Article Text

Abstract
Objective The aim of our study was to investigate the acute effect of night work during pregnancy on the risk of calling in sick the following day using register-based information and the workers as their own controls.
Methods Using the payroll-based national Danish Working Hour Database, including all public hospital employees in Denmark, we identified 9799 pregnant women with ≥1 day shift and ≥1 night shift and ≥1 day of sick leave during the first 32 pregnancy weeks from January 2007 to December 2013. We performed fixed effects logistic regression, that is, within-worker comparisons, of the risk of sick leave of any duration starting within 24 hours after night shifts of different length versus day shifts.
Results Most of the participants were nurses (64%) or physicians (16%). We found an increased relative risk of sick leave following night shifts compared with day shifts during all pregnancy trimesters. The risk was highest for night shifts lasting >12 hours (OR 1.37, 95% CI 1.15 to 1.63 for nurses; OR 1.87, 95% CI 1.69 to 2.08 for physicians) and among women aged >35 years (OR 1.42, 95% CI 1.24 to 1.63).
Conclusion Among Danish public hospital employees night shifts during pregnancy, especially shifts longer than 12 hours, increased the risk of calling in sick the following day independent of personal factors and time-invariant confounders in all pregnancy trimesters.
- shift work
- female reproductive effects and adverse pregnancy outcomes
- sickness absence
- sick leave
- night work
Statistics from Altmetric.com
- shift work
- female reproductive effects and adverse pregnancy outcomes
- sickness absence
- sick leave
- night work
Key messages
What is already known about this subject?
Shift work during pregnancy may be associated with increased risk of sick leave. However, prior studies presented crude assessment of working schedules, lack of pregnancy period-specific analysis, information bias and healthy worker selection.
What are the new findings?
Among Danish public hospital employees, night shifts during pregnancy, especially shifts longer than 12 hours, increased the risk of calling in sick the following day independent of personal factors and time-invariant confounders in all pregnancy trimesters.
How might this impact on policy or clinical practice in the foreseeable future?
If pregnant women work at night, reducing the frequency and duration of night shifts in the organisation of their working schedules may reduce sick leave during pregnancy.
Introduction
A high prevalence of long-term (>14 consecutive days) sick leave among European pregnant workers has been demonstrated.1–3 The primary reason for that seems to be pregnancy-related but a mismatch between pregnancy and work, for instance work-family conflicts, workload and reproductive occupational hazards,4–7 and different polices for sick leave during pregnancy across countries also play a role.3 Women not covered by paid sick leave during pregnancy might have higher threshold for calling in sick due to economic challenges. Recently published studies found that nearly 10% of the women with long-term sick leave during pregnancy reported work-related reasons for sick leave.1 3
Shift work during pregnancy has in Danish studies been associated with an increased risk of long-term sick leave, including a dose-effect relationship with increasing number of night shifts.1 5 8 9 To our knowledge, there are no studies on short-term (≤14 consecutive days) sick leave during pregnancy. It is possible that short-term and long-term sick leave during pregnancy in relation to night work might involve different factors, but this is yet to be elucidated.
One of the mechanisms connecting night work with sick leave involves fatigue and disturbed sleep, both sleep length and quality, leading to lack of recovery.10–13 Härmä and colleagues found, in a recently published study, that night shifts were associated with fatigue, both during work and free days, altered sleep length and difficulties to fall asleep.14 In a 2-year prospective cohort of truck drivers, need for recovery after work predicted sick leave of >14 days.15 The acute effect of night shifts, including night shifts lasting up to 12 hours, on sleep and fatigue among healthcare workers has been shown in epidemiological and field studies.16–19 There is, however, a lack of studies on health effects of night shifts longer than 12 hours.
Crude assessment of working schedules, lack of pregnancy period-specific analysis, information bias and healthy worker selection challenge the results from prior studies. Furthermore, sick leave is closely related to personal factors, which is an important source of bias in comparisons between individuals.
We aimed to investigate the acute effect of night shifts of different length during pregnancy on the risk of calling in sick within 24 hours after a shift regardless the duration of sick leave. We hypothesised that night shifts lead to lack of recovery and where increased the risk of sick leave in the subsequent day. The novel aspects of our study are the register-based assessment of exposure and outcome, and within-worker comparisons in a prospective design.
