Article Text

Abstract
Objectives Since 2000 the European Industrial Minerals Association’s Dust Monitoring Programme (IMA-DMP) has systematically collected respirable dust and respirable quartz measurements from 35 companies producing industrial minerals. The IMA-DMP initiative allowed for estimating overall temporal trends in exposure concentrations for the years 2002–2016 and for presenting these trends by type of mineral produced, by jobs performed and by time of enrolment into the DMP.
Methods Approximately 32 000 personal exposure measurements were collected during 29 sampling campaigns during a 15-year period (2002–2016). Temporal trends in respirable dust and respirable quartz concentrations were studied by using linear mixed effects models.
Results Concentrations varied widely (up to three to four orders of magnitude). However, overall decreases in exposure levels were shown for the European minerals industry over the 15-year period. Statistically significant overall downward temporal trends of −9.0% and −3.9% per year were observed for respirable dust and respirable quartz, respectively. When analyses were stratified by time period, no downward trends (and even slight increasing concentrations) were observed between 2008 and 2012, most likely attributable to the recent global economic crisis. After this time period, downward trends became visible again.
Conclusions Consistent and statistically significant downward trends were found for both exposure to respirable dust and respirable quartz. These downward trends became less or even reversed during the years of the global economic crisis. To our knowledge, this is the first time that analyses of long-term temporal trends point at an effect of a global economic crisis on personal exposure concentrations of workers from sites across Europe.
- occupational exposure
- temporal trends
- respirable dust & respirable quartz
- dust monitoring
- industrial minerals
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- occupational exposure
- temporal trends
- respirable dust & respirable quartz
- dust monitoring
- industrial minerals
Key messages
What is already known about this subject?
Occupational exposure to respirable crystalline silica (RCS) has been proven to result in silicosis and lung cancer.
A new binding occupational exposure limit (OEL) for RCS (0.1 mg/m³, 8 hours) has recently come into force in Europe.
The body of literature regarding long-term temporal trends of occupational exposures to respirable dust and respirable quartz within the industrial minerals producing sector is limited.
What are the new findings?
Within the industrial minerals sector, enormous variability in respirable dust and respirable quartz exposure concentrations appeared to be present, up to three to four orders of magnitude.
Over the full period of the study, statistically significant downward trends were observed for both respirable dust and respirable quartz.
Exposure to respirable dust and respirable quartz were in 2016 considerably lower than in 2002 for all jobs and (almost all) minerals.
During the global economic crisis between 2008 and 2012, the downward temporal trends came to a halt and even (somewhat) reversed. After 2012, temporal trends in respirable dust and respirable quartz started to decline again.
How might this impact on policy or clinical practice in the foreseeable future?
By further investigating and improving current situations with elevated exposure levels, the European Industrial Minerals Association’s Dust Monitoring Programme (IMA-DMP) will be instrumental in order to demonstrate compliance with the recently introduced new European OEL and its potential lowering in the (near) future.
IMA-DMP will enable estimation of valid and precise quantitative exposure–response curves in human observational (epidemiological) studies.
Introduction
Occupational exposure to respirable crystalline silica (RCS) can result in developing pulmonary tuberculosis,1 chronic obstructive pulmonary disease,2 silicosis3 and lung cancer.4 Two decades ago, the International Agency for Research on Cancer (IARC) classified RCS as carcinogenic to humans (Group 1) based on sufficient evidence that exposure to RCS is causally associated with an increased risk for lung cancer (IARC 1997).5 IARC upheld the Group 1 classification in its most recent re-evaluation of RCS in 2012.6
In 2017, the European Parliament and Council set a new binding occupational exposure limit (OEL) for RCS dust at 0.1 mg/m³ (respirable fraction, 8-hour time-weighted average).7 This new limit value serves two purposes: to improve workers’ health protection by reducing occupational exposure to RCS and to create more harmonised EU-wide protection of workers against carcinogens.6 In comparison, the EU Scientific Committee on Occupational Exposure Limits8 recommended a health-based limit of 0.05 mg/m³ in 2003. The US Occupational Safety and Health Administration’ final rule on RCS, published in 2016, established two standards—one for the construction industry and one for general industry and maritime,9 which came into effect in 2017 and 2018, respectively. Both standards require employers to protect worker from RCS exposures above the recently established permissible exposure limit of 0.05 mg/m3, averaged over an 8-hour shift.9
