Article Text

Abstract
Objectives To investigate exposure–response relationships between measured movements and postures of the wrist and the incidence of carpal tunnel syndrome (CTS), and any modifications by sex.
Methods In 2011, we established a historical cohort of 9364 members of the Painters’ Union in Denmark. Self-reported task distributions were obtained by questionnaire (53% responded) and combined with sex-specific task exposure matrices to get individual estimates of exposure intensity, that is, velocity of wrist flexion/extension, mean power frequency (MPF) and non-neutral wrist postures. Exposure duration was assessed from yearly working proportions. Registered first-time hospital discharge CTS diagnoses and CTS surgery were collected as outcomes. The cohort was followed from 1994 to 2010. Log-linear Poisson regression was used.
Results For CTS diagnoses, the adjusted incidence rate ratios (IRRs) increased with increasing wrist velocity (IRR=1.37 (95% CI 1.10 to 1.71) per °/s) and MPF (IRR=1.53 (95% CI 1.21 to 1.91) per 0.01 Hz). For CTS surgery, the results were similar. The outcomes were not related to non-neutral postures or exposure duration. The adjusted IRRs for women were higher than those for men. There were no multiplicative interaction effects between exposure intensity, exposure duration and sex. However, the absolute incidence rates (IRs) increased at a steeper rate for women than for men, indicating an additive interaction.
Conclusions The incidence of CTS increased with increasing velocity of wrist flexion/extension and MPF of wrist movements. The relative increase in incidence rates was the same for women and men, but the absolute incidence rates increased at a steeper rate for women than for men.
Statistics from Altmetric.com
What this paper adds
It is well documented that women report more work-related musculoskeletal disorders in the upper extremity than men, but it is unknown if women are more vulnerable than men are at the same level of exposure.
This study combines outcome data from the Danish National Registers with questionnaire data and sex-specific task exposure matrices, to investigate exposure–response relationships between postures and movements of the wrist and the incidence rate of carpal tunnel syndrome (CTS) diagnoses and CTS surgery, and any modifications by sex, in a seemingly homogeneous population.
Our findings suggest that repetitive and high velocity wrist movements are occupational risk factors for CTS, whereas this relationship was not found for non-neutral wrist postures. There was no indication of cumulative effects.
We found the same relative increase in CTS for men and women by the same change in exposure, and by this criterion, women are not more vulnerable than men are; yet the same change in exposure caused a larger absolute increase in CTS for women than for men, and in this sense women are more vulnerable than men are.
Introduction
Carpal tunnel syndrome (CTS) is one of the most common wrist disorders associated with occupational exposures.1 ,2 The exact pathogenesis of CTS is unknown but increased pressure on the median nerve by the surrounding tissue in the carpal tunnel plays a role.3 Several risk factors for CTS are well known including age, sex, body mass index (BMI), pregnancy and medical conditions such as rheumatoid arthritis, diabetes, hypothyroidism and trauma.1 Forceful and repetitive movements and awkward postures of the wrists as well as exposure to hand-arm vibrations have been reported as occupational risk factors for CTS but few studies have included objectively measured exposures.1 ,4–8 Furthermore, it is not clear if any exposure effect is related to the short-term intensity or to a long-term cumulated effect and if any effects are different for men and women. Treatment options include rest, splinting, local corticosteroid injections and surgery.9 ,10
Many studies have investigated sex differences in the occurrence of work-related musculoskeletal disorders (WMSDs) in the upper extremity.11–13 When investigating exposure–response relationships, most studies have assumed that men and women within the same profession have equal exposures. This assumption has been criticised because there could be large differences in exposures due to different sex-specific task exposures and sex-segregated task distributions, even within the same profession.14–16 If so, results on sex differences in the occurrence of WMSDs could be biased by inaccurate exposure assessment. In a previous study of Danish house painters,17 we found only minor sex differences in task distributions and task-specific movements and postures of the wrists. This led us to conclude that house painters in Denmark is a profession suitable for examining if women are more biologically vulnerable than men are at the assumed same level of exposure.
The aim of this study was therefore to investigate (1) exposure–response relationships between objective measures of movement intensity and postures of the wrist and the incidence of CTS; (2) the relationship between exposure duration and the incidence of CTS and (3) if the effects of exposure intensity were modified by exposure duration and sex.