Methods
Design
We conducted a prospective nationwide register-based cohort study using the participants as their own controls. We used information from two Danish national registries linked on the individual level via the civil registration number given to all residents in Denmark since 1968.
The Danish Working Hour Database (DWHD), a national payroll database covering more than 250 000 employees in the Danish administrative regions including all public hospital employees, provided the source population. It includes daily information on time of start and end of shifts and all types of paid and unpaid leave, job title and place of employment from January 2007 to December 2015.20 Information on pregnancy and covariates was identified from The Danish Medical Birth Registry, which contains information on all births in Denmark since 1973.21
Study cohort
The study cohort was retrieved from the same source population as in a recently published study.22 In short, it comprised 42 485 women from the DWHD who gave birth at least once during from January 2007 to December 2013, giving a total of 60 482 pregnancies. We excluded women≤18 and ≥50 years (n=15), multiple pregnancies (n=2957) and pregnancies conceived in 2006 (n=6403), because they lacked payroll data, and thereby exposure data, from conception to January 2007. Further, we excluded pregnancies if employment in one the administrative Regions of Denmark, and therefore registration in the DWHD, started after conception or ended before 32 pregnancy weeks (n=16 570) to ensure that payroll data were available throughout the first 32 pregnancy weeks. We conducted fixed effects analysis, which requires change in both the exposure and the outcome for each participant.23 Therefore, the study population comprised women with both ≥1 day shift, ≥1 night shift and ≥1 day of sick leave during the first 32 pregnancy weeks (n=23 024 excluded). Finally, each woman contributed with only their first pregnancy occurring during the study period (n=1714 pregnancies excluded), leaving 9799 women eligible for analyses (online supplementary figure).
Supplementary file 1
Exposure
Risk days were days with a DWHD registration other than maternity leave, vacation, unpaid leave and compulsory day off preceded by a day or a night shift within a 24-hour period.
Shifts during the first 32 pregnancy weeks, including on-call shifts, lasting ≥3 hours were defined as day (start time after 06:00 and end time before 21:00) or night (any start and end time including any duration of working hours between 23:00 and 06:00) corresponding to 84% of all registered shifts, the rest being evening or early morning shifts. The duration of night shifts was defined as ≤8 hours, >8–12 hours or >12 hours (long night shifts).
Outcome
The outcome was defined as a DWHD registration of sick leave lasting ≥3 hours. Registrations with consecutive dates of sick leave were collapsed with the date of the first and last registration defining the duration of the sick leave period.
Registrations coded as ‘exacerbated pregnancy symptoms’ or ‘pregnancy complications’ (pregnancy leave) were used for descriptive purposes to assess the total absence during pregnancy. They reflected pregnancy leave mostly due to medical complications and not ordinary sick leave. Administrative procedures for registration of pregnancy leave differ from registrations of sick leave, and they vary across the five administrative Regions of Denmark. Registrations of pregnancy leave were therefore not appropriate to investigate the risk of calling in sick within 24 hours after a shift. The combined effect of both sick leave and pregnancy leave was investigated in sensitivity analysis.
Demographic characteristics
Age (<30, 30–35, >35 years), body mass index (BMI, <25, 25–29, ≥30 kg/m2), parity (1, 2, ≥3) and smoking (non-smoker, former smoker, smoker) registered by the midwife or family doctor at the first antenatal visit were retrieved from The Danish Medical Birth Registry.
Classification of socioeconomic status (SES) into high, low or medium was derived from Statistics Denmark and was based on DISCO-88, the Danish version of the International Standard Classification of Occupations from 2007 to 2009 and 2010–2013 (ISCO-88 and DISCO-08), respectively.24 25
We considered age, BMI and occupation as potential effect modifiers. The reason for the latter is that different occupations have different organisations of working schedules and work content, that is, different tasks and workload.