In 2000, a discussion was started within the European Industrial Minerals Association (IMA-Europe) to address the need to monitor occupational exposure to respirable dust and in particular to RCS in the dust within its member companies. IMA-Europe is mainly composed of small-sized and medium-sized enterprises, but also includes some of the world’s leading international companies. The 500 mineral member companies operate more than 700 mines and quarries and 750 plants throughout Europe. IMA-Europe represents the European producers of andalusite, bentonite, borates, calcium carbonate, cristobalite, diatomite, dolomite, feldspar, kaolin, kaolinitic clays, lime, mica, quartz, sepiolite, talc, vermiculite and wollastonite. A prospective IMA-Europe Dust Monitoring Programme (IMA-DMP) was initiated to build a body of statistically reliable data that could be used in discussions with authorities about future OEL setting and which would be suitable for future epidemiological studies.10 This, still ongoing, initiative also allowed participating companies to check compliance with OELs set by regulatory authorities at the European level and in the respective countries, to identify hotspots with high exposures and to implement further control measures where needed. In a recent editorial on the need for more exposure surveillance in the field of occupational health, the IMA-DMP initiative was referred to as an outstanding example.11 At the start of the project, predominantly sites of companies in Western Europe participated in the IMA-DMP. More recently, from 2010 onward, also sites from Eastern Europe, Russia, Turkey and Ukraine enrolled into the programme. At present, the IMA-DMP database contains the largest number of occupational personal exposure measurements of respirable dust and RCS (quartz) collected systematically within a single industrial sector.10 The body of literature regarding (recent) long-term temporal trends in occupational exposures to RCS is small. Within the US silica sand industry, a clear annual downward trend in quartz exposure of 11% per year for the period 1946–1996 has been reported.12 In China, for the years 1950 to 1987, exposures to total dust and respirable silica were assessed in 20 mines and 9 pottery factories. Downward trends in quartz exposure of 5% and 7% per year were seen for total dust and RCS, respectively.13 A recently published study showed an 8% annual downward trend in exposure to respirable RCS in the Australian mining sector for the years 1986–2014.14 The multicentre SYNERGY study (pooled analysis of case-control studies on the joint effects of occupational carcinogens in the development of lung cancer) showed decreasing quartz concentrations by 6% per year across a wide range of industries predominantly in Europe over almost three decades (1976–2009).15 Data from measurements made in British quarries between 1984 and 2004 and included in the SYNERGY study also showed annual average respirable dust levels decline with 6% per year, but corresponding quartz levels decreased at a much slower rate of 1.2% per year.15
From the start of the IMA-DMP project, the importance of a common protocol and a well-defined measurement strategy was seen as a necessity. In addition, quality control criteria were introduced to obtain representative and reliable exposure data.10
The objective of this analysis of measurement data collected within the IMA-DMP was to estimate temporal trends in exposure to respirable dust and respirable quartz for workers within the European minerals industry over a 15-year period from 2002 to 2016. The detailed information present in the database allowed to analyse these trends by type of mineral produced, by (standardised) job performed and by time of enrolment into the DMP. Changes in these long-term trends due to global macroeconomic developments were studied as well.
Materials and methods
IMA-DMP database
The longitudinal prospective IMA-DMP exposure database contains personally measured respirable dust and respirable quartz concentrations. Measurements used for the analyses reported here were taken during 33 sampling campaigns between winter 2000/2001 and winter 2016/2017. The respirable dust and quartz exposure data originated from 163 sites owned by 35 companies located in 23 European countries. Companies in Belgium, Denmark, Finland, France, Germany, Greece, Italy, The Netherlands, Norway, Portugal, Spain, Sweden, Switzerland and the UK participated from the start (2002) and were defined as ‘original participants’. Companies or sites in Austria, Bosnia, Czech Republic, Hungary, Poland, Russia, Slovakia, Turkey and Ukraine joined the project later (from 2010) and are designated as ‘recent participants’. In our previously published paper,10 we have described in detail the organisational structure within IMA-DMP. Briefly, the company-specific exposure data are sent to IRAS-UU and, after meeting rigorous quality criteria, entered into the central IMA-DMP database. The data are not publicly available and are not shared between companies in order to maintain confidentiality. Yet, results of statistical analyses of pooled data are being discussed during biennial debriefing with Occupational Health and Safety representatives from the participating companies. More details of the IMA-DMP database (as it existed per 1 May 2015) can be found in the same paper.10 For the temporal trend in respirable dust and respirable quartz analyses, a selection was made of measurements present in the exposure database as per 1 July 2017 (31 760 respirable dust and 27 148 respirable quartz measurements).
Our a priori exclusion criteria are presented in figure 1. In short, measurements with extreme concentrations (>100 mg/m3 for respirable dust and >10 mg/m3 for respirable quartz), most likely due to measurement procedure errors, tampering with samples or extreme conditions were considered outliers and excluded. Also, measurements with a sampling duration shorter than 4 hours and longer than 10 hours were excluded. Exposure measurements with missing ‘worker ID’ data were excluded. In addition, the first three campaigns (campaigns 1–3) and the most recent campaign (campaign 33) were excluded because of limited amounts of data available in these campaigns, leaving data from 29 sampling campaigns for analyses. Consequently, the temporal trend analyses considered 25 539 respirable dust and 22 593 respirable quartz measurements collected between summer 2002 and summer 2016 during 29 campaigns, which amount to 80% and 83%, respectively, of the data present in the database per 1 July 2017.

Flow chart of exclusion criteria applied within the European Industrial Minerals Association’s Dust Monitoring Programme (IMA-DMP) database.