Methods
Population
The study cohort comprised all members of the Painters' Union in Denmark, who were born in 1940 or later and were still members and living in Denmark on 1 March 2011 (N=9364, 6236 (66.6%) men and 3128 (33.4%) women). The study population for analysis consisted of those members of the cohort who filled in a questionnaire sent by postal mail with up to two reminders (N=4957, 52.9% of the study cohort).
Outcomes
Since 1968, every person in Denmark with permanent residency is assigned a personal identification number (PIN) from the Danish Civil Registration System.18 The PIN enables linkage of information at the individual level in all Danish national registers. The Danish National Patient Register (DNPR) contains personal information on practically all patient contacts with the Danish public hospital system, and since 2003 also for private hospitals.19 Since 1994, diagnoses have been reported using the International Classification of Diseases, 10 (ICD-10), and since 1996 surgery has been reported using the Danish version of the NOMESCO Classification of Surgical Procedures (NCSP-D). From the DNPR, we extracted information on CTS diagnoses (ICD-10 code G56.0) and CTS surgery (NCSP-D codes KACC51 and KACC61) and the date of diagnosis and surgery. DNPR surgery cases were a subset of DNPR CTS diagnoses.
Some patients are diagnosed and/or treated by private practising surgeons. In Denmark, this group of healthcare professionals are contracted by the Danish National Health Service and they receive payment by reporting a service code, indicating the form of service they have provided, to the Danish National Health Service Register (NHSR).20 The service code 3146 (‘nerve compression’) has been used since 2002. The code is non-specific with respect to the type of nerve compression, and does not distinguish between diagnosing the nerve compression or performing decompression surgery. On the basis of information from specialists in the area, we assume that the service code 3146 is primarily used for CTS cases. These cases were included as CTS diagnoses in a sensitivity analysis.
Exposure intensity
The individual exposure assessment was based on a self-record of task distribution and sex-specific task exposure matrices (TEMs) based on technical measurements of task-specific movements and postures of the wrist. Details have been described in a separate paper.17 Task distributions were constructed by having the questionnaire respondents divide their working hours in a typical week between the 12 most common painting tasks (eg, painting with a brush, painting with a roll, spraying, levelling, sanding, covering, driving, other tasks). The typical week should represent their work as a painter since 1990. Sex-specific TEMs of movements and postures of the upper extremity were constructed using goniometry (wrists) and inclinometry (shoulders, neck and forehead) to measure 50 full working days equally distributed between male and female house painters. During the measurements, a log-book clearly stating the time spent on each task was filled out by the participants.17 Exposure measures from the TEMs were weighted by the self-reported task distributions to obtain individual estimates of exposure intensity for the wrist in terms of median velocity of flexion/extension of the wrist (wrist velocity) (°/s), mean power frequency (MPF) (Hz) of wrist movements as a measure of repetition, and non-neutral wrist postures as a combined measure of extreme postures of flexion/extension and radial/ulnar deviation of the wrist, defined as the %time with angles exceeding 45° flexion/extension or 20° ulnar/radial deviation.17
Exposure duration
Information on start date and seniority as a painter was obtained from the questionnaire. For each calendar year, the yearly working proportion was assessed from record linkage with Danish national registers. Information on periods of absence from work during employment (ie, maternity leave, sickness absence and periods of education) was obtained from the Danish Register for Evaluation of Marginalisation, which contains data on all Danish public transfer payments on a weekly basis.21 Data on periods of unemployment was obtained from the Integrated Database for Labour Market Affiliation for Persons, which contains data on yearly unemployment as a proportion of the total number of possible working days per year. On the basis of this information, we calculated a yearly working proportion for each member of the cohort (range 0–1, 0=did not work that year, 1=worked all working days that year). The working proportion was calculated for each calendar year after entry into the study (see below in the statistical analyses section).
Other covariates
Information on sex and date of birth was obtained from the Civil Registration System.18 From the questionnaire, we obtained information on height and weight, fractures near the wrist, and comorbidity in terms of thyroid disorders, diabetes, rheumatoid arthritis, gout and connective tissue disorders (0=none, 1=any of these diseases). BMI was calculated as weight (kg)/height (m)2. A pregnancy variable was defined as a period of 7 months prior to and 5 months after giving birth according to dates of birth obtained from the DNPR.