Statistical analyses
We compared the risk of sick leave of any duration starting within 24 hours after night shifts of different length versus day shifts during the first 32 pregnancy weeks using the participants as their own controls. We performed fixed effects logistic regression to account for repeated measures within workers. This statistical method requires that each participant has change in both the exposure and the outcome, as it in praxis, answers the question: ‘Does a change in the exposure cause a change in the outcome?’.23 Results were presented as ORs with 95% CIs.
For interaction analysis with age, BMI and occupation, we used a likelihood ratio test comparing models with and without the interaction term. As nurses and physicians represented most of the cohort, we limited stratified analyses to these occupations. We performed sensitivity analyses restricted to nulliparous women and using both sick leave and pregnancy leave as the outcome.
We used two-tailed tests with a significance level of 0.05. All analyses were done with the SAS V.9.4 software (SAS Institute, Cary, North Carolina, USA).
Results
The study cohort comprised 9799 women contributing to 474 338 risk days. Around 65% were nurses and 16% physicians. Table 1 presents the participant’s personal and working time characteristics. Of all shifts included in the analyses, 82% were day and 18% night shifts. Nurses and physicians had similar number of night shifts, while physicians had more day shifts than nurses (table 1). Around 42% of the night shifts lasted ≤8 hours, 35% lasted >8–12 hours and 23% lasted >12 hours. The proportion of long night shifts was 7% among nurses and 99% among physicians (table 1). These differences reflect different collective agreements for nurses and physicians in Denmark.26 27 Nurses had more than twice as many days of absence during the first 32 pregnancy weeks (mean 34.4, median 17.0, SD 38.9) than physicians (mean 15.7, median 6.0, SD 25.9) (table 1). Nearly 18% of the women in the study cohort had 1–3 days of absence; 17% had 4–7 days and 8–14 days, respectively; 13% had 15–28 days and 35% had >28 days of absence during the first 32 pregnancy weeks (figure 1). Around 33% (n=3 264) of the cohort had at