As described previously,10 a standardised common protocol was developed in 2000 and submitted to each of the participating companies. This protocol included all requirements related to how the measurements for the IMA-DMP should be performed. Briefly, personal measurements had to be collected per specific site-job-campaign combination. A unique worker code had to be registered to identify monitored workers. To avoid interlaboratory differences, internal and (accredited) external laboratories are supposed to participate in an interlaboratory round-robin exercises. To what extent this is common practice in the involved laboratories is unclear. Complementary information concerning type of minerals mined or used in the production processes was collected at enrolment and later when new companies and sites entered the programme. The sampling devices had to be either personal respirable dust cyclones with a filter or multifraction samplers containing a sized-selective foam matrix. All samplers used had to be in conformity with the European standard EN-481 (NEN-EN481, 1993).
Appropriate correction factors were applied to account for differences in sampling and analytical efficiency between samplers. The corrections were based on published ratios from different field and experimental studies. The derived correction factors are shown in online supplementary material 1. Quartz concentrations had to be determined with either X-ray diffraction or Fourier transform infrared spectroscopy.
Supplemental material
Imputations
Three thousand two hundred six of 25 539 (13%) respirable dust measurements and 6306 of 22 593 (28%) respirable quartz measurements resulted in concentrations below the limit of detection (LoD). To prevent overestimation of measures of central tendency and underestimation of variability in exposure concentrations, we resorted to multiple imputation techniques for concentrations below the LoD following the method described by Jin et al .16 The imputation was repeated 20 times, creating 20 datasets in order to take into account uncertainties in imputed data.
Linear mixed models to describe temporal trends
Measured exposure concentrations appeared to be log-normally distributed. Therefore, all statistical analyses were carried out on log-transformed concentrations. Linear mixed effect models to estimate temporal trends were elaborated using the PROC MIXED procedure in SAS software V.9.4. In the mixed model, the hierarchical structure of the data was taken into account. Collected repeated measurements on individual workers were nested within job titles, which were consequently nested within a site. A mixed model was fitted with fixed effects for temporal trend (sampling campaign) and random effects of site, job title nested within a site and a random effect worker within job title within a given site. The model can be described as follows:
Ysjwd = β0 + β1Campaign + αs + αsj + µsjw + εsjwd
where Ysjwd=the log-transformed exposure concentration measured on day d=1, 2, …, d, for worker w=1, 2, …, w, in a job title j=1, 2, …, j, at site s=1, 2, …, s;
β0=true underlying mean of log-transformed exposure (intercept);
β1Campaign=fixed effect per sampling campaign (temporal trend);
αs=random effect of site s;
αsj=random effect of job title j within site s;
µsjw=random effect of worker within job title j within a site s; and
εsjwd=random day-to-day effect for day d for worker w within a job title j within site s.
The linear mixed modelling was repeated 20 times and the results were summarised by using SAS procedure MIANALYZE. The temporal trends obtained from the mixed models were expressed as percentages temporal change per sampling campaign (half-year period). Stratified analyses were carried out by job title, by type of mineral and by three time periods (2002–2008, 2008–2012 and 2012–2016).
In our attempts to analyse macroeconomic effect, especially the effect of the global economic crisis, we stratified the data in three time periods; before (2002–2008), during (2008–2012) and after (2012–2016) the global economic crisis.
Additionally, cubic spline models were used to visualise the temporal trends in a less restricted (non-linear) manner. Five knots at the campaigns 6 (2003), 13 (2006), 21 (2010), 26 (2013) and 31 (2015) were placed. The restricted cubic splines models were fitted in SAS using Frank Harrell’s17 macro %RCSPLINE to create the spline terms in the mixed model.