Statistical analyses
The incidence rate ratios (IRRs) of all CTS diagnoses and of the subset with CTS surgery were examined by survival analyses with exposure intensity and exposure duration variables, sex, age, BMI, fractures near the wrist, comorbidity and pregnancy as explanatory factors. Age, seniority, working proportion and pregnancy were considered as time-dependent variables. Pregnancy had no significant effect in any of the models examined and was therefore not included in the final models.
The cohort members were followed from 1 January 1994 or start date as a painter, whichever came last, until a first-time CTS event or 1 January 2011, whichever came first (the cohort only consisted of persons who were alive at the end of follow-up). Ninety-one persons emigrated during the study period, with a combined risk time of 112.3 person-years (0.1% of the total risk time). Since the majority of these were only temporary migrations, no exclusions were made. Risk time was calculated from entry to exit date for each calendar year, broken down by time-dependent variables. Risk time calculations were made with a publicly accessible macro22 using the methodology of a Lexis diagram.23 Persons with a CTS event before start of follow-up or start as a painter were excluded. A CTS event was defined as a CTS diagnosis in the analyses of CTS diagnoses (including surgery cases) and as CTS surgery in the analyses of CTS surgery. The reason for not excluding prior CTS diagnoses without surgery in the analyses of CTS surgery was that CTS diagnoses without surgery may reflect less severe cases with a more uncertain diagnosis. We used a log-linear Poisson model for the analyses with logarithmic transformation of the risk time as offset value.
The effects of exposure duration were examined in separate parallel analyses of the effects of the working proportion variable calculated over years for time windows of 1, 2 and 5 years and for seniority in each calendar year before the year of occurrence of a CTS event. These variables were included in the models as continuous covariates and the effects were assessed by the effect of a full working year (working proportion=1).
In the analyses of data for both sexes, we examined if the effects of the exposure variables were different for men and women by including a multiplicative interaction term between sex and the exposure variable. We made graphical analyses of sex-specific observed IRs of CTS by tertiles of exposure intensity compared with corresponding continuous IR estimates from the analytical models. We also examined if there was a multiplicative interaction between exposure intensity and duration. Non-significant interaction terms were excluded from the final models.
Since we considered CTS diagnoses with surgery as more reliable than CTS diagnoses without surgery, all models were examined twice, once for all CTS diagnoses and once for the subset with CTS surgery. In a sensitivity analysis, we included service code 3146 (‘nerve entrapment’) from the NHSR as a CTS diagnosis to assess the stability of the results. Finally, we examined if the effects of factors recorded for the whole cohort (age, sex, seniority and working proportion) on CTS diagnoses and CTS surgery were different for questionnaire responders and non-responders.
Statistical analyses were made using SAS statistical software (V.9.3 Cary, North Carolina, USA). The GENMOD procedure was used to fit the log-linear Poisson models. No imputation was made for missing data.
Ethics statement
The study protocol was accepted by the Regional Scientific Ethics Committee, Capital Region of Denmark (j.no.: H-C-FSP-2010-036). Individuals who participated in the technical exposure measurements gave written informed consent. The Danish Data Protection Agency gave permission to store personal information concerning the participants (j.no.: 2010-41-5325).
Results
In the DNPR, we identified 464 registrations of CTS, of which 192 qualified as first-time diagnoses. After exclusion of persons with a CTS diagnosis before entry into the Painters' Union, 155 first-time CTS diagnoses remained. They included 108 cases who responded to the questionnaire, including a subgroup of 71 cases with first-time surgery for CTS. In the NHSR, we identified 54 additional cases of first-time nerve entrapments among questionnaire responders and with service code dates after start date as a painter.
Table 1 presents characteristics of the total cohort and of questionnaire responders. The incidence rate of CTS diagnoses and CTS surgery was approximately 15% higher among questionnaire responders than in the total material. The proportion that responded was lower among men (51%) than among women (59%), especially among younger men. Among questionnaire responders, the men were on average 14 years older than the women were and had worked 13 years more as a painter. These differences are due to a secular trend of recruiting increasingly more women to the profession. There were few missing questionnaire values (BMI, n=183 (3.7%); fractures near the wrist, n=134 (2.7%); and comorbidity, n=170 (3.4%)). The prevalence of comorbidity was twice as high among men as among women, most likely due to the higher age among men. The reported prevalences (men/women) were: thyroid disorders: 2.4/3.6%; diabetes: 6.3/1.0%; rheumatoid arthritis: 10.1/5.4%; gout: 4.4/0.7%; connective tissue disorders: 1.2/0.9%. The high prevalences of rheumatoid arthritis are probably due to a misconception about the disorder being mixed up with, for example, arthrosis.
