Article Text

Abstract
Objective To prospectively study suspected occupational risk factors for amyotrophic lateral sclerosis (ALS).
Methods For this case–cohort analysis within the prospective Netherlands Cohort Study, 58 279 men and 62 573 women aged 55–69 years at enrolment in 1986 were followed up for 17.3 years on ALS mortality. Information on occupational history and potential confounders were collected at baseline through a self-administered questionnaire and entered for a random subcohort (2092 men and 2074 women) and ALS deaths (76 men and 60 women). Occupational exposure to solvents, pesticides, metals, extremely low frequency magnetic fields (ELF-MFs) and electrical shocks was estimated by means of job exposure matrices (JEMs). Associations between ever/never occupationally exposed and cumulative exposure and ALS mortality were analysed by gender using Cox regression.
Results Occupational exposure to ELF-MF showed a possible association with ALS mortality among men: HR for ever holding a job with high exposure versus background 2.19 (95% (CI): 1.02 to 4.73) and HR for the highest tertile of cumulative exposure versus background 1.93 (95% CI 1.05 to 3.55).
Interpretation These results strengthen the evidence suggesting a positive association between ELF-MF exposure and ALS. We did not replicate earlier positive findings for other occupational exposures.
- Electromagnetic fields
- Amyotrophic Lateral Sclerosis
- occupation
- pesticides
- metals
Statistics from Altmetric.com
What this paper adds
Multiple occupational exposures have been hypothesised to be related to amyotrophic lateral sclerosis (ALS), such as extremely low frequency magnetic fields (ELF-MFs), electrical shocks, solvents, metals and pesticides.
Studies on these exposures suffered from one or more methodological shortcomings.
This study, using The Netherlands Cohort Study, improves upon earlier efforts by using a large, prospective, general-population cohort, with complete job histories up to enrolment while testing for multiple occupational exposures.
We observed an association between occupational exposure to ELF-MF and ALS mortality, but not with other occupational exposures.
Introduction
Amyotrophic lateral sclerosis (ALS) is a progressive disease of the motor neuron system, usually resulting in death within 1–6 years of onset.1 Approximately 5%–23% of the cases of ALS are familial, suggesting that environmental exposures may play an important role in the occurrence of ALS.2 A higher prevalence and an earlier onset of ALS has been observed in men compared with women.3 4 Educational level,1 5 smoking,6 physical activity,7 repeated physical trauma,8–10 and various occupational exposures1 11–13 have been postulated as risk factors for ALS. However, current evidence for these behavioural and environmental factors is still insufficient to draw strong conclusions about their relationship with ALS.1
Occupational exposures that have been hypothesised to be related to ALS are extremely low frequency magnetic fields (ELF-MFs), electrical shocks, solvents, metals and pesticides.1 11–14 Studies on these exposures suffered from one or more methodological shortcomings, such as analyses by occupation instead of assessing specific exposures,8 using self-reported exposures instead of more objective exposure measures,15 using only a single job instead of a full occupational history to assess exposure13 16 and a limited ability to adjust for potential confounders.16 17
We aimed to extend the current evidence base and improve on the previous studies by analysing the effects of occupational exposure to ELF-MF, electrical shocks, solvents, metals and pesticides on ALS mortality in a large, prospective, population-based cohort study18 with occupational history information up to baseline, using state-of-the-art job exposure matrices (JEMs) and detailed information on possible confounders.
Methods
The Netherlands Cohort Study (NLCS) on diet and cancer consists of 58 279 men and 62 573 women who were enrolled in 1986.18 At the time of enrolment, subjects were 55–69 years old, lived throughout the Netherlands and completed a self-administered questionnaire on occupational history, dietary habits, lifestyle and other potential risk factors focusing on cancer. The cohort was followed up for cause-specific mortality and cancer incidence. Following a case–cohort approach, person-years were estimated using a randomly drawn subcohort (2411 men and 2589 women). Questionnaires were entered manually for incident cases as well as for the subcohort. Questionnaires were entered blind to case/subcohort status by drawing extra (non-case) questionnaires at random, which were entered simultaneously with the new cases.
The NLCS was approved by the institutional review boards of the Netherlands Organisation for Applied Scientific Research TNO (Zeist) and Maastricht University (Maastricht).