Results
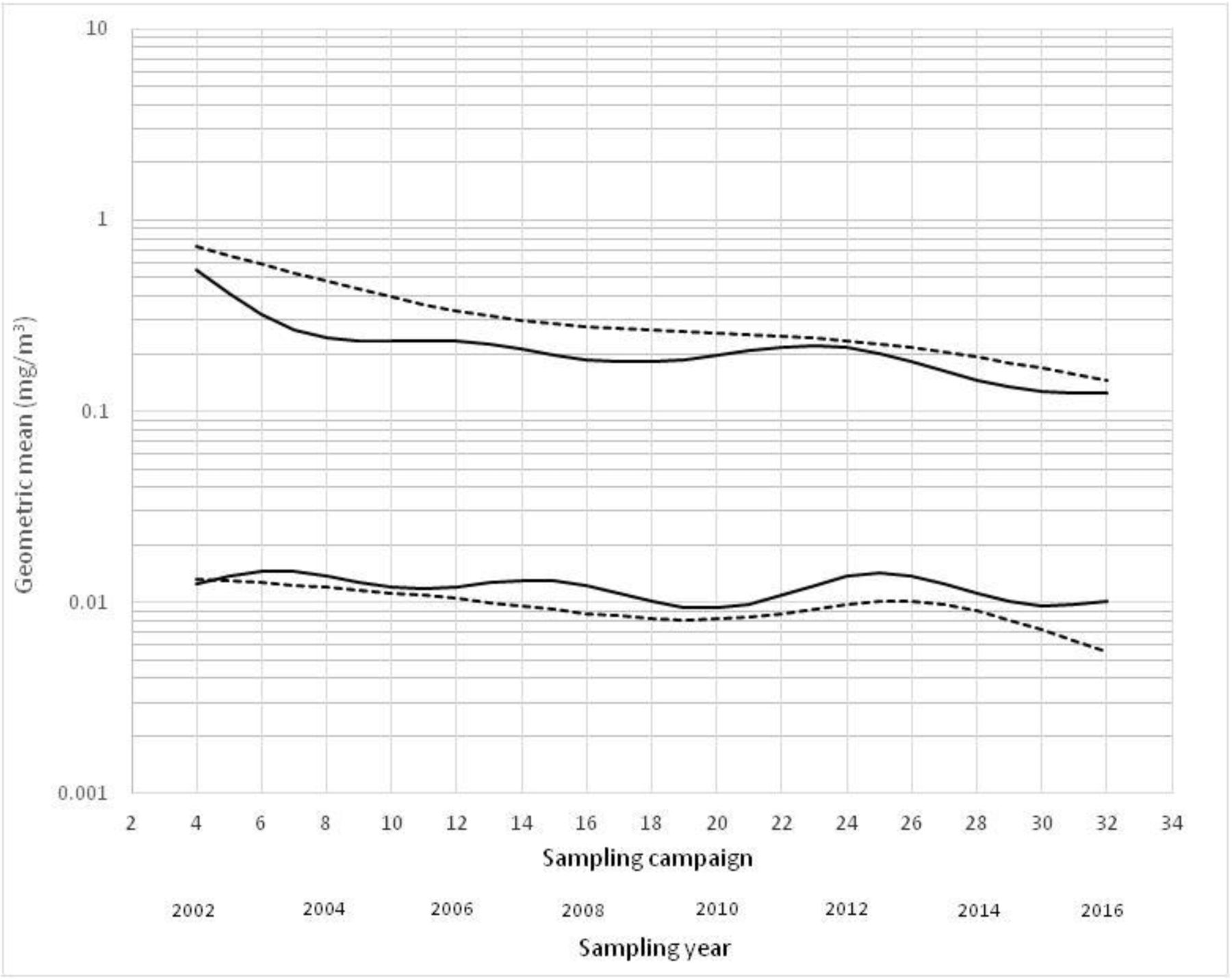
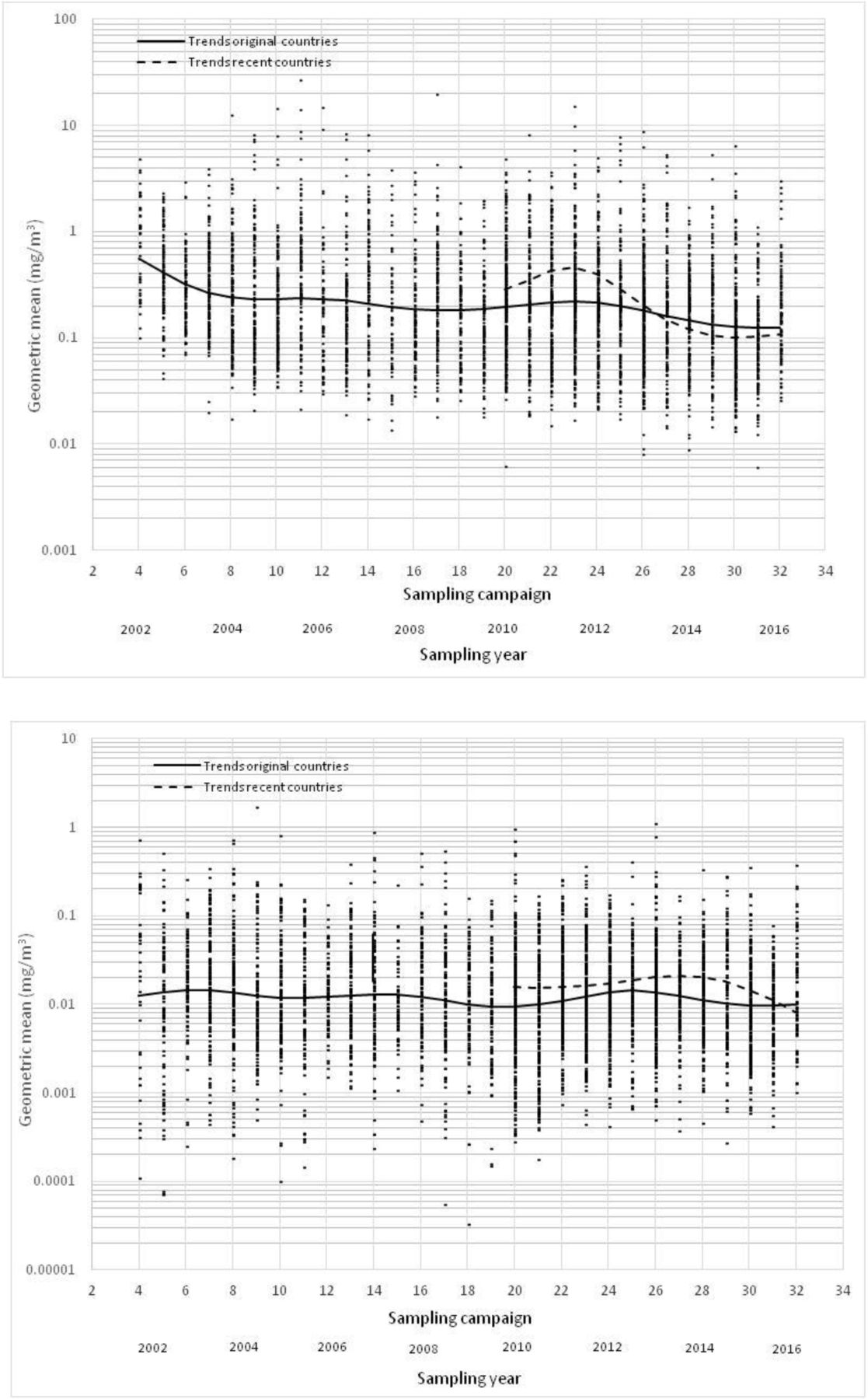
The estimated geometric means for a specific job at a specific site during a specific sampling campaign were plotted against sampling campaign, as shown in figure 2A,B. Figure 2A shows that geometric mean respirable dust concentrations per job per site per campaign varied over three orders of magnitude from 0.01 to 10 mg/m3. Geometric mean respirable quartz concentrations per job per site per campaign varied even more at four orders of magnitude from 0.1 to 1 mg/m3 (figure 2B).

(A) Unadjusted temporal trends in geometric mean respirable dust concentration (mg/m3). (B) Unadjusted temporal trends in geometric mean respirable quartz concentration (mg/m3).
An unadjusted spline was plotted through the median geometric means respirable dust and respirable quartz concentrations, showing the trends in exposure levels over time. We estimated two separate curves for the original and more recent participants in the IMA-DMP. The curves for respirable dust and quartz for the original participants in figure 2A,B show an overall downward temporal trend in median geometric mean concentration over the 15-year period. The median respirable dust concentrations decreased roughly fourfold from 0.52 mg/m3 in 2002 to 0.12 mg/m3 in 2016. The median respirable quartz concentration declined less steeply about twofold from 0.018 mg/m3 in 2002 to 0.009 mg/m3 in 2016.
The trend for respirable dust in figure 2A suggests a steep decline in concentration levels in the first few years of the project. However, this downward trend reversed in 2008 and even started to increase slightly until 2012, after which it started to decrease again. Figure 2B suggests the same phenomenon for respirable quartz where an overall decrease in exposure over the full period of 15 years is interrupted by a short period of increase in exposure between 2008 and 2012. Sites enrolled recently had clearly higher exposure levels in 2010, compared with original sites participating already for 10 years in the IMA-DMP. These differences in exposure levels between original and recent participating countries were no longer discernible in 2016.
