Article Text

Abstract
Objectives Major depressive disorder (MDD) is associated with absenteeism. In this study, the effectiveness of collaborative care, with a focus on return to work (RTW), was evaluated in its effect on depressive symptoms and the duration until RTW in sick-listed workers with MDD in the occupational health setting.
Methods In this randomised controlled trial, 126 sick-listed workers with MDD were randomised to usual care (N=61) or collaborative care (N=65). Collaborative care was applied by the occupational physician care manager, supported by a web-based tracking system and a consultant psychiatrist. Primary outcome measure was time to response. Secondary outcome measures were time to remission, depressive symptoms as continuous measure and the duration until full RTW.
Results Collaborative care participants had a shorter time to response, with a difference of 2.8 months. However, no difference was found on time to remission or depressive symptoms as continuous measure. With a mean of 190 days in the collaborative care group, and 210 days in the usual care group, the groups did not differ significantly from each other in the duration until full RTW. Adherence to the collaborative care intervention was low.
Conclusions These results do not justify a widespread implementation of collaborative care in occupational healthcare, as it was operationalised in this study. However, since the study might have been underpowered for RTW and because treatment integrity was low, further research, with larger sample sizes, is needed to develop the best fitting (collaborative care) model for addressing RTW in depressed sick-listed workers.
Trial registration: ISRCTN78462860
Statistics from Altmetric.com
What this paper adds
-
Major depressive disorder (MDD) is associated with absenteeism. To achieve a more rapid return to work (RTW) as well as a reduction in depressive symptoms in sick-listed patients with MDD, a focus on both aspects is essential in treatment.
-
Compared with usual care, collaborative care applied by occupational physician-care managers led to a faster response (ie, at least 50% reduction in depressive symptoms). However, no difference between the two groups was found on the duration until RTW, time to remission or depressive symptoms as continuous outcome measure. Adherence to the collaborative care intervention was low.
-
A widespread implementation of collaborative care in the occupational healthcare setting, as it was operationalised in this study, is not yet justified.
Introduction
Major depressive disorder (MDD) is strongly associated with negative work outcomes such as absenteeism.1 ,2 In the Netherlands, workers with MDD have 8–9 times more absence days than their colleagues without MDD, and with a mean duration of 200 days, absences due to depressive symptoms often have a long duration.3–5 Moreover, MDD is the largest contributor to the total number of sickness absence days in the Dutch working population, generating an annual cost of 1.8 billion Euros.6 Besides placing a high financial burden on society, prolonged absence from work has important consequences for the quality of life of the depressed, sick-listed worker.7 Therefore, reducing sickness absence and stimulating return to work (RTW) is important.
Sickness absence and RTW are multifactorial phenomena, influenced by the health condition and personal characteristics of the worker as well as by environmental factors such as the workplace and the healthcare system.8–10 In line with this multidimensionality, research showed that a reduction in depressive symptoms does not automatically lead to RTW.11–13 Thus, focusing treatment solely at symptom reduction is not sufficient. To achieve a more rapid RTW as well as a reduction in depressive symptoms in sick-listed patients with MDD, a focus on both aspects is essential in treatment.11–13 Moreover, current evidence suggests that interventions aimed at RTW need to take into account the work environment and could be best delivered by professionals who are close to, and familiar with, the work environment, such as labour experts or occupational physicians (OPs).13 ,14 In the Netherlands, OPs play a central role in the guidance of sick-listed workers. Since more than a century, treatment and sickness certification are separated from each other in Dutch social security legislation. The OP was introduced to provide better guidance to RTW, as regular physicians found it hard to do so. The separation between OP and other physicians was aimed at protecting the worker's privacy and at the possibility for the sick-listed worker to maintain a confidential relationship with the curative physician.15 However, this separation resulted in a lack of collaboration and communication between OPs and the curative sector and a lack of focus on RTW in the curative sector, which both hamper recovery towards RTW.16 ,17 Therefore, improvement of these issues became a major goal in the Netherlands.15 ,18 In addition, waiting lists hamper the referral from the occupational health service to the specialty mental health setting. To overcome these barriers, in the present study a collaborative care model with a focus on RTW was applied in the treatment of sick-listed patients with MDD by OPs in the occupational healthcare setting. Collaborative care was developed in the USA as a primary care treatment model for MDD, and the effectiveness of this treatment model in reducing depressive symptoms has been shown in many studies.19 ,20 In collaborative care, a care manager (CM) coordinates care, offers a short, structured intervention such as Problem Solving Treatment (PST) and monitors treatment progress regularly. In addition, a consultant psychiatrist is available for expert input. In the present study, a similar intervention was provided by an OP-CM in combination with a workplace intervention. The workplace intervention was aimed at eliminating barriers for RTW and involved the worker, the OP-CM and the employer.21 By combining the workplace intervention with interventions aimed at the worker (such as PST) and by having the collaborative care treatment applied by an OP-CM, the intervention in this study was expected to reduce both the duration until RTW and the severity of depressive symptoms. In a previous study among workers with common mental disorders, linking the expertise of OPs with that of a consultant psychiatrist showed promising results on reducing the duration until RTW.22 In the present study, a more comprehensive treatment model for MDD, the collaborative care model, was evaluated for its effectiveness, with a web-based tracking system and a consultant psychiatrist supporting the OP-CM. Results of this study at 3 months after baseline have been described elsewhere, showing that collaborative care was more effective than usual care in terms of response on depressive symptoms, which is a reduction in symptoms of at least 50%.23 Although no effect for collaborative care could be found on depressive symptoms as a continuous outcome measure, post hoc analyses found collaborative care to be more effective than usual care among those with moderately severe depression.23 Here the results of the 12-months follow-up are presented, reporting on the effect of collaborative care on depressive symptoms as well as on RTW.