Follow-up and case definition
Vital status for the period from January 1987 to October 2003 was obtained from the Dutch Bureau of Genealogy and the municipal resident registration. Causes of death were obtained from Statistics Netherlands, coded according to the 9th and 10th (since 1 January 1996) edition of the International Classification of Diseases, codes 335.20 and G12.2, respectively. For the current analyses, data were available for 17.3 years of follow-up (from September 1986 to December 2003). In total, 88 male and 70 female ALS deaths (0.15% and 0.11% of entire cohort, respectively) were registered, either as a primary or secondary cause of death. Of these, seven men and two women were also part of the subcohort (0.29% and 0.08% of the subcohort, respectively).
Exposure assessment
The baseline questionnaire contained questions on lifetime occupational history up to time of enrolment in the cohort (ie, when subjects were 55–65 years of age). Subjects reported whether they ever had a paid job, and if so they supplied the name of the company or institution they worked at, the type of company or institution, what was produced at their department, their job title, and period of employment for each job for up to five jobs.
Subjects in the subcohort who ever had paid jobs (n=4344) reported 1.9 jobs on average. Jobs were coded by one designated researcher according to the Dutch occupational classification system developed in 1984 by Statistics Netherlands, based on the industry and occupational descriptions provided by the subjects. These job codes were subsequently translated to the International Standard Classification of Occupations 1988 (ISCO-88) using a crosswalk described previously.19 Occupational exposures were assigned by linking the job histories to various JEMs by ISCO-88 job codes:
ELF-MF: using a recently developed ELF-JEM.20
Electrical shocks: using a recently developed Shock-JEM based on registries of occupational electric injuries.21
Total, aromatic and chlorinated solvents, metals, pesticides, insecticides, herbicides and fungicides: using the ALOHA+-JEM.19 22 23
All these JEMs assign exposure based on intensity and probability of exposure, with the exception of the Shock-JEM, which is based on the probability of workplace electrical injuries. The JEMs were ordinal and had three exposure levels: no (or background), low and high exposure.
The following metrics of occupational exposure were used for each exposure: (1) Ever had a job with at maximum a high, a low or background occupational exposure (hereafter referred to as background, only low or ever high exposure respectively). If there were few exposed cases in a single category (<5), the only low and ever high exposure categories were merged into one category, hereafter referred to as ever exposed. We also tested for trend based on the high, only low and background categories. (2) Cumulative exposure: calculated by first assigning weights to the exposure ratings reflecting the multiplicative nature of occupational exposure distributions (ie, no exposure: 0, low: 1, high: 4), then summing the products of the exposure weights and duration of each job over the entire job history. Subjects who had never had a paid job (eg, homemakers or other, 8% of cases and 6% of subcohort) were assigned background exposure in the main analyses. Subjects for whom all job information was missing (12% of cases and 12% of subcohort) were set to missing.
Statistical analyses
Associations between occupational exposures and ALS mortality were investigated using Cox proportional hazards models with age as the time scale, stratified by sex. Following the case–cohort approach, the number of cases was the number in the entire cohort, whereas the person-time was estimated through the follow-up of the members of the subcohort. 95% CI were calculated using the robust estimator of variance to account for the additional variance introduced by the case–cohort. Censoring occurred at date of death, loss to follow-up or end of follow-up, whichever occurred first. Models were analysed using STATA V.12.1 (Statacorp, College Station, Texas, USA).
The following covariates were included in the risk models based on the literature1: smoking (current vs former and non-smokers), attained level of education (primary vocational vs lower vocational, secondary and medium vocational and higher vocational), body mass index (in kg/m2) and physical activity (in min/day). All these covariates were measured at baseline. Alcohol consumption in the year prior to baseline was also considered as a covariate, but as the evidence for an association with ALS is scarce and alcohol consumption showed no clear association with ALS mortality in the cohort, this confounder was not entered in the final models. Information on occupational history and potential confounders was available for analyses for 76 male and 60 female ALS cases and 2092 men and 2074 women in the subcohort.
The occupational exposure metrics were analysed as categorical variables, using background exposure as the reference category. For cumulative exposure, sex-specific tertiles in the subcohort were used to categorise the exposed individuals. A test for trend was performed based on the medians of the exposure categories.
We first analysed occupational exposures based on the ever/never classification adjusting for attained educational level as a covariate. Depending on whether this analysis showed significant associations, or showed an increasing trend from background to ever high exposed, we further explored exposure-response associations using cumulative exposure. Lastly, if an occupational exposure showed a possible exposure-response association with ALS mortality in the analysis of cumulative exposure, we analysed this exposure while mutually adjusting for the other exposures.
Sensitivity analyses
Two types of sensitivity analyses were performed. First, all subjects with missing exposure levels due to a job history that contained too little information to be coded were assigned to the no/background exposure group instead of being omitted from the analyses. Second, an analysis was performed where subjects who never had a paid job at baseline, that is, homemakers and unemployed, were omitted from the analyses, whereas they were considered to be exposed to background levels in the main analysis.