Table 1A shows the number of sites and observations for all, original and recent participating countries. In addition, estimated geometric means in 2002, 2010 and 2016 and estimated temporal trends, obtained from a linear mixed model adjusted for site and job, are presented in table 1A. Overall, we found statistically significant, consistent downward temporal trends of −4.6% and −2.1% per sampling campaign (which translates to −9.0% and −3.9% per year) over the 15year period for respirable dust and respirable quartz, respectively.
Estimated geometric means (mg/m3) and temporal trends per campaign for respirable dust and respirable quartz concentrations, (A) overall, (B) per job and (C) mineral produced, adjusted for random effects of site, job and worker
Similar statistically significant consistent downward temporal trends were found for the sites enrolled from the start of the dust monitoring programme from whom 95% of data in the IMA-DMP database originated. However, for site and job, adjusted temporal trends estimated for the recently enrolled sites (between 2010 and 2016) suggested an increase in exposure levels by +1.6% and+5.6% per sampling campaign for respirable dust and respirable quartz, respectively. Both of these trends, however, were not statistically significant due to the still limited amount of collected data and large variability.
Temporal trends and geometric means were estimated for each job and each mineral, as shown in table 1B,C. For respirable dust, statistically significant consistent downward temporal trends per campaign were found for all jobs (table 1B). These trends ranged between −2.9% for ‘crusher’ to −8.4% for ‘plastification worker’. Statistically significant temporal trends for respirable quartz were also observed for almost all jobs (except for the ‘crusher’). They ranged from −10.1% for ‘plastification worker’ to −1.3% for ‘quarry worker’. In general, the downward temporal trends for respirable dust were steeper than for respirable quartz for all jobs except for ‘plastification worker’.