least one period lasting >14 days. This distribution was similar to that observed among 20 912 pregnant women from the same source population with ≥1 shift of any type during the first 32 pregnancy weeks (data not shown). We observed large differences in the duration of periods of pregnancy leave compared with sick leave. Registrations of pregnancy leave lasted on average 44 days (median 33.0, SD 40.3), being 60% of the periods>14 days and were observed for half of the study cohort (n=4976), mainly during the second and third trimesters. These women had slightly higher proportion of overweight and obesity and of medium and low SES compared with the rest of the cohort. Sick leave periods lasted on average 9.1 days (median 6.0, SD 11.9), were equally distributed throughout pregnancy and only 5% of the periods lasted >14 days.
Characteristics of 9799 pregnant public hospital employees* in Denmark, 2007–2013

Distribution of total days of absence, including sick leave and pregnancy leave, during the first 32 pregnancy weeks among 9799 public hospital employees* in Denmark, 2007–2013. *Workers with ≥1 day shift and ≥1 night shift and ≥1 day of sick leave during the first 32 pregnancy weeks.
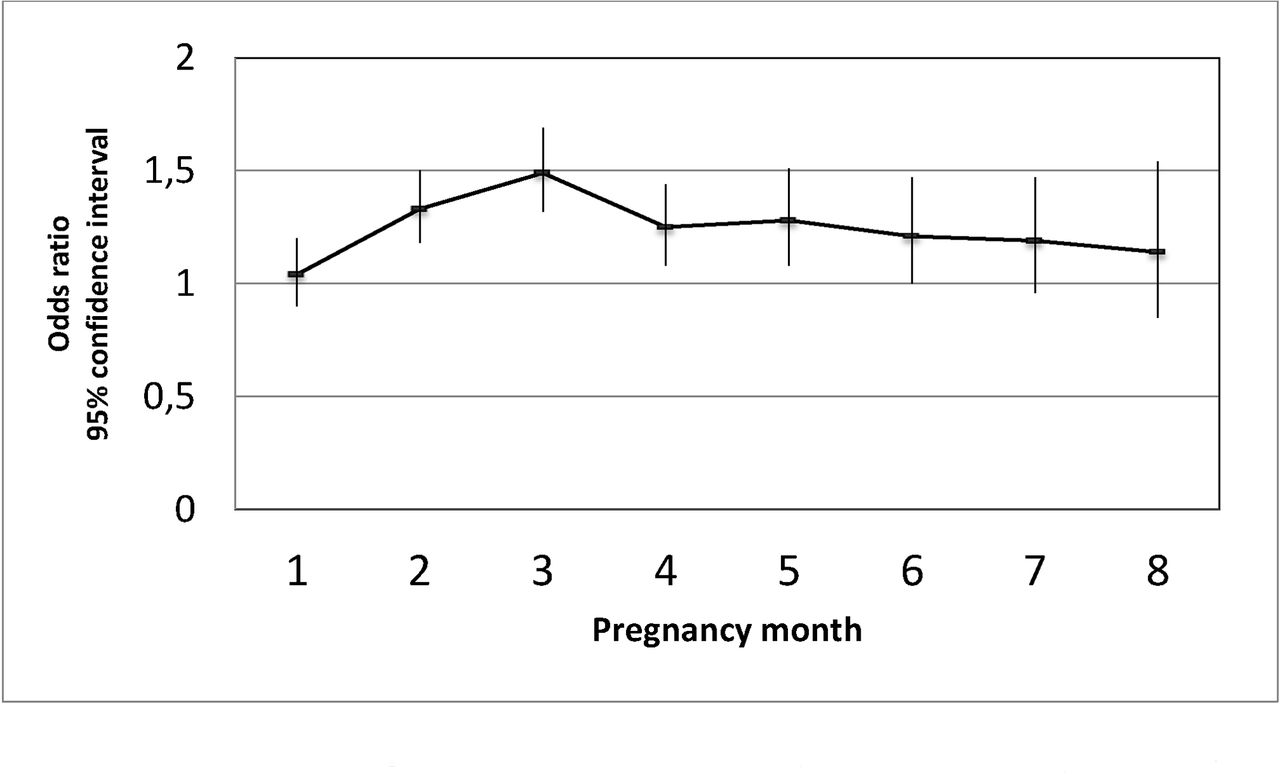
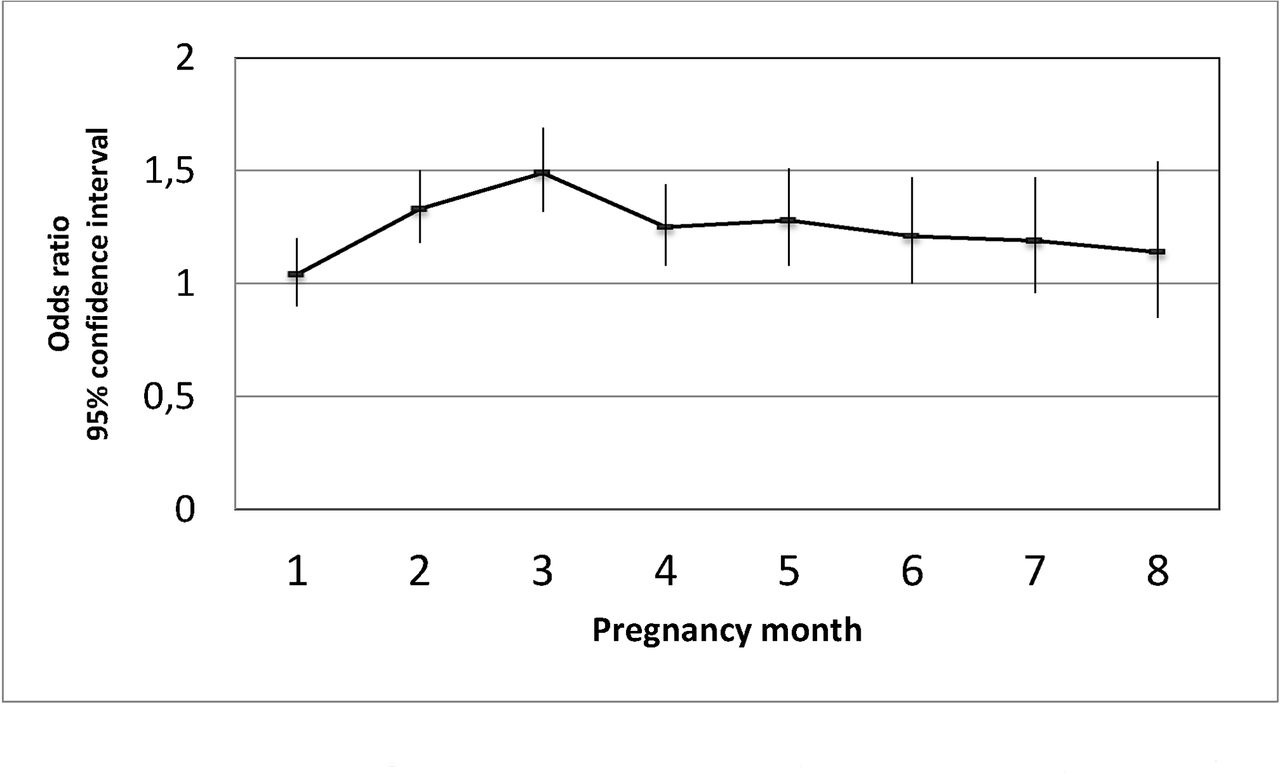
We found increased OR of calling in sick within 24 hours after night versus day shifts in all pregnancy trimesters (OR 1.28, 95% CI 1.19 to 1.37 in the first trimester; OR 1.27, 95% CI 1.17 to 1.39 in the second trimester and OR 1.13, 95% CI 0.96 to 1.31 in the third trimester)—see table 2. Physicians presented the highest estimates (OR 1.94, 95% CI 1.67 to 2.27; p value for multiplicative interaction with occupation<0.0001). Figure 2 presents stratification by pregnancy month for the whole cohort. The overall risk during the first 32 pregnancy weeks was OR 1.23, 95% CI 1.17 to 1.29.
![[SP1.jpg]](https://oem.bmj.com/content/oemed/76/3/163/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Risk of calling in sick, regardless of duration of sick leave, within 24 hours after night versus day shifts during the first 32 pregnancy weeks stratified by pregnancy month with the participants as their own controls* among 9799 public hospital employees† in Denmark, 2007–2013. *Fixed effects logistic regression. †Workers with ≥1 day shift and ≥1 night shift and ≥1 day of sick leave during the first 32 pregnancy weeks.