Results
Table 1 shows the exposure distribution of the selected potential confounders and occupational exposures for men and women in the subcohort and among ALS cases. Cases tended to have a lower level of attained education at baseline compared with the subjects in the subcohort. Forty-four per cent of cases ever had a blue collar job, compared with 38% of the subcohort. Exposure prevalence in the subcohort varied across the different occupational exposures with ever high exposed varying between 2% to 25% for men and 0% to 2% for women (table 1). Due to the overall low number of exposed women, risk analyses for women were largely uninformative and limited to ever/never exposed analyses (see online supplementary figure e-1 and table e-1). Here, we only present the results for men.
Distribution of age, level of education and occupational exposures previously hypothesised to be related to ALS by subcohort and case-status
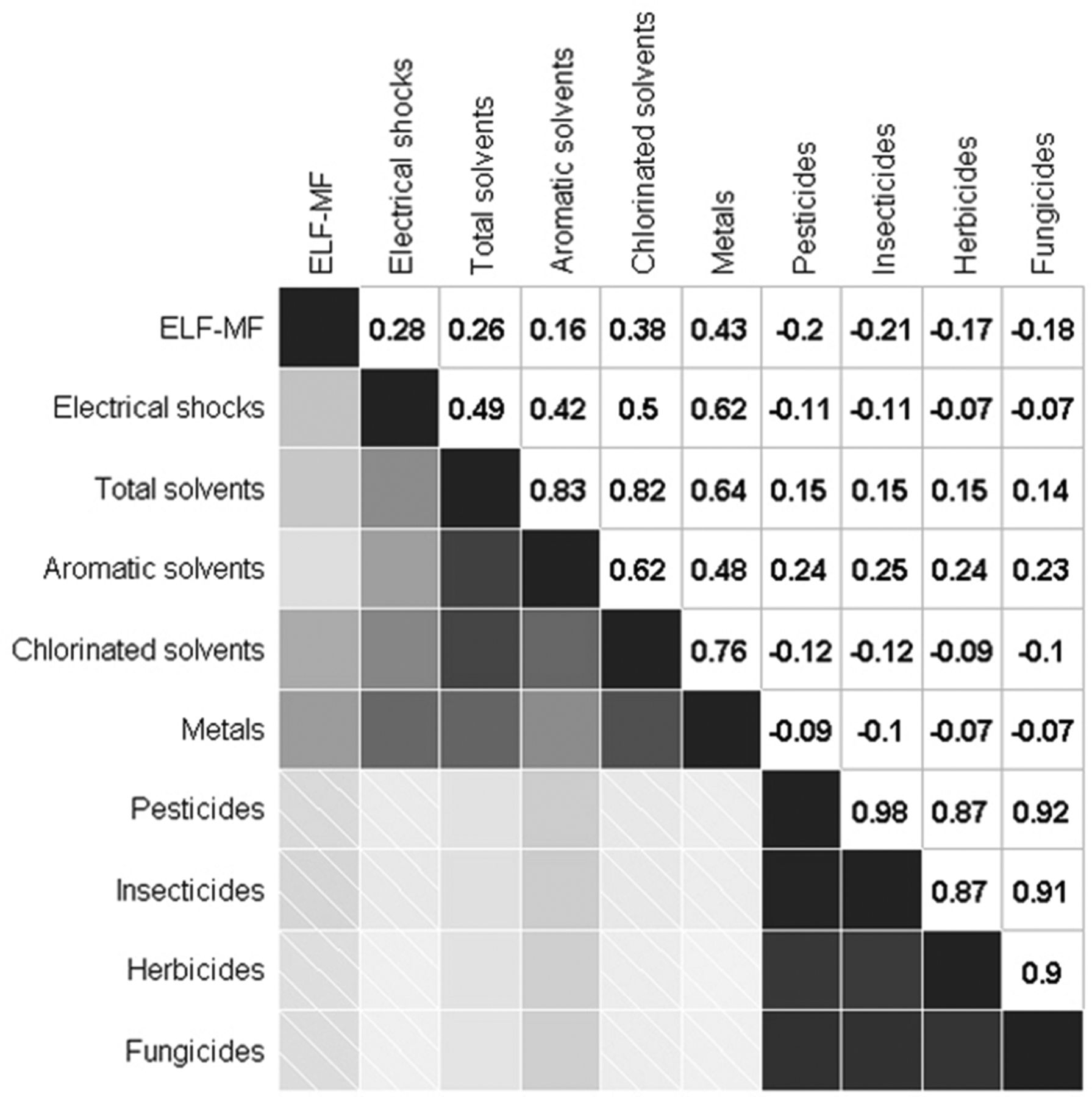
Correlation analyses between the different occupational exposures revealed low to highly correlated exposures. Two main exposure clusters could be identified. One cluster contains ELF-MF, electrical shocks, solvent and metal exposures. The other cluster contains exposure to pesticides, insecticides, herbicides and fungicides (see figure 1).