For respirable dust, statistically significant consistent downward temporal trends were found for all minerals produced, ranging from −2.0% for ‘talc’ to −7.3% per campaign for ‘mixed minerals’, as can be seen in table 1C. Downward trends for respirable quartz were statistically significant except for ‘kaolin’, ranging from −0.9% for ‘silica’ and −4.7% for ‘clay’. Again, as noted for jobs, temporal trends estimated for respirable dust were steeper than trends for respirable quartz.
Estimated time trends per time period adjusted for site and job sampled are presented in table 2. For measurement sampled between 2002 and 2008, we found downward temporal trends of −7.4% and −4.0% per campaign for respirable dust and respirable quartz, respectively. During the period (2008–2012), only a slight downward temporal trend was visible for respirable dust (−1.8% per campaign). For respirable quartz, the temporal trend was actually reversed with increasing exposure concentrations during those years (+4.1% per campaign). For the most recent years (2012–2016), decreasing temporal trends were apparent again for both respirable dust and quartz of −7.1% and −8.7% per campaign, respectively. All these trends and differences in trends between the periods were statistically significant (online supplementary material 2) . These changes in trends appeared to be consistent when we performed these analyses stratified by region and size of workforce (data not shown).
Estimated temporal trends per campaign for respirable dust and quartz exposures for three time periods adjusted for random effects of site, job and worker
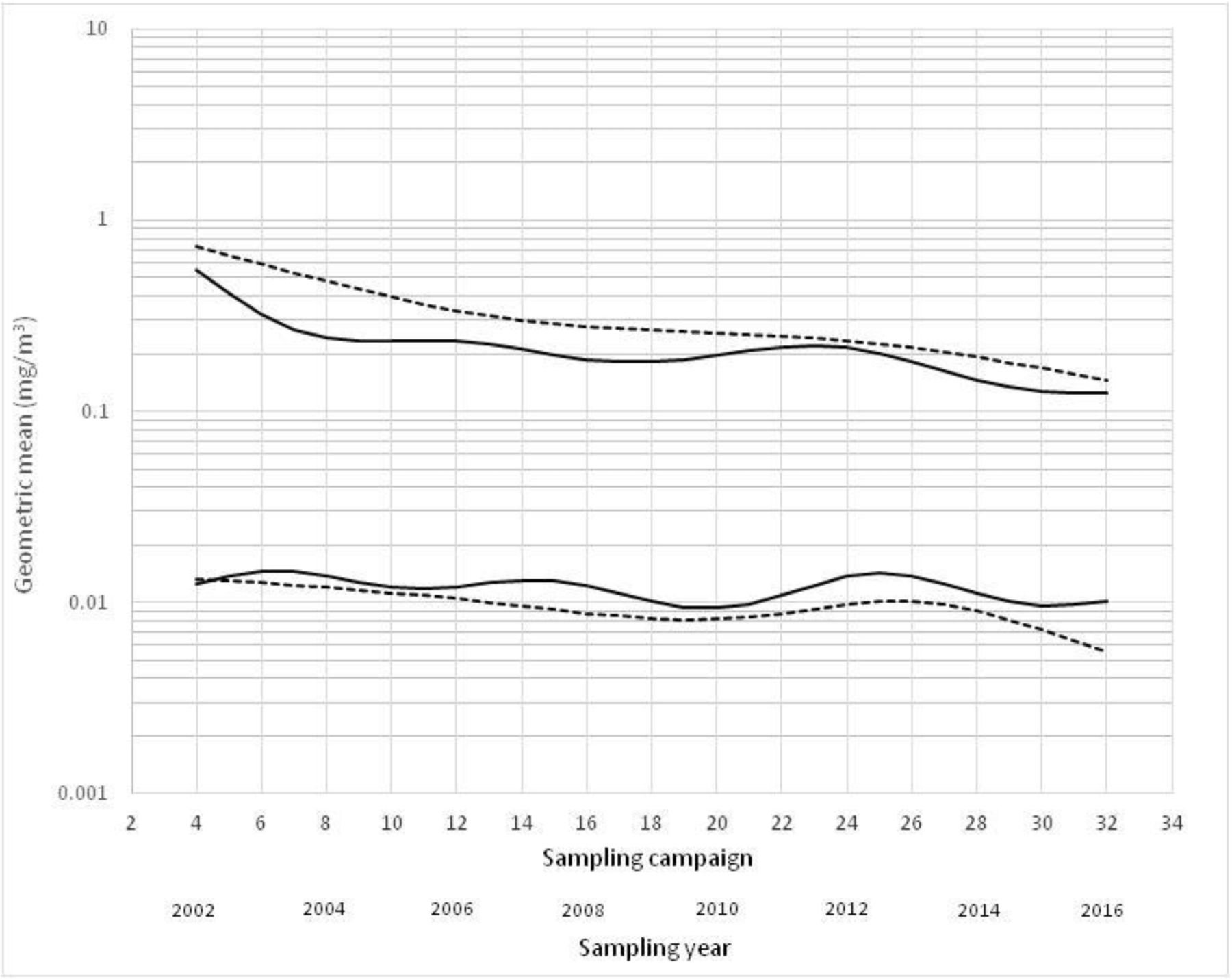
Figure 3 shows both the unadjusted splines (as presented in figure 2A,B) and the adjusted (for site and job) splines for both respirable dust and respirable quartz. Over the 15 years of the project, the unadjusted and adjusted time trends look comparable; with an overall consistent decline in respirable dust and respirable quartz exposures. However, between 2008 and 2012, there is a slight difference between unadjusted and adjusted time trends especially for respirable dust. The adjusted time trends showed a levelling off trend where the unadjusted time trends showed an increase in respirable dust exposure levels. For respirable quartz, both unadjusted and adjusted time trends showed similar patterns.
