Article Text

Abstract
Objective To determine whether lung function trajectories after 9/11/2001 (9/11) differed by sex or race/ethnicity in World Trade Center-exposed Fire Department of the City of New York emergency medical service (EMS) workers.
Method Serial cross-sectional study of pulmonary function tests (PFTs) taken between 9/11 and 9/10/2015. We used data from routine PFTs (forced expiratory volume in 1 s (FEV1) and FEV1% predicted), conducted at 12–18 month intervals. FEV1 and FEV1% predicted were assessed over time, stratified by sex, and race/ethnicity. We also assessed FEV1 and FEV1% predicted in current, former and never-smokers.
Results Among 1817 EMS workers, 334 (18.4%) were women, 979 (53.9%) self-identified as white and 939 (51.6%) were never-smokers. The median follow-up was 13.1 years (IQR 10.5–13.6), and the median number of PFTs per person was 11 (IQR 7–13). After large declines associated with 9/11, there was no discernible recovery in lung function. In analyses limited to never-smokers, the trajectory of decline in adjusted FEV1 and FEV1% predicted was relatively parallel for men and women in the 3 racial/ethnic groups. Similarly, small differences in FEV1 annual decline between groups were not clinically meaningful. Analyses including ever-smokers were essentially the same.
Conclusions 14 years after 9/11, most EMS workers continued to demonstrate a lack of lung function recovery. The trajectories of lung function decline, however, were parallel by sex and by race/ethnicity. These findings support the use of routine, serial measures of lung function over time in first responders and demonstrate no sex or racial sensitivity to exposure-related lung function decline.
Statistics from Altmetric.com
What this paper adds
Previous studies of the prevalence of post-9/11 symptoms and diagnoses in workers and others have shown differences by sex and by race and ethnicity.
None of these studies examined lung function decline over time by these demographic characteristics.
This study shows that there were no clinically significant differences in lung function trajectories by sex or race/ethnicity as a result of exposure to the World Trade Center (WTC) disaster.
Ongoing surveillance of affected populations remains important in understanding the long-term consequences of WTC exposure.
Introduction
Thousands of Fire Department of the City of New York (FDNY) firefighters and emergency medical service workers (EMS) responded to the World Trade Center (WTC) attacks on or after September 11, 2001 (9/11). During the months of rescue and recovery, many were exposed to high volumes of aerosolised dust, resulting in a well-described burden of WTC-related physical and mental health conditions.1–3 Starting before 9/11, the FDNY Bureau of Health Services (BHS) included lung function tests as part of its routine monitoring examination, recognising their importance in assessment of work fitness, efficacy of personal protective equipment and treatment response. Our earlier study of lung function in the FDNY cohort found that during the first post-9/11 year, lung function (forced expiratory volume in 1 s (FEV1)) decreased substantially in never-smokers, with greater declines in firefighters (−439 mL, or ∼15 times greater than usual) than EMS (−267 mL or ∼9 times greater than usual).4 The forced vital capacity (FVC) behaved similarly.4 A recently completed 13-year follow-up study that included only firefighters showed a lack of recovery in lung function.5
It remains unknown whether the observed lack of recovery in lung function following WTC exposure was influenced by sex and race/ethnicity. In the general population, lung volumes and their age-related declines are known to differ by sex and race/ethnicity.6 The incidence and clinical course of several respiratory diseases are also known to differ by sex and race/ethnicity.7–10 Further, non-WTC exposures, such as smoking and air pollution, have demonstrated a disproportional impact on women, who are at increased risk for reduced lung function, obstructive airways disease (OAD) and lung cancer.9–13 Sex hormones may play a role as they are associated with the regulation of lung innate immunity and inflammation.14 For these reasons, federally funded research mandates that sex and race/ethnicity effects be examined.15
FDNY firefighters are homogeneous—nearly all white men. FDNY EMS, however, are a diverse group, which allows examination of differences in the host response to WTC exposure by sex and race. Recently, we reported that in FDNY WTC-exposed EMS, the incidence of OAD was higher in women, but similar between whites and non-whites.16 We undertook the current study to compare the trajectories of post-9/11 lung function decline in this cohort, by sex and race/ethnicity, through the first 14 post-9/11 years.
Methods
Study population
Our base population included 2075 FDNY-EMS who were active FDNY employees on 9/11 or had left FDNY employment, but responded to the WTC attacks within the first 2 weeks (9/11–9/24/2001). Study participants gave written informed consent for research, had available body weight information (recorded on at ≥50% of monitoring examinations) and known smoking status. Owing to small numbers, Asians (n=43) and Native Americans (n=2) were excluded. The final population included 1817 (87.6% of base population) EMS. Montefiore Medical Center's institutional review board approved this study.