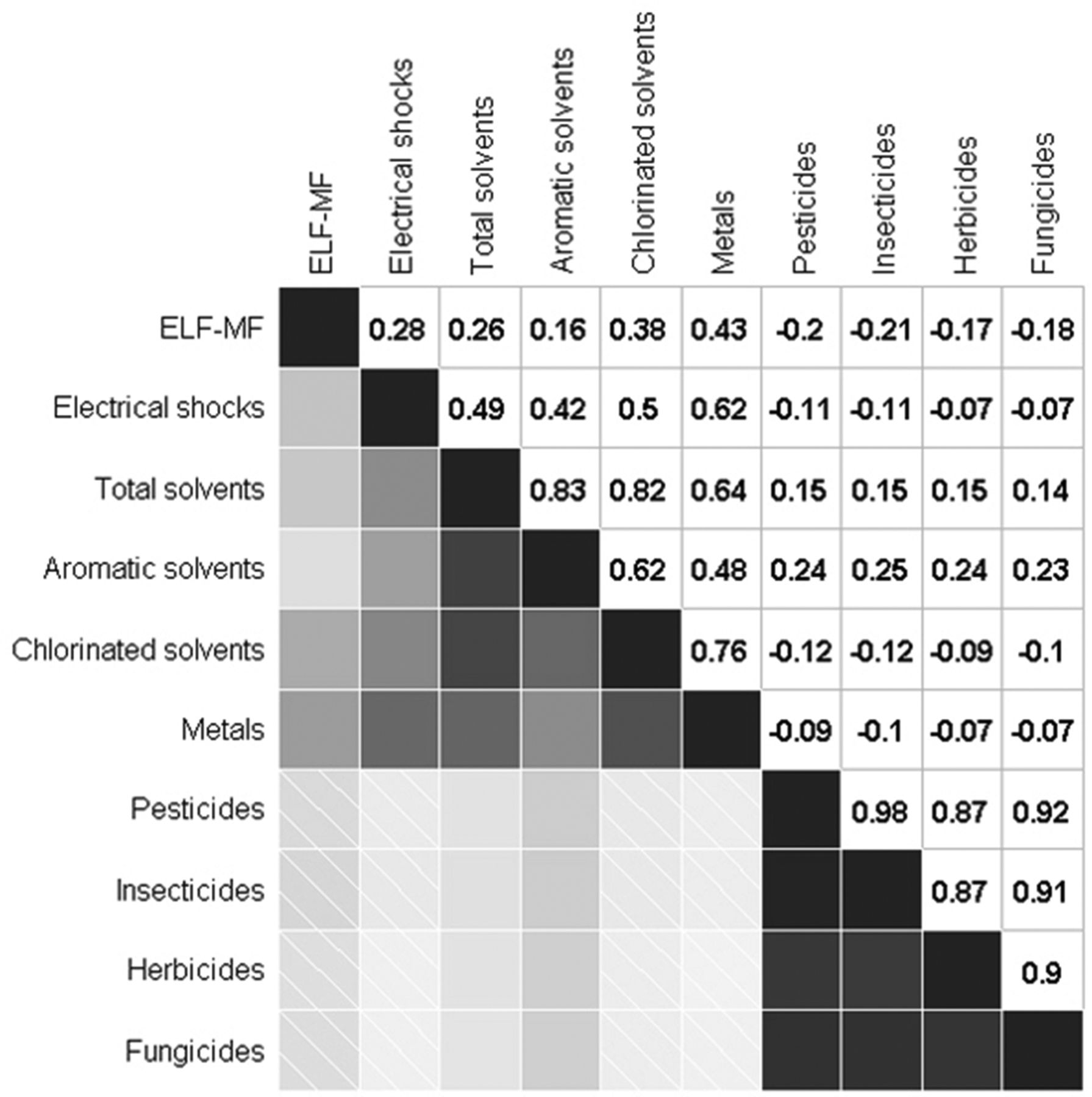
Correlogram displaying the Pearson correlations between cumulative occupational exposures among men in the subcohort. ELF-MF, extremely low frequency magnetic fields. Shaded: negative correlations; smooth: positive correlations; lighter coloring: lower correlation.