Characteristics of the total material and of the study population of questionnaire responders
Information on task distribution was missing for 537 participants (11%), leaving 4420 participants for the analyses. Table 2 shows the distributions of the three exposure intensity variables and their Pearson correlations. For median velocity, there was no statistically significant difference between men and women. For MPF, women had significantly lower values than men. The time spent in non-neutral wrist postures was statistically significantly higher for women, but the overlap in distributions was large.
Distributions of exposure intensity variables and their correlations
For women, there was a strong correlation between MPF and wrist velocity (0.80) and a moderate correlation between MPF and non-neutral postures (−0.60). Other sex-specific correlations reached a maximum of 0.21.
Table 3 shows the crude and adjusted effects of exposure intensity variables, work proportion and sex. Owing to missing values, the analyses were based on 4198 participants (85% of the questionnaire responders).
Crude and adjusted IRRs of CTS diagnoses and surgery by wrist exposure intensity and duration variables and by sex
Crude IRRs were similar to the IRRs in the adjusted models for median velocity, non-neutral wrist postures and working proportion. For MPF, the crude effect was in the opposite direction of the adjusted effect. This was due to the lower MPF in women (table 2) and their risk of CTS. Since women had a higher risk of CTS, this resulted in a decreasing crude IRR of CTS with increasing MPF, even though the IRR increased with increasing MPF for both men and women. Also, the crude IRRs for women versus men increased after adjustment, mainly due to the different age distribution of men and women.
Increasing wrist velocity was associated with statistically significantly higher IRRs for CTS diagnoses and CTS surgery, total and for women (table 3), with IRRs between approximately 1.4 and 1.6 per °/s. For men, the IRRs were lower, 1.1–1.2 per °/s, and not statistically significant. Apart from the crude total effect, increasing MPF was also associated with statistically significantly higher IRRs for CTS diagnoses and CTS surgery, total and for women, with IRRs between approximately 1.5 and 1.6 per 0.01 Hz. For men, the IRRs were of the same order of magnitude for CTS diagnoses and slightly higher for surgery, but far from statistical significance. Increasing %time with non-neutral wrist postures showed no significant associations with CTS outcomes, except that the adjusted association for CTS diagnoses for women was just significantly below unity, opposite to the hypothesised direction.
Exposure duration (working proportion) in the previous year was not significantly related to the CTS outcomes in any of the models (table 3) and neither were exposure periods of 2 and 5 years prior to events (data not shown).
In the adjusted analyses, the IRs for women were approximately four times higher for CTS diagnoses and six times higher for CTS surgery than for men in the model for wrist velocity. The same pattern was found in the models for MPF and non-neutral wrist postures (data not shown).
Increasing age and BMI, previous fractures and comorbidity were associated with higher IRRs of CTS outcomes (data not shown).
Age and seniority were highly correlated (Pearson correlation coefficients 0.82 among men and 0.77 among women), and their effects could therefore not be separated. Age had a stronger and more consistent effect than seniority, and seniority was therefore not included as a covariate in the final models.