Risk of calling in sick, regardless of duration of sick leave, within 24 hours after night versus day shifts during the first 32 pregnancy weeks with the participants as their own controls* among 9799 public hospital employees† in Denmark, 2007–2013
The association between night shifts and the risk of sick leave was modified by age (p value for multiplicative interaction 0.03) but not by BMI (p value for multiplicative interaction 0.32). The OR of sick leave following night shifts was 1.42 (95% CI 1.24 to 1.63) among women older than 35 years; 1.25 (95% CI 1.17 to 1.35) among women aged 30–35 years and 1.16 (95% CI 1.08 to 1.25) among women younger than 30 years.
The effect of night shifts on the risk of calling in sick within 24 hours following night shifts was driven by night shifts lasting >12 hours (OR 1.55, 95% CI 1.43 to 1.69 among all women; OR 1.37, 95% CI 1.15 to 1.63 among nurses and OR 1.87, 95% CI 1.69 to 2.08 among physicians)—see table 3. Analysis of night shifts of ≤8 and>8–12 hours among physicians revealed relatively higher estimates, but they were based on quite few shifts (table 3).
Risk of calling in sick, regardless of duration of sick leave, within 24 hours after night shifts of different length compared with day shifts during the first 32 pregnancy weeks with the participants as their own controls* among 9799 public hospital employees† in Denmark, 2007–2013
Sensitivity analyses either restricted to nulliparous women (n=5095) or with both sick leave and pregnancy leave as the outcome slightly attenuated the estimates, mainly during the second and third trimesters (data not shown), but the effects observed in the main analyses remained.
Discussion
This is to our knowledge the first study of the acute effect of night work on sick leave during pregnancy presenting trimester-specific estimates and applying a statistical method that accounts for personal and time-invariant factors. We found that night shifts, especially long shifts, are a risk factor for calling in sick within 24 hours after the shift in all pregnancy trimesters.