Single occupational exposure analyses
In the ever/never exposure analysis (table 2), only ELF-MF showed a significant positive association with ALS mortality among men (adjusted HR (HR) ever high exposure versus background exposure: 2.19, 95% CI 1.02 to 4.73). The association also showed a significant test for trend (p=0.02). Occupational exposure to solvents or metals also showed positive associations, but with wide CIs and without a clear trend. If the low and high exposure categories were merged, the results were comparable (see online Supplementary table e-1). In contrast, exposure to pesticides resulted in negative associations with ALS mortality. However, these analyses were limited by the low number of exposed cases resulting in wide CIs.
Associations between ever/never occupationally exposed to selected agents and ALS mortality in men*
Based on the positive significant association in the ever/never analyses and sufficient exposed cases (n>5) per cumulative exposure category, we analysed the possible association between cumulative exposure to ELF-MF and ALS mortality. The cumulative exposure analysis showed a significant positive association with cumulative ELF-MF exposure and ALS mortality with the third tertile versus background exposure resulting in a significant increased risk of 1.93 (95% CI 1.05 to 3.55) with a positive exposure-response trend across cumulative exposure categories (p=0.02) (table 3).
Association between cumulative occupational ELF-MF exposure and ALS mortality in men*
Combined exposure analysis
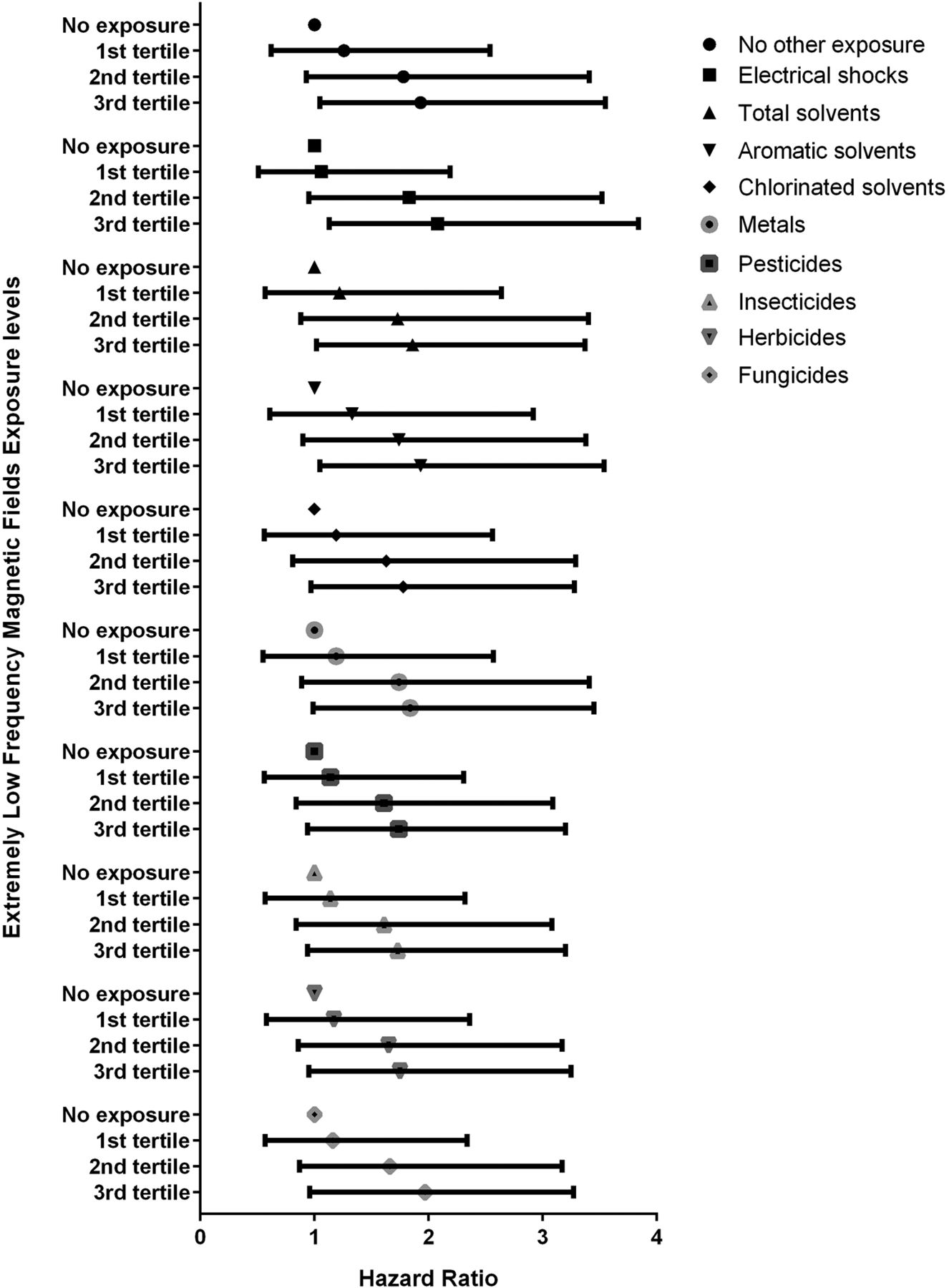
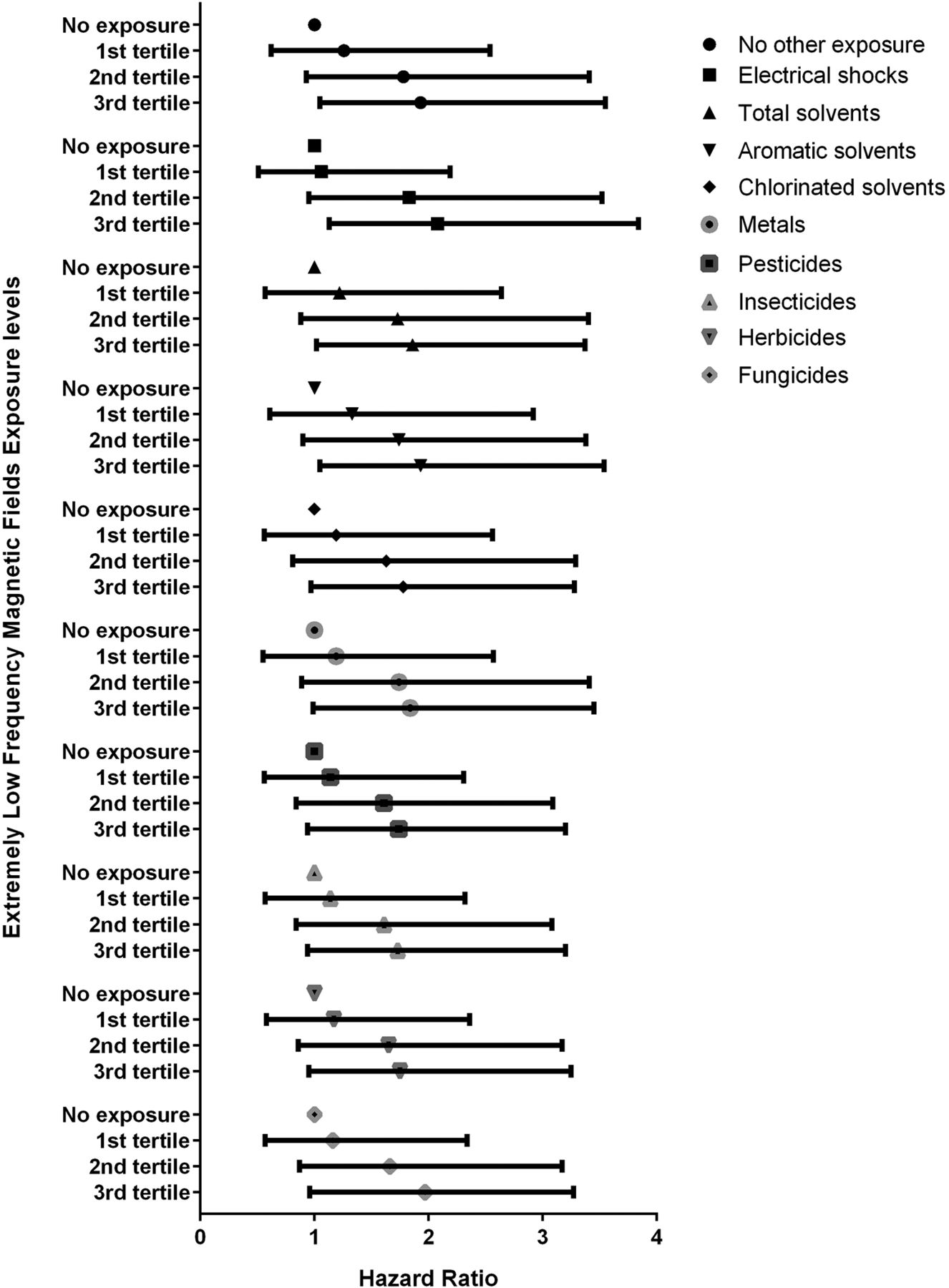
When analysed together with the other exposures, HRs for the third tertile of cumulative exposure to ELF-MF among men changed from 1.93 (95% CI 1.05 to 3.55) in the single cumulative occupational exposure analysis to 1.73 (95% CI 0.94 to 3.20) when analysed together with insecticides and 2.09 (95% CI 1.13 3.84) when analysed together with electrical shocks (see figure 2). In these analyses, none of the other occupational exposures was significantly associated with ALS mortality (results not shown).