Interactions
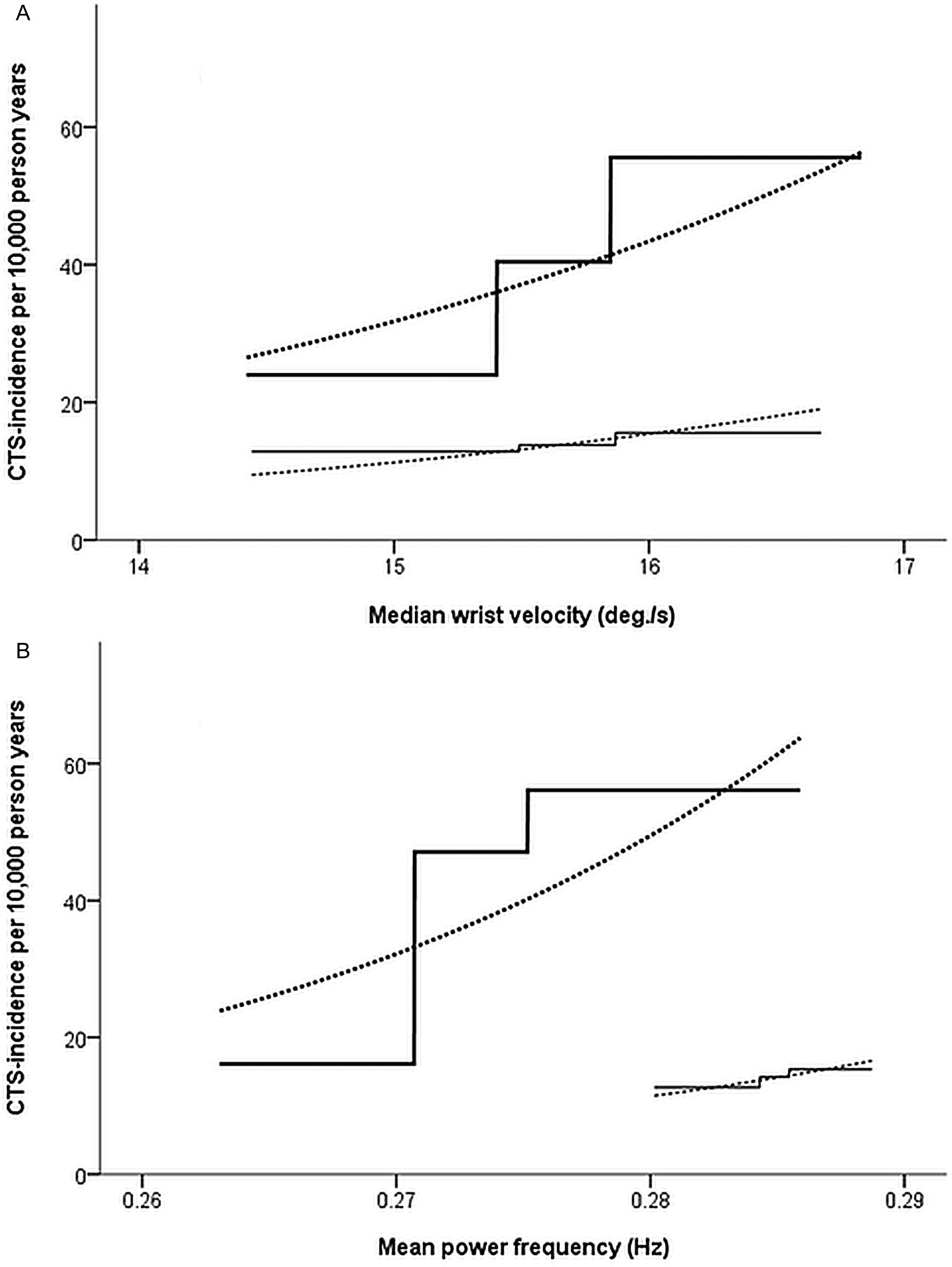
There were no significant multiplicative interactions between sex and any of the exposure intensity or duration variables in any model, indicating that the effects of exposure were the same for men and women. However, this was the case in a logistic regression analysis. When the estimates are back-transformed, the lack of a multiplicative interaction in the logistic analyses means that the ratio of the IRs for men and women is constant across the exposure variable. Since women had a higher IR of CTS outcomes, the absolute difference between men and women increased. These relations are illustrated in figure 1 for median velocity and for MPF. For raw data, we calculated and plotted the IRs by sex-specific tertiles of the exposure variable, overlaid by the estimated absolute IRs based on the back-transformed effect estimates from the logistic regression analyses, adjusted for sex. The figure demonstrates the different absolute increase in IR by sex-specific tertiles and continuously as estimated from the analyses. The figure for MPF also illustrates the different distribution of this exposure for men and women and why the crude association with CTS was negative for this variable (table 3).

{kind=link}
Observed incidence rates of carpal tunnel syndrome (CTS) diagnoses by tertiles (solid lines), with estimated rates, based on crude associations adjusted for sex (model Total in table 3) (dotted lines), overlaid. All lines (thin for men and thick for women) are displayed in the 5th–95th centile interval of: (A) median wrist velocity and (B) mean power frequency.