Methods
Study design
The study is a randomised controlled trial in which the effectiveness of a collaborative care treatment for MDD was compared to usual care in the Dutch occupational healthcare setting. Randomisation took place at patient level. In both groups, the participants received sickness guidance and certification as usual by their company's OP. In addition, participants allocated to the intervention group received the collaborative care treatment from an OP-CM. Participants allocated to the usual care group were not referred to the OP-CM. In both groups, participants were free to engage in any other treatment as well. The study protocol, which is described in greater detail elsewhere, was approved by the Medical Ethics Committee and the EMGO scientific committee, both of the VU University Medical Centre.24 In the power calculation, based on response on depressive symptoms, response rates of 14.76% in the usual care group and 31.8% in the collaborative care group were assumed.19 With an α of 5% and power of 80%, 126 participants were needed in order to detect a standardised difference of 0.5 SD.24
Study population and recruitment procedures
The study was carried out within a large occupational health service in the Netherlands.
Workers on sickness absence between 4 and 12 weeks whose absence was diagnosed by the OP as due to mental disorders, were screened for depressive symptoms. The 9-item depression subscale of the Patient Health Questionnaire, the PHQ-9, was used as screener. The PHQ-9 ranges from 0 to 27 and is a reliable instrument for detecting depressive disorders and for monitoring treatment response.25 Workers who reached the cut-off score of 10 for at least moderate MDD and who gave initial informed consent were contacted by a research assistant for administration of the mini-International Neuropsychiatric Interview (MINI) by telephone.26 Sick-listed workers between 4 and 12 weeks who met the Fourth Edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for MDD according to the MINI and gave written informed consent were included in the study. Workers who were suicidal, psychotic or had a primary diagnosis of substance abuse or dependence, as assessed by the MINI, were excluded. In addition, workers with insufficient command of the Dutch language to fill out the questionnaires, those who were pregnant and those with a legal involvement against their employer, were excluded.
Randomisation and blinding
The randomisation scheme was prepared by computer, with blocks of four, by an independent statistician. While assessing eligibility for the study, both the research assistant and the participant were blinded for the allocation. Then, the participant was informed about the computer generated allocation status by the research assistant. Next, the baseline questionnaire was sent by mail. After that was filled out, the inclusion was finalised and collaborative care participants were assigned to an OP-CM. Data were collected by self-report questionnaires, in order to exclude the possibility of interviewer bias. Data entry was done by blinded assistants. Because OP-CM were only assigned to workers in the intervention group, contamination between the two groups was unlikely to occur.
Interventions
Collaborative care intervention
The collaborative care intervention, provided by the OP-CM, contained the following elements: 6–12 sessions of PST, manual-guided self-help, a workplace intervention and, depending on patient preference, prescription of antidepressant medication according to a treatment algorithm. PST is a brief, structured psychological intervention aimed at teaching the worker problem solving skills.27 The self-help manual used in this study was based on several existing self-help books and focused on cognitive restructuring, RTW and aspects of healthy lifestyle.28 The workplace intervention, in which the worker, the OP-CM and the employer participated, consisted of a workplace assessment and work adjustments. In the workplace intervention, the employer and the worker both pointed out barriers for RTW, brainstormed for possible solutions and made a plan for implementation of the solutions.21 The workplace intervention was aimed at reaching consensus about the RTW plan. Therefore, active participation and commitment of the worker and employer were essential. In the workplace intervention, the role of the OP-CM was that of process mediator. All kinds of solutions for RTW may be chosen, as long as both the worker and the employer participated in the decision process and both agree in the chosen solutions. The collaborative care treatment was closely monitored by the OP-CM, using the PHQ-9 as monitoring instrument. In order to enhance adherence to the treatment model, ongoing supervision and psychiatric consultation was provided to the OP-CMs. Also, a web-based tracking system was developed to support the OP-CM in monitoring treatment outcomes and in adhering to the stepped care protocol. In case of questions regarding the treatment, prescription of antidepressants, or (lack of) progress of the worker, the OP-CM was prompted by the web-based tracking system to consult the psychiatrist. The content of the collaborative care intervention in this study is described elsewhere more extensively.24
In accordance with the separation of treatment and sickness guidance in Dutch legislation, the collaborative care treatment and sickness guidance were separated from each other in this study. Therefore, communication between the company's OP and the OP-CM followed existing Dutch laws and guidelines and was only allowed after written informed consent by the participant.29 The OP-CMs received a 2-day training prior to the study, and supervision during the study, in order to be able to fulfil the role of CM.
