positive NSP tests in the province of Milan and the weekly number of patients with COVID-19 hospitalised at LSUH (figure 2B). Accordingly, the highest number of seroconversions in our cohort coincided with the peak of the epidemic in Milan.
Factors associated with SARS-CoV-2 seroconversion
Table 2 shows the univariable and multivariable logistic regression analysis of the factors associated with the odds of seroconverting during the first 2 months of the survey. Reported contacts with ill relatives or friends and experiencing symptoms attributable to COVID-19 were independently associated with an increased likelihood of seroconverting (adjusted OR (aOR) 8.12, 95% CI 2.95 to 22.34, p<0.0001, and 15.13, 95% CI 5.97 to 38.37, p<0.0001). Sex, age, occupational category and having been exposed to patients with COVID-19 (aOR 1.19, 95% CI 0.37 to 3.79) were not associated with an increased risk.
Univariable and multivariable logistic regression analysis of factors associated with the risk of seroconverting between 4–12 March and 14–22 April
Discussion
This paper describes the estimated seroprevalence of SARS-CoV-2 antibodies in a cohort of 676 HCWs working in a referral hospital for contagious diseases from the beginning to the peak of the COVID-19 outbreak in Milan. The Wantai total Ab assay used has previously been found to perform well and to have an acceptable positive predictive value even in populations with a low seroprevalence.10 11
The estimated seroprevalence of SARS-CoV-2 increased from 0.5 (95% CI 0.1 to 1.7) in March to 5.4 (95% CI 3.6 to 7.9) in April and reached a plateau in May, in line with the course of the epidemic in Milan. Two previous studies have cross-sectionally evaluated the prevalence of SARS-CoV-2 infection among HCWs working in Milan hospitals14 15: the study by Lombardi et al 14 was conducted in a very early phase (12 February–31 March) and found that 139 (8.8%) of 1573 HCWs had a positive NSP test; the study by Sandri et al 15 was carried out between 28 April and 16 May and found a similar prevalence (8%) in 2872 employees of three hospitals tested for SARS-CoV-2 antibodies. Both of these findings are higher than ours. The only available data concerning the general population of Milan come from a cross-sectional study of anti-SARS-CoV-2 IgM/IgG using a lateral flow immunoassay in healthy asymptomatic blood donors, which indicated a seroprevalence of 7.2%.16 The reported rates of SARS-CoV-2 infection in HCWs in Europe range from 3% to 45%14 15 17–23 and depend on the testing approach (ie, testing only symptomatic or both symptomatic and asymptomatic subjects), the diagnostic method (ie, PCR tests of NPS or serology, or both) and, mainly, the intensity of the local epidemic at the time. Even the data concerning Lombardy (the Italian region most involved by the epidemic) range widely (from 3% to 43%) and are strictly related to the epidemic burden in the area.15
The lower seroprevalence observed in our study may be explained by the fact that our hospital is the reference centre for infectious diseases and bioemergencies in Northern Italy and has the largest number of ID beds in Lombardy and an active biocontainment unit in which ID and ICU staff are continuously trained to use different types of PPE. As demonstrated during the SARS outbreak and the COVID-19 epidemic in China, the appropriate use of masks, gloves, gowns and hand hygiene is effective in preventing virus transmission in clinical settings,24–27 and so it is likely that the availability of PPE and confidence in using it, together with the early implementation of preventive measures throughout the hospital (including the use of surgical masks in COVID-free areas and by colleagues not involved in treating patients with COVID-19) played a crucial role in containing the spread of the virus. It must be acknowledged that differently from other clinical settings and territorial health facilities, our hospital did not experience severe shortage of PPE at any time of the outbreak. It should also be noted that we did not find any difference in seroprevalence between the HCWs working in medical wards converted into COVID-19 wards and those working in the ID department (data not shown), which indicates that negative-pressure rooms are not essential if PPE is used and suitable infection control measures are taken.
In line with the findings of other recent studies,18 28 we found that previous contacts with COVID-affected relatives or friends and a history of symptoms consistent with COVID-19 were strongly associated with an increased likelihood of testing positive for SARS-CoV-2 antibodies, whereas there was no significant association with the type of occupation or having had contacts with hospitalised patients with COVID-19. Notably, while at the time of first data collection, out-of-hospital contacts with both relatives and friends had been reported; over the remaining study period, the same were prevalently referred to relatives cohabitating with the HCW as the result of the strict lockdown measures imposed to Italy. Although our study is not designed to define the dynamics of infection within family clusters, the fact that the probability of seroconversion among HCWs at the different time points was consistent with the incidence of infection in the general population suggests an out-of-hospital source of the infection. Despite the number of seroconversions finally occurred in our cohort was small, the awareness of factors associated with a higher risk of acquiring SARS-CoV-2 in a potentially risk environment is crucial to indicate the correct behaviours to adopt inside and outside the working setting, and it might be helpful to cope with the ongoing second wave of the epidemic.