Spirometric measurements
FEV1 and FVC measurements were obtained from spirometries conducted during the FDNY-BHS's routine monitoring examinations, scheduled every 12–18 months, between 9/11 and 9/10/2015. The spirometers used during the current study were identical to those used in our previous work, as were exclusion criteria (improper scheduling, poor quality or physiologically impossible values) for invalid measurements, resulting in the exclusion of 1173 of 18 638 spirometries (6.3%).4 ,5 We used NHANES normative prediction equations to calculate FEV1% predicted based on sex, race/ethnicity and height for whites, African-Americans and Hispanics. FEV1, as an absolute value and as a per cent predicted (FEV1% predicted), was the outcome of interest due to the known greater variability of FVC.5
Other measures
Descriptive information (age, sex, race/ethnicity) was obtained from the FDNY employee database. Height and weight data were recorded at each monitoring examination. Weight was missing from 546 monitoring examinations with concurrent spirometry (3.1%); for these examinations, we imputed weight from the time of the closest examination with a non-missing weight.
Cigarette smoking status (never, former or current) was based on information from participants' most recent monitoring questionnaire. Only those reporting never smoking throughout the study period were classified as ‘never-smokers’.
Statistical analysis
Demographic comparisons were made using Pearson's χ2 test. We assessed FEV1 and FEV1% predicted over time in never-smokers (n=939) stratified by sex and race/ethnicity, and in current, former and never-smokers stratified by sex. We conducted similar analyses using FVC as the outcome (absolute and % predicted). The FEV1 and FEV1% predicted findings have different interpretations: The longitudinal FEV1 analyses are comparisons of decline rates within-individuals, across the different groups. The longitudinal FEV1% predicted analyses assess differences over time in how the NHANES reference population compares with our population in FEV1. Owing to the nature of our data (repeated measures with significant variability between participants), we used mixed linear models with a random intercept and adjusted for age on 9/11 and weight at the time of the spirometry. Models with absolute FEV1 as the outcome were adjusted for height. Age was assessed as a linear and non-linear effect; however, because there was no discernable difference, age was included as a linear effect. All models estimated the weighted average values of each outcome in 1-year increments from 9/11 to 9/10/2015. Analyses were performed using SAS (V.9.4; SAS Institute, Cary, North Carolina, USA).
Results
Study population
Three hundred and eighty-eight of the 1817 (21.4%) were African-American and 450 (24.8%) were Hispanic; 334 (18.4%) were women. While the most common race was white (n=979, 53.9%), women were more likely than men to be African-American (27.5% vs 20.0%, p=0.002). Overall, 51.7% were never-smokers and 12.5% were current-smokers. Smoking status differed slightly by sex, as women were less likely than men to report never smoking (46.4% vs 52.9%; p=0.033) and by race, as African-Americans were more likely to be never-smokers (61.9% vs 46.6% for whites and 54.0% for Hispanics; p<0.001). The median number of spirometries per participant was 11 (IQR 7–13) with a median length of follow-up 13.1 years (IQR 10.5–13.6); both were similar by sex. Excluded EMS had similar characteristics to those included in the final population (data not shown).
After 9/11, there was no discernible recovery in lung function. FEV1 annual decline was greatest among current-smokers and lowest among never-smokers, with a difference of 12.5 mL/year for men and 10.8 mL/year for women between the two smoking statuses.