{kind=link}
{kind=link}
{kind=link}
Temporal trends of respirable dust (upper) and respirable quartz concentrations (lower) (mg/m3), unadjusted (solid line) and adjusted for random effects of site, job and worker (dotted line).
Discussion
This study examined the temporal trends in exposure to respirable dust and respirable quartz within the European minerals industrial sector, based on almost 32 000 personal exposure measurements obtained over a 15-year period and collected within the IMA-DMP database. It is considered to be representative for the sector and allows for an in-depth analysis of personal exposure to respirable dust and respirable quartz in this sector.
Key findings
For site and job, adjusted temporal trends showed an overall significant decrease in exposure levels within the European minerals industry over the 15-year period. Statistically significant and consistent downward temporal trends were observed for respirable dust and respirable quartz. The trends were more steeper for respirable dust than for respirable quartz at −9.0% versus −3.9% per year. When stratification was done according to time of enrolment, temporal trends in sites recently enrolled (predominantly from eastern European countries) in the dust monitoring programme showed after adjustment for site and job non-significant upward trends since 2010 for respirable dust and respirable quartz concentrations. Differences in level of exposure and trends between European regions (west vs east) have been reported previously.18
Consistent downward temporal trends were observed for all jobs and for (almost all) minerals produced for both respirable dust and respirable quartz. However, during the years 2008–2012, the downward temporal trends for respirable dust came to a halt, and even reversed for respirable quartz, indicating temporal trends were disrupted by the economic recession faced by most European countries.
IMA-DMP data quality
The standardised common protocol and strict quality criteria within IMA-DMP allowed this detailed analyses and provide detailed insight into these temporal trends. Although our results are more or less in keeping with other studies where exposure levels appeared to be declining over time, bias due to different sampling strategies applied will not have been an issue in our study (except for using different sampling devices where we could adjust for). Important limitations of most previously reported exposure trends studies were lack of a common measurement protocol and standardised measurement strategies to ensure comparability of exposure data over time and across countries.19 20 For instance, within the SYNERGY study it was not possible to adjust for measurement strategy-related factors, which the authors claimed could have resulted in considerable uncertainty and bias in the estimates for RCS exposure per region and might have affected the estimates of temporal trends.15 The availability of the IMA-DMP standardised common protocol, however, did not prevent the increasing number of measurements below the LoD as a result of declining concentrations respirable dust and respirable quartz. Therefore, more imputations had to be performed in order to end up with unbiased estimates of average exposures and to prevent underestimation of variability in exposure concentrations.16 Another aspect that could have resulted in bias was the use of various respirable samplers and analytical methods. We assume, however, that the effect of using different samplers will have been small, because we were able to apply correction factors based on a number of comparison studies of sampler efficiencies in wind tunnel and field conditions (online supplementary material 1). Although these correction factors were based on a relatively small number of studies, they showed consistent patterns and allowed us to derive correction factors enabling unbiased comparison of respirable dust and respirable quartz concentrations from different countries.
Differences in temporal trends between respirable dust and quartz
Temporal trends were adjusted for site and job, because not every site, job and individual worker were measured during any given campaign. It became clear that the adjusted splines showed considerable differences in overall temporal trends between respirable dust and respirable quartz, with trends being steeper for respirable dust than for respirable quartz. Given the stronger temporal downward trend for respirable dust, we hypothesise that quartz must be more prevalent in the smaller fraction of the respirable dust and hence more difficult to control. This is confirmed by Huggins et al 21 who found that quartz particles appeared to be predominantly present in the range between 0.6 and 1.5 µm at metal and non-metal mine and plant sites. Also, Page stated that with average dust particle size decreasing, the percentages of quartz were increasing.22
The splines after adjustment indicated somewhat higher concentrations for respirable dust but lower for respirable quartz when compared with unadjusted splines. Sites participating longer in the IMA-DMP with more observations in the database had relatively lower respirable dust concentrations but higher respirable quartz concentrations than sites with fewer observations. Adjusting for site therefore resulted in higher respirable dust but lower respirable quartz concentrations.
Comparison of temporal trends with the literature
In line with our study, the SYNERGY study showed an overall annual decrease in quartz exposure levels over almost three decades (1976–2009) across a wide range of European industries,15 but the reported −6% per annum is somewhat steeper than seen within the IMA-DMP at almost −4% per annum. The industry, within the SYNERGY project, most comparable to our study was the British quarry industry. It showed a slower decrease in respirable dust exposure of −6% per annum between 1984 and 2004, based on 2937 measurements, than we did (−9%). Like in our study, the corresponding quartz concentrations decreased at a slower rate of −1.2% per annum.15 Our findings concur also with other studies that previously reported downward trends for respirable dust (−5%)13 and quartz (−11%),12 (−7%),13 (−6%)23 and (−10%)24 within several industries worldwide.