{kind=link}
{kind=link}
Associations between cumulative ELF-MF exposure and ALS mortality in men adjusted for other occupational exposure. ALS, amyotrophic lateral sclerosis; ELF-MF, extremely low frequency magnetic field.
Sensitivity analyses
The sensitivity analyses omitting subjects never having a paid job or assigning subjects without detailed occupational exposure to background exposure levels showed only minor changes to the risk estimates obtained in the main analysis and did not result in different conclusions (results not shown).
Discussion
We studied occupational exposures with an a priori hypothesis of being related to an increased ALS risk. Of the 10 selected exposures, only ELF-MF showed a significant and increasing exposure-dependent association with ALS mortality.
Electromagnetic fields and shocks
Previous studies have suggested that so-called electrical occupations are associated with an increased risk of ALS.8 15 24 25 Both exposure to ELF-MF and electrical shocks have been proposed as an explanation for this finding.8 26 However, studies assessing occupational exposure to ELF-MF across occupations have been less consistent than those of electric occupations, with some showing a positive association17 24 27–31 while others did not.16 25 32–34 Industrial cohort studies using more detailed job histories more frequently reported positive associations,17 29 30 whereas general population studies using the job reported on the death certificate16 or jobs at single time points more often reported no associations.25 32
Only few studies have assessed the association of ALS mortality and self-reported electrical shocks.8 15 Deapen and Henderson8 reported increased risks between self-reported electrical shocks producing unconsciousness and ALS incidence. Gunnarson et al 15 found no association between self-reported high-voltage electrical shocks and ALS incidence, although the authors did report an association for ALS with low-voltage electrical shocks in a subgroup aged 45–59 years. Recently, some attempts have been made to assess these associations using JEMs.31 33 34 Of these studies, only Fischer et al 34 provided weak support for an association between occupational exposure to electrical shocks and an increased incidence of ALS. We found no indications for an increased risk of ALS for subjects with a higher risk of injuries due to electrical shocks in the workplace. In contrast, we did observe an exposure-dependent association between ELF-MF exposure and ALS mortality. This would suggest that exposure to ELF-MF rather than electric shocks in electric occupations may drive the observed increased risk of ALS.
Solvents
Exposure to solvents as an overall category has been implicated as a possible risk factor for ALS in earlier epidemiological studies,8 15 but results have been heterogeneous.35 36 Some studies looking at more specific solvents such as chlorinated solvents, glycol ethers37 and formaldehyde38 39 have shown positive associations, although these results have not been replicated.12 39 We found no significant association between occupational exposure to total solvents, chlorinated, or aromatic solvents and ALS mortality. Our study therefore does not support previous findings of an association between occupational solvent exposure, including aromatic and chlorinated solvents and ALS mortality.
Metals
Occupational exposure to lead and mercury has been associated with ALS in previous studies.1 12 40 Some studies have also associated increased levels of lead in plasma with ALS, although other metals have not shown similarly consistent associations.41 42 Assignment of specific metals based on a JEM is difficult, as occupational categories are generally too broad to distinguish between exposures to specific metals. Some studies have found an association between occupational exposure to metals and ALS mortality using this methodology,36 although others did not.43 We used the ALOHA+-JEM to assign total metal exposure, which due to the broad categorisation might not have captured possible associations between specific metals and ALS mortality. While our analyses showed increased HRs for exposure to metals, none were significant. Our study therefore provides little further evidence for an association between occupational exposure to metals and ALS mortality. However, the prevalence of exposure was low. Together with the inability to estimate potential risks associated with exposure to specific metals, we cannot exclude small risks related to specific metals.