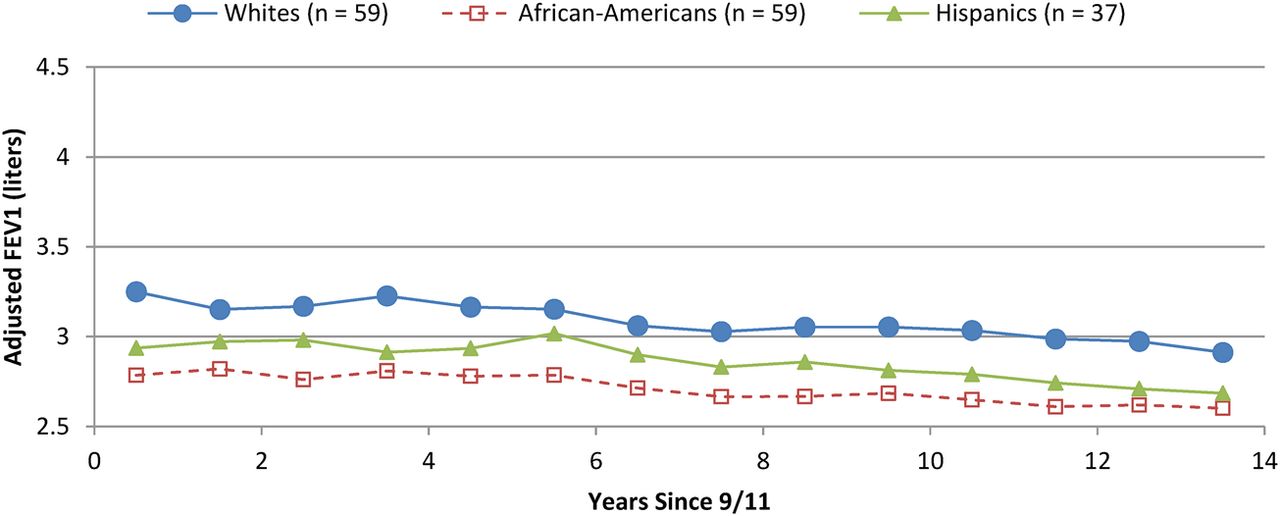
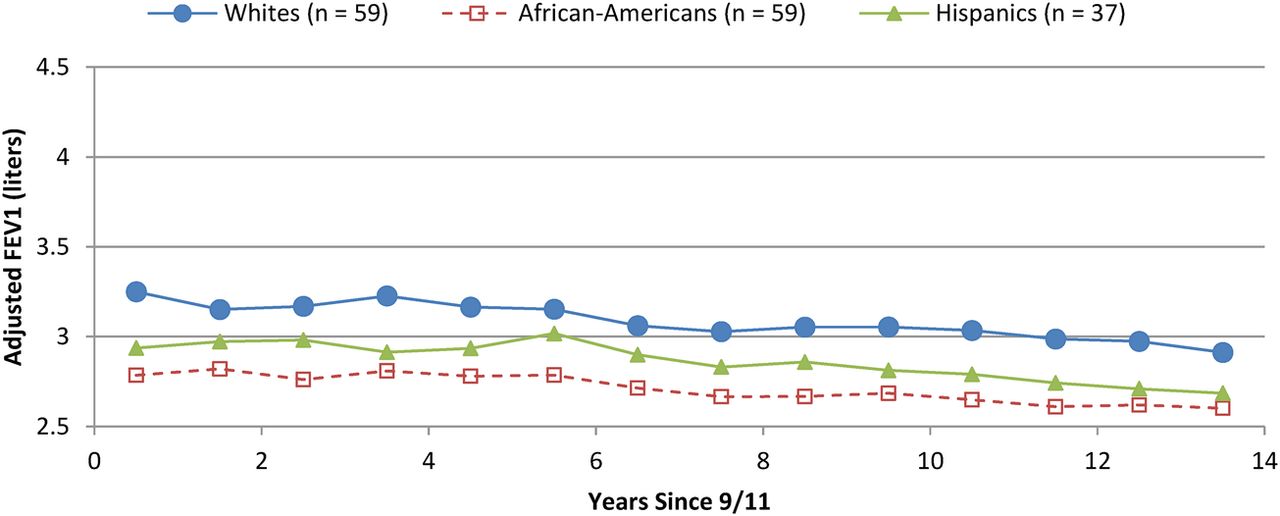
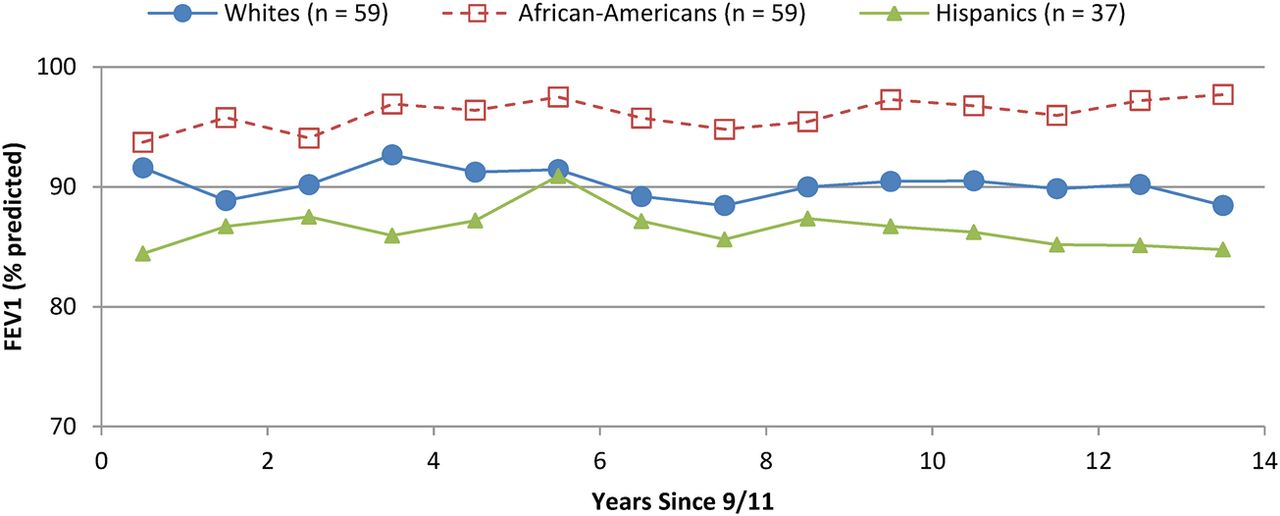
Among the 939 never-smokers, the trajectories of post-9/11 decline in adjusted FEV1 and FEV1% predicted were relatively parallel for men (figure 1, panels 1 and 2) and women (figure 1, panels 3 and 4) in the three race/ethnic groups throughout follow-up. African-Americans had the lowest adjusted FEV1, but the highest FEV1% predicted. The small differences among race/ethnic groups in FEV1 annual decline were not clinically meaningful. The largest difference in yearly decline was between white and Hispanic men (4.1 mL/year) and African-American and Hispanic women (4.9 mL/year). Neither sex nor race/ethnicity was associated with recovery. Analyses including former and current-smokers were similar, as were results using FVC and FVC% predicted (data not shown).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trajectories of post-9/11 decline in adjusted forced expiratory volume in 1 s (FEV1) and FEV1 per cent predicted in never-smoking male and female emergency medical service workers in the three race/ethnic groups.
Discussion
We carried out this study among 1817 WTC-exposed EMS, and believe that we are the first to report that the trajectory of post-9/11 lung function decline (FEV1 and FEV1% predicted) was similar for WTC-exposed men and women and also did not differ by race/ethnicity. As we found in firefighters,5 current-smokers had a greater annual decline than never-smokers. Our findings rely on the availability of high-quality, serial lung function measurements, which have proven to be an extraordinary resource for understanding the impact of WTC exposures on worker health. An important distinction between this WTC-exposed EMS cohort and general population studies is that in this cohort, neither sex, race/ethnicity, nor smoking status is associated with income, as all EMS were FDNY employees with similar pay based on collective bargaining agreements.
Our study has some limitations. We do not have normative equations that are more specific than ‘African-American’; thus, our finding that African-Americans have the lowest adjusted FEV1 but the highest FEV1% predicted may be the result of ethnic and/or demographic differences between our population and the NHANES reference population. Also, we used the ‘Mexican-American’ prediction equations from NHANES as normative values for