Our findings are in accordance with prior Danish studies showing an increased risk of sick leave during pregnancy among shift workers.1 5 8 Similar to our cohort, Kaerlev and colleagues investigated hospital employees (n=773).8 They used roster data on job tasks and sick leave and questionnaire information on working schedules. They found that night or shift work was a risk factor for sick leave corresponding to >10% of the scheduled work time (OR 1.4, 95% CI 1.0 to 1.9 adjusted for age, occupation, full-time or part-time job and previous sick leave). Using data from the Danish National Birth Cohort from 1996 to 2002, Hansen et al investigated occupational exposures in relation to sick leave during pregnancy among 51 874 women.5 They included primarily sick leave periods of >15 days from the Danish Register for Evaluation of Marginalisation (DREAM). Information on working schedules was based on an interview conducted between 17 and 30 pregnancy weeks. They found an increased risk of sick leave among women with shift work including night shifts (HR 1.61, 95% CI 1.42 to 1.83), and a trend of increasing risk with increasing number of monthly night shifts (HR 1.89, 95% CI 1.67 to 2.15 among women with >8 night shifts per pregnancy month). Last, sick leave of >20 days was reported more frequently by women who worked evening and/or night shifts during pregnancy in a survey of 508 women.1
The rate of 33% of the women in this cohort having at least one period of absence lasting >14 days is also in line with prior Scandinavian studies.1 2 5 7 8 However, considering that our cohort did not include women on sick leave throughout pregnancy, either those with fixed night, fixed evening or with fixed day shifts, it is possible that this rate is underestimated.
Our findings of higher risk of sick leave following night shifts during first trimester may be partly explained by selection out of night work, into either other working schedules or into long-term sick leave, by women experiencing pregnancy complications. Such a change of working schedules happens usually during the end of the first trimester, when many Danish women inform their workplace about their pregnancy. Figure 2 illustrates this by the increasing relative risk of calling in sick within 24 hours after night shifts during the first trimester followed by a relative decrease during the second and third trimester. It is important to notice that we did not investigate the cumulative risk of sick leave during pregnancy. Our analyses included only women who were at work and had a change of both exposure (≥1 day shift and ≥1 night shift) and outcome (≥1 day of sick leave) in the respective pregnancy trimester. As rates of sick leave are known to increase throughout pregnancy,6 8 women who continue working night shifts until the third trimester are probably healthier.28 It was therefore not surprising that the risk of calling in sick after a night shift in our study was higher in the first pregnancy trimester, that is, before the healthy worker selection has occurred. Nevertheless, even women who worked night shifts until the third trimester (n=8382), in our cohort, were at increased risk of sick leave after a night shift. This is, probably, because night work at this point may add to the effects of insufficient sleep and fatigue physiologically imposed by late pregnancy. It is also important to keep in mind that sick leave during pregnancy in relation to night work might also be associated with other potentially more severe disorders than fatigue.22 29–33
Analysis restricted to nulliparous women revealed attenuated estimates. It is known that first time pregnancies are at increased risk of certain complications, such as hypertensive disorders.34 However, women who experienced complications in prior pregnancies might be more cautious and where have a lower threshold to call in sick in subsequent pregnancies.
We also observed attenuation of the estimates in analysis including pregnancy leave as the outcome. This was not surprising, as pregnancy leave in our cohort represented mostly medical complications requiring planned and long-term absence. The longer duration of pregnancy leave periods might have contributed to the healthy worker effect later in pregnancy. This is supported by the almost identical results for the first trimester for sensitivity analysis including pregnancy leave (OR 1.27, 95% CI 1.19 to 1.35) and main analysis (OR 1.28, 95% CI 1.19 to 1.37—from table 1), but attenuation of the estimates in the second and third trimesters.