Pesticides
Working in agricultural jobs has been indicated as a risk factor for ALS.12 Three meta-analyses on pesticide exposures and risk of ALS concluded that occupational exposure to pesticides increases the risk of ALS in men.11 14 44 Studies included in these meta-analyses generally did not make a distinction between the types of pesticides used precluding the identification of specific pesticides related to ALS risk. A subsequent study, conducted after the meta-analyses, showed no elevated risk of ALS mortality and exposure to pesticides but did show increased risks for several specific pesticides, including exposure to aldrin and dieldrin.14 Malek et al 36 and Yu et al 43 also showed an association between occupational exposure to pesticides and ALS incidence. We found a non-significant, negative association between occupational exposure to pesticides, herbicides or insecticides and ALS mortality. These negative associations were unexpected and offer no further support for an association between occupational exposure to pesticides and ALS within the general population. Due to the low number of exposed cases in the cohort, we had to collapse the high and low exposure categories. Therefore, we also could not investigate possible exposure–response relationships.
Combined exposure analyses
Cumulative occupational exposures to ELF-MF, shocks, solvents and metals showed moderate to high correlations. These correlations are mainly driven by jobs in the metal industry and by metal workers in construction industries. In our combined exposure analysis of ELF-MF adjusted for other occupational exposures in bivariate models, the patterns observed for ELF-MF remained the same, increasing our confidence in the results.
Strengths and limitations
Our study has several strengths compared with earlier studies. First, we used a prospective cohort to investigate the effects of occupational exposures on ALS mortality. The majority of studies on the association between occupational exposure to chemical agents and ALS have been performed in case-control settings,12 which may be vulnerable to recall bias. Second, we used JEMs to assess exposure levels instead of relying on self-reported exposure. Subjects may overestimate their own past exposures, leading to exposure misclassification and possibly bias if differential by case status.45 Third, we used a cohort with extensive information on potential confounders. This allowed us to address potential confounding both by demographic and lifestyle factors. Lastly, the NLCS includes information for up to five jobs up to baseline, instead of using a single occupation, which has been the case in many of the general population studies on ELF-MF and ALS to date.16 Given the age of the subjects at baseline and the average number of jobs reported at baseline (2.1 for men and 1.6 for women), we covered most of the job history for all subjects.
However, our study also had a number of limitations. First, we used causes of death to identify cases of ALS mortality, rather than using ALS incidence. Although the progression of ALS is generally fast, with patients dying on average 1–6 years after diagnosis,1 the cause of death could be misclassified on the death certificate.46 47 We also used the ICD-10 code for motor neuron disease (ICD-10 12.2) to identify ALS. Although ALS forms the large majority of motor neuron disease cases, these are not synonymous. In the NLCS, we observed a crude mortality rate of nine ALS mortality cases per 1 00 000 person-years, which is in line with estimates of the incidence rates in The Netherlands for this age group (~8 per 1 00 000 person-years for people 65–69 years of age).48 This provides evidence that our study has no significant under ascertainment of ALS cases through the mortality registration. Furthermore, it is unlikely that any under ascertainment or disease misclassification is differential by occupational exposure. As such, it would, if present, result in a loss of power without biasing the results.
Second, information on the occupational history of the subjects was only available up to baseline. However, as the population was between 55 and 70 years of age a large proportion of the cohort had already retired at baseline (79% of cases and 78% of the subcohort). Furthermore, on average, subjects in the cohort retired at 62 years of age, indicating that these subjects would only add a small number of exposed years to the cumulative exposure in the subcohort and cases. Therefore, this is unlikely to have a major influence on the results. Third, while the use of JEMs to assign occupational exposures is not prone to misclassification due to recall bias of self-reported exposure, it is possibly less reliable for some (specific) exposures when compared with expert assessment.45 Expert assessment was not possible as no detailed information on the job (eg, tasks performed) was available within the cohort. Furthermore, the JEMs used broad categories of occupational exposures (eg, metals, solvents and insecticides). This might have led to missing associations with specific occupational exposures, such as lead,15 formaldehydes38 or organochlorine insecticides.14 As the Shock-JEM is based on accident data, associations with shocks that did not lead to severe consequences might have been missed as well.
Finally, while the NLCS cohort is large, ALS is a rare disease, and the low numbers of high exposed subjects led to low power to detect potential effects of occupational exposures on ALS, in particular among women.
Conclusions
We studied the association between selected occupational exposures and ALS mortality. Only for ELF-MF in men we observed a significant increased risk of ALS mortality with increasing exposure levels. The other occupational exposures showed some weak non-significant associations with ALS mortality among men and women, without showing clear exposure-dependent trends in risk. This prospective study offers further support for an association between occupational exposure to ELF-MF and an increased risk of ALS mortality.
References
Supplementary materials
Press release
Press release
Files in this Data Supplement:
Footnotes
Funding This work was supported by The Netherlands Organization for Health Research (ZonMW) within the programme Electromagnetic Fields and Health Research under grant numbers 85200001 and 85800001.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.