Hispanics, although the proportion of our Hispanic population that identifies as Mexican-American is unknown. As a result, intra-racial/ethnic differences in FEV1 may be greater than inter-racial/ethnic differences. We also acknowledge that the use of these equations to adjust for the impact of ‘normal’ ageing on FEV1 is imperfect. Nonetheless, normative equations are widely used and we observed similar trajectories when our outcome was actual FEV1 rather than FEV1% predicted. Finally, since we modelled annual decline by sex and race/ethnicity, some of the data for women were based on relatively small sample sizes, which also prevented our examination of decline by smoking status and by race/ethnicity in women.
The study strengths outweigh its limitations. Strengths include a relatively large proportion of women and non-whites, all of whom met pre-employment physical requirements; a cohort defined prior to 9/11 with analyses limited to lung function data obtained from routine monitoring examinations, thereby reducing potential selection bias; and, minimal longitudinal dropout over a lengthy post-exposure follow-up, using the same spirometers and techniques as we have previously reported.
In conclusion, over 14 years of follow-up, we found a continued lack of lung function recovery and trajectories of lung function decline that did not vary by sex or race/ethnicity. The public health implications of this study include support for routine serial measures of lung function over time in occupational cohorts with significant exposure risks.
Acknowledgments
This project was supported by the World Trade Center Health Program contracts from the National Institute of Occupational Safety and Health and R01HL119326. DJP had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
References
Footnotes
Contributors TKA, MV, RZ-O, CBH and DJP designed the study, analysed and interpreted the data. TKA and DJP had the initial idea for the study. TKA, MV, RZ-O, CBH and DJP had full access to the data. TKA, MV, RZ-O and DJP drafted the first manuscript with critical revisions from CBH, TS, WM, MPW, HWC, AN, MDW, VC and KJK. All authors have approved the final manuscript.
Funding National Institutes of Health, 10.13039/100000002, R01HL119326, National Institute of Occupational Safety and Health, 200-2011-39378, 200-2011-39383.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Montefiore Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.