Shift’s characteristics
We found that occupation modified the effect of night work on sick leave. Even though we pursued to disentangle the different dimensions of night work for research purposes, what we observed is a combination of them. The different results observed among nurses and physicians in our cohort might partly be explained by differences in absence rates and in the organisation of shift work. Nurses had higher rates of absence (see table 1), especially during the first trimester, and higher proportion of absence periods lasting >14 days (46%) and >28 days (31%) compared with physicians (27% and 16%, respectively). Consequently, relatively more physicians than nurses contributed to analyses of the second and third trimesters. Furthermore, in Denmark, while nurses tend to have regular 3-shifts schedules, physicians have almost exclusively night shifts longer than 12 hours.26 27 Even though physicians have the possibility of on-call shifts and planned sleeping breaks more frequently than nurses, emergency duties across departments may limit this possibility in praxis. This combined effect of long night shifts and increased workload might aggravate fatigue and insufficient recovery explaining the relatively higher estimates among physicians.
Similarly, the combination of long night shifts with increased workload might explain the effect of night shifts >12 hours on the risk of calling in sick within 24 hours observed for nurses (table 3). Among them, long night shifts occurred mostly when they worked two shifts in a row. Such changes in working schedules reflect frequently increased workload due to, for example, sick leave among colleagues or increased number of patients in a hospital department.
The design of our study was not appropriate to investigate consecutive night shifts and quick returns but they have been negatively associated with several health outcomes35 36 and may also contribute to the effect of night work on sick leave during pregnancy. In a recent published study using the same source population as in the present study, we found that women with longer spells of consecutive night shifts, and among obese women also those with long night shifts and quick returns, during the first 20 pregnancy weeks had increased risk of hypertensive disorders.22 Field studies have shown increasing hormonal dysfunction with increasing number of consecutive night shifts.37–39 Additionally, most of the workers in our cohort have irregularly rotating shifts and do not fulfil the suggested recommendation of at least 2 days off following a night shift to adjust the circadian rhythm back to a day pattern.40
Strengths and limitations
The large sample size, objective and detailed exposure assessment, prospective design and the use of the workers as their own controls are the major strengths of our study. Selection bias due to incomplete coverage was reduced to a minimum due to the nationwide source population. Adequate comparisons of sick leave between individuals are challenging because sick leave is highly correlated with personal factors, such as prior health, threshold for calling in sick and family and work environment.4 The use of within-workers comparisons fully accounts for personal factors and time-invariant confounders. This design has been shown as efficient in other studies of occupational exposures.14 However, fixed effects modelling does not account for time-variant factors, such as work content. This might have induced bias towards the null in our cohort because work tasks vary largely from day-to-day in a hospital, and fatigue is presumably higher following night shifts with increased workload.
Our results are based on a cohort of hospital employees with the majority having unregularly changing schedules nearly weekly. Therefore, our results may not apply for populations with other working schedules. Not including pregnancy leave in the main analysis may have isolated the effect of working schedules on sick leave independently of pregnancy complications, although whether our results apply for non-pregnant women with similar working schedules waits to be proven.
Conclusion
Among Danish public hospital employees, night shifts during pregnancy, especially shifts longer than 12 hours, increased the risk of calling in sick the following day independent of personal factors and time-invariant confounders in all pregnancy trimesters. If pregnant women work at night, reducing the frequency and duration of night shifts in the organisation of their working schedules may reduce sick leave during pregnancy.
Acknowledgments
The Danish administrative regions are acknowledged for the participation and willingness to provide data to the DWHD. Jens Worm Begtrup, Lisbeth Nielsen and Anders Ørberg are thanked for valuable work with data management. Statistics Denmark is acknowledged for ensuring appropriate anonymisation of the data in accordance to the current Danish Data Protection legislation.
References
Footnotes
Contributors PECH, JPB, AHG, EMF, ADL and LMB provided substantial contributions to the conception of the study and the analysis of the data. PECH, AHG and ADL contributed to the acquisition of the data. PECH was responsible for drafting the paper. All authors contributed substantially to the interpretation of the data, the critical revision of the paper for important intellectual content and the final approval of the version published. All authors are accountable for all aspects of the work.
Funding This work was financially supported by The Danish Working Environment Research Fund grant 31-2015-03 2015001705. The establishment of the DWHD has been financed by research grants from The Danish Working Environment Research Fund (grant 23-2012-09), The Nordic Program on Health and Welfare – Nordforsk (grant 74809) and The National Research Centre for the Working Environment. The Danish administrative regions have partially financed the transfer of data to the cohort.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.