There were no significant multiplicative interactions between the exposure intensity variables and the duration variables.
Sensitivity analyses including incident nerve entrapment cases from the NHSR showed the same significant effects, albeit with slightly lower effect estimates (data not shown).
Discussion
We found that the IRs of CTS diagnoses and CTS surgery increased with increasing velocity of wrist flexion/extension and MPF, but not with non-neutral wrist postures. The duration of work measured as the working proportion during 1, 2 and 5 years prior to a CTS event had no significant effect. These findings suggest that high velocity and repetitive wrist movements are occupational risk factors for CTS, whereas this association was not found for non-neutral wrist postures.
The effects of velocity and repetition on CTS were the same for men and women in the logistic regression analyses (no multiplicative interaction). However, when back-transformed to absolute IRs, the IRs for women increased at a steeper rate than for men because women had a higher basic IR of CTS than men. This response pattern reflects an additive interaction of sex with wrist velocity and MPF.
The effects of velocity and repetition were not modified by exposure duration 1, 2 and 5 years prior to a CTS event, indicating that the effects of median velocity and MPF may develop after a short exposure period with no prior accumulation of effects over time.
Strengths and limitations related to exposure assessment
A main strength was that the exposure was expressed on continuous generic scales, based on technical measurements recorded in a preceding study.17
One limitation was the low proportion of questionnaire responders, and that quite a few had missing values, leaving only 45% of the total cohort for the survival analyses. Questionnaire responders had a higher IR of CTS outcomes than non-responders. This difference could cause inflation bias, if questionnaire response status was also related to higher exposure.
Individual exposure intensity measures were based on questionnaire information on distribution of painting tasks during a typical working week for painting work after 1990. Obviously, this is a difficult question, especially if there was a large individual variation in task distributions over years. According to representatives of the Painters' Union in Denmark, work as a painter had not changed much over the years, although some changes had taken place, for example, more giraffe drywall sanding. If status as a CTS case influenced the recall of the typical task distribution, this may have resulted in inflated effect estimates. If so, we think that CTS cases would probably report a higher proportion of tasks with high force requirements. Analyses comparing the sex-specific task distributions for all questionnaire responders with the subgroup of CTS cases revealed that male cases primarily did more ‘spraying’ and ‘other tasks’ and less ‘hanging wallpaper’ and had fewer pauses.17 Female cases reported more ‘full levelling’ and ‘hanging wallpaper’ and less ‘driving’. Some of the tasks that are usually considered among the hardest (‘giraffe drywall sanding’ and ‘removing wallpaper’) were reported for a lower proportion of the time among both male and female cases. This indicated that cases did not just report more of the tasks which were felt as physically demanding. Also, if recall bias was to explain our results, we would expect that non-neutral wrist postures had been related to the outcomes as well. Knowing that the composition of a questionnaire can influence the responses,24 ,25 we tried not to use phrases which implied a special interest in CTS, and the questionnaire contained questions on many different personal and physical aspects.
Another limitation was that no measure of muscular load was included. In a previous study,26 we have shown that male and female house painters exert the same absolute force doing the same tasks. Owing to their lower physical strength, women are therefore exposed to a higher relative muscular load than men are.27 It has been suggested that a sex difference in relative muscular load accumulated over years may play a role in the development of WMSDs.28
The distribution of MPF turned out to be quite different for men and women when weighted with self-reported task proportions. This was due to a pattern of slightly lower MPF estimates for women than for men in tasks with a higher proportion among women than among men. The resulting difference in MPF distribution for men and women may to some extent be an artefact resulting from imprecise estimates of task proportions. However, since we analysed the data controlling for sex, and separately for men and women, the different distributions of MPF for men and women were not likely to affect our results.
Strengths and limitations related to outcomes
It is a main strength of the study that the outcome is based on medical diagnostic criteria and recorded independent of the exposure.