In our study, temporal changes varied from job to job. The ‘plastification worker’, for instance, showed the steepest decline in respirable dust and respirable quartz concentration. This was not surprising given the very high concentrations for this job at the beginning of the DMP. The second highest exposed job was the ‘bagging worker’. Watts et al reported these workers having the highest exposure to quartz in metal and non-metal mining.25 Anderson et al also showed that bagging jobs historically tended to have the greatest quartz exposures.26 Interestingly, in the study of Anderson et al , quarry and wet process workers had the lowest exposures and these findings are also in line with our results. In another study conducted within the American industrial sand industry, very significant reductions in respirable quartz over time (1970–2010) were described for most work processes and activities including bagging operations and wet processing.27
Macroeconomic developments affecting temporal trends
Our study indicates that the overall downward temporal trends in exposure to respirable dust and respirable quartz were not constant over the full period of 15 years. The observed changes in temporal trends could be associated with global economic developments. Especially between 2008 and 2012, the downward temporal trends came to a halt and in the case of quartz even slightly reversed. The recession started around 2008–2009 and in this industry had resulted in downsizing of workforces resulting in more diverse (including more dusty) tasks and potentially less time for good housekeeping in the workers still employed. In addition, cutting costs might have also resulted in delayed or less maintenance of ventilation (replacement of filters), or delayed investments in control measures and new machinery. Comparable non-linear time trends were also visible in the ExpoSYN exposure database due to macroeconomic changes in the early 1980s and early 2000s.28 In another study, based on dust measurements in Russian asbestos mines, dust concentrations increased after a period of decrease due to political and economic reform in the late 1980s and early 1990s.29 Lack of financial resources to repair machines and invest in new ones or to install or maintain control measures resulted in higher exposures to dust.29
The decrease in exposure concentrations within the IMA-DMP might have been the result of direct feedback to companies in the form of company reports prepared after each sampling campaign. These reports helped companies to identify and intervene in hotspots where exposures are not in compliance. Recently, Basinas et al showed in a randomised intervention study that feedback on measured concentration as such could reduce exposure levels among farmers already by 20%–30%.30 It is most likely that decrease in exposure concentrations within the IMA-DMP has occurred due to increased awareness of presence and health effects of RCS and resulting changes in behaviour during task performances among the involved workers. Basinas et al concluded that reductions in dust exposure levels among farmers most likely resulted from changes in working style and changes in behaviour during task performances.30 Also, Peters et al reported that decreasing exposure levels to respirable quartz are likely a result of awareness around health effects of RCS, modifying mining practices and advanced control measures.14 In addition, proper housekeeping and prevention of leakages (or spillages) could play a substantial role in reducing exposure levels in the working environment. Cherrie et al suggested technological changes in production processes, availability of improved equipment and stronger national legislation as main drivers for reducing exposure levels.31 Several control measures within the European mineral industry sector have been implemented to reduce the exposure levels, including automation of bagging lines, introduction of fogging systems and enclosure of bagging installation.32 To evaluate the effects of interventions, provisions for standardised collection of information on control measures have recently been incorporated in the IMA-DMP database.
Conclusions
Significant downward trends were found for both exposure to respirable dust and respirable quartz over a 15-year period. The value of the IMA-DMP database has been proven by showing precise estimates of trends in concentrations over time and it enables accurate estimation of exposure to respirable dust and quartz for multiple sites, jobs and minerals produced for different time periods across Europe.
To our knowledge, this is the first time that analysis of temporal trends point at an effect of a global economic crisis on measured personal concentrations in sites across Europe. It can be hypothesised that this industrial sector was not unique in this respect. By further investigating and improving current situations with elevated exposure levels, the IMA-DMP database will be instrumental for the mineral industry to be able to meet the recently introduced European OEL, be ready for future limits and provide accurate exposure estimated for future human observational studies.
Acknowledgments
The authors gratefully thank the participating companies and their employees all across Europe for their cooperation by submitting measured personal data and the exchange of insights at the biennial debriefing meetings.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors HZ collected the exposure data from the European Industrial Minerals Association’s Dust Monitoring Programme (IMA-DMP) database, performed the statistical analyses and drafted the manuscript. RH and HK manage the IMA-DMP database, designed the study, provided guidance for statistical analyses and critically reviewed the manuscript. All authors have read and approved the final version of the manuscript.
Funding We gratefully acknowledge the funding of this project by the Industrial Minerals Association Europe (IMA-Europe). The funder had no involvement in the analysis and interpretation of the data, in the writing of this manuscript and the decision to submit the paper for publication. All authors contributed to the interpretation of the results and all approved the final version before submission.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are not available due to confidentiality requirements.