Moreover, and again in line with the findings of other studies,14 15 17–20 23 29 30 we observed a considerable proportion of seropositive subjects (38%) with asymptomatic or paucisymptomatic infection. During the COVID-19 outbreak in Milan, asymptomatic HCWs were not screened in order to reduce the risk of outbreaks at work, and PCR testing of NPS was only used in the presence of symptoms; from our findings, it cannot be inferred if the benefits of periodic screening for SARS-CoV-2 among HCWs, in the case of well-trained personnel and a continuous supply of PPE, outweigh the costs.
Finally, it is interesting to note that a large proportion (40%) of our seronegative study participants reported symptoms compatible with SARS-CoV-2 infection at some time during the study, a finding that is similar to that of Brandstetter et al.31 This may have been due to the simultaneous spread of respiratory infections other than SARS-CoV-2 during the winter/spring, seasonal allergic disorders and/or psychological distress, but a number of false negative results cannot be excluded. Moreover, it has recently been demonstrated that subjects with a history of asymptomatic or mild COVID-19 show SARS-CoV-2 specific T cell responses in the absence of specific antibodies,32 thus suggesting the wider spread of infection despite the absence of a detectable humoural response.
Our study has some limitations. Although representative of our hospital’s occupational categories, the sample was not randomly enrolled and therefore our findings may not reflect true prevalence as a potential selection bias cannot be excluded; however, the longitudinal study of a large number of voluntary participants does provide important information concerning the dynamics of SARS-CoV-2 seroconversion among HCWs and the factors associated with it.
Second, it is difficult to follow subjects exposed to the intense workload, shift work and stressful environment characterising the peak phase of the epidemic in our hospital (and many others); however, only a few of the participants with gaps in their follow-up (4/71) were hospitalised (one) or quarantined (three), and this is unlikely to have introduced biases in the seroprevalence data.
Finally, although the performance of the ELISA we used is good, the accuracy of commercially available SARS-CoV-2 antibody tests requires further validation in the setting of paucisymptomatic and asymptomatic SARS-CoV-2 infection.
In conclusion, the longitudinal sampling of HCWs in a referral hospital for patient with COVID-19 in Milan revealed an increase in the seroprevalence of SARS-CoV-2 antibodies at the time of the peak of the epidemic, but this was less than that observed in other city hospitals14 15 and probably reflects the prompt and effective reorganisation of our hospital and the implementation of infection control measures as the seroconversions seemed to be related to extrahospital contacts. The detection of SARS-CoV-2 antibodies in a relatively high number of asymptomatic HCWs highlights the need for the regular surveillance of asymptomatic HCWs in order to protect both staff and patients from possible nosocomial transmission, particularly if strict adherence to infectious diseases control measures and continuous training in the use of PPE cannot be ensured. Further longitudinal serological studies would help to clarify the quality and persistence of SARS-CoV-2 specific immunity among HCWs.
Data availability statement
Data are available on reasonable request. Anonymised participants data were collected in a protected database and are available on reasonable request from LM (laura.milazzo@asst-fbf-sacco.it) and ALR (annalisa.ridolfo@asst-fbf-sacco.it).
Ethics statements
Ethics approval
The study was approved by hospital’s ethical committee (
Comitato Etico Interaziendale Area 1 DDG n. 453/202) and conducted in compliance with Good Clinical Practice guidelines and the Declaration of Helsinki.
Acknowledgments
We would like to thank all the HCWs who have worked tirelessly on the frontline and agreed to participate to this study by providing their samples and questionnaires. We would also like to thank the Hospital Medical Management for their support.
References
Footnotes
Contributors LM and AL designed the study and wrote the manuscript; AL and AB performed the serological analyses; LP, FC and DM carried out the survey on the healthcare workers (HCWs); CM organised the communication to the HCWs and their periodical calls; LO performed statistical analysis; MC was involved in planning the conceptual idea; MG and SA supervised the work and critically revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.