The DNPR functions as a tool for payment of health services related to specific diagnoses and surgery. It is therefore considered as almost complete and of good quality.19 Since 2003, it has been mandatory for private hospitals to report all services, but a 2008 estimate from the Danish National Board of Health still showed an under-reporting of 5% in surgery reported to the DNPR.19 We consider this misclassification as non-differential in relation to our study. Our IRs resembled those of a Swedish register-based population study reporting IRs of CTS diagnoses of 18.2 per 10 000 person-years for men and 42.8 for women, including non-hospital cases.29
In a sensitivity analysis, we supplemented DNPR CTS cases with incident cases of service code 3146 (‘nerve compression’) from the NHSR system for health services outside hospitals, also a tool for determining payment for specific services.20 From personal contact with practitioners in this field, we were assured that most of these registrations concern CTS. The results of these analyses were very similar to the results for CTS diagnoses based only on hospital cases. Slightly lower IRRs in these analyses may indicate more diagnostic misclassification in the NHSR cases.
Interpretation
Our results are in accordance with other studies showing that CTS may be caused by high velocity and repetitiveness of wrist movements. Thus, a 2012 meta-analysis concluded that repetitive wrist movements may cause CTS.1
Regarding repetitive wrist movements expressed on generic scales, our results are directly comparable regarding exposure with a cross-sectional study where the exposures were assessed with the same method. However, in this study, the prevalence of CTS was assessed by a standardised clinical examination of all participants, while in our study the incidence was based on cases with symptoms sufficiently severe to surpass the iatrogenic threshold by being subjected to hospital examination and treatment. Still, comparisons of incidence and prevalence rates, on generic continuous scales, may enhance the understanding of how to aggregate results from studies with different designs.
We did not find any association between non-neutral wrist postures and CTS. This is in contrast to a recent meta-analysis5 which showed a relative risk of 2.01 (CI 1.32 to 2.97) with high exposures to non-neutral wrist postures. However, this meta-analysis only included studies where non-neutral wrist postures were assessed by self-report or by an observer. Our results supported a meta-analysis from 20121 and a systematic review from 2009,30 which, in concurrence with others,31–33 found insufficient evidence for non-neutral wrist postures increasing the risk of CTS.
We do not know the exact mechanisms behind the development of CTS. The pathogenic effects of the exposures may arise after a short time, possibly in combination with other intrinsic or extrinsic host factors, or may be accumulated over a longer time frame before it becomes manifest as clinical CTS. In the latter case, one would expect that the effects of exposure intensities were modified by duration of exposure. Since we found no statistically significant interactions between exposure intensity and duration variables, our results do not support the idea that CTS is a ‘cumulative trauma disorder’.
If our results are solid and can be extrapolated to other occupations and tasks, the additive interaction of sex with wrist velocity and repetition indicates that preventive measures directed at reducing these exposures would be more effective in reducing the number of work-related CTS cases if directed towards women rather than towards men.
Generalisability
In our study, the range of exposure intensity variables was not very wide compared with other studies that have included a diversity of occupations.28 Our study was limited to Danish house painters, and the results should therefore be interpreted with caution when applied to other populations. Considering the paucity of other studies on the interplay between recent and cumulated wrist exposures and between sex and ergonomic wrist exposures with respect to CTS, our results also need to be confirmed in other studies.
Conclusion
Our study showed an increasing risk of CTS with increasing velocity and MPF of wrist movements. We found the same relative increase in CTS for men and women by the same change in exposure, and by this criterion women cannot be seen as more vulnerable than men. Yet the same change in exposure caused a larger absolute increase in CTS for women than for men, and in this sense women are more vulnerable than men.
References
Footnotes
Contributors TH-H contributed to the conception and design of study; data acquisition; data analyses; interpretation of data; and drafting of the work. SM contributed to the conception and design of study; data analyses; interpretation of data; drafting of the work; and revising it critically. SWS and JFT contributed to the conception and design of study; interpretation of data; and revising it critically. LCT contributed to the data analyses; interpretation of data; and revising it critically. G-ÅkH contributed to the conception and design of study; data acquisition; interpretation of data; and revising it critically. All the authors gave final approval of the version to be published.
Funding The study was funded by the Danish Working Environment Research Fund (grant number 43-2010-03).
Disclaimer The funding source had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study protocol was accepted by the Regional Scientific Ethics Committee, Capital Region of Denmark (j.no.: H-C-FSP-2010-036). The Danish Data Protection Agency gave permission to store personal information concerning the participants (j.no.: 2010-41-5325).
Provenance and peer review Not commissioned; externally peer reviewed.