Usual care
In the Netherlands, sick-listed workers start to visit the company's OP before the 6th week of sickness absence. The guidance of company's OP is protocollised according to the OP guidelines of the Dutch Board for Occupational Medicine.30 However, in practice, whether or not sick-listed workers will receive treatment for MDD may vary considerably. Therefore, the actual care that was provided was assessed by questionnaires in both groups.
Outcome measures and data collection
Data were collected by self-report questionnaires at baseline and 3, 6, 9 and 12 months after baseline. The questionnaires were returned to the Netherlands Institute of Mental Health and Addiction by mail and were processed anonymously by the researchers. Sickness absence data were derived from the register of the occupational health service 1 year after randomisation.
Primary outcome measure
Primary outcome measure in this study was time to first response on depressive symptoms. Response is defined as a reduction in depressive symptoms of at least 50%.25
Secondary outcome measures
Secondary outcome measures were time to first remission, the PHQ-9 as a continuous outcome measure and the duration until lasting, full RTW. Remission is defined as a score of less than 5 on the PHQ-9.25 The duration until lasting, full RTW was defined as the duration of sickness absence due to MDD in calendar days, from the day of randomisation until full RTW for at least 4 weeks without partial or full recurrence. In accordance with the Dutch Health Law, two sickness absence episodes with less than 4 weeks of full RTW in between, were counted as a single, continuous absence episode. Data were censored for workers whose sickness absence ended because they resigned. In addition, the total number of sickness absence days was assessed, calculated for the entire follow-up period. Post hoc, the effect was explored in participants with a baseline PHQ-9 score of at least 15.23 Finally, actual healthcare utilisation in both groups was assessed with the Trimbos/iMTA questionnaire for Costs associated with Psychiatric Illness.31
Covariates
Demographic data such as age, gender, marital status, educational level and nationality were collected. Comorbid chronic medical illness was measured with the Dutch Central Bureau of Statistics list.31 The PHQ was used to measure anxiety (including generalised anxiety and panic) and somatic symptoms.32 ,33 Job characteristics were assessed with the Job Content Questionnaire, including decision latitude, psychological job demands, physical job demands, job insecurity and social support.34
Statistical analyses
Most analyses were performed using multilevel analysis with three levels: Time to administration, participant and participant nested within OP-CM. Analyses were performed according to the intention-to-treat principle. In addition, per-protocol analyses were performed, comparing usual care participants with the collaborative care participants who actually had visited the OP-CM and examining the influence of the separate collaborative care elements (PST, antidepressant medication, psychiatric consultation and the workplace intervention) as well. The analysis of time to response and remission proceeded in two steps. First, it was examined whether the usual care group and collaborative care significantly differed from each other in the odds of not achieving remission or response, using logistic multilevel regression analysis. Second, time to remission or response were analysed for the participants who had achieved remission or response, using linear multilevel regression analyses. For an extended discussion of the coding scheme for the variables time to first remission/response, its properties and the way it was analysed using multilevel analysis see Adèr.35 The PHQ-9 as a continuous outcome measure was also analysed using linear multilevel regression analyses, using the depressive symptom severity at screening as baseline correction. The duration until lasting RTW was analysed using accelerated lifetime (log-duration) models. Covariates were considered as an effect modifier if the interaction term had a significant p value (p<0.05). The total number of sickness absence days during the entire follow-up period was compared between both groups by using the Mann-Whitney U test, performed with SPSS 15.0 software. All multilevel analyses were performed with MLwiN software, V.2.15. Propensity scores were calculated and included in all models to correct for possible selection bias.
Results
Participants and baseline characteristics
The recruitment of participants lasted 22 months. During that period, 14.595 workers sick-listed between 4 and 12 weeks due to psychological causes were screened for depressive symptoms. Three hundred and sixty-eight workers refused to participate. A total of 2955 workers (20.2%) participated in the screening, of which 52.5% (N=1551) screened positive for depression. Of the screened-positive workers, 1425 workers were excluded for various reasons, which are shown in figure 1. Finally, 126 participants were included in the study and were randomised in the usual care group (N=61) or the collaborative care group (N=65). Baseline characteristics of the participants are shown in table 1. With regard to the self-report questionnaires, the loss to follow-up rates at 3, 6, 9 and 12 months were respectively 22.2%, 28.6%, 33.3% and 41.3%. Both groups did not differ significantly from each other on the loss to follow-up rates (p>0.05).
Baseline characteristics of the participants*

Flowchart of participants.
Depressive symptoms
Collaborative care participants did not differ significantly from usual care participants in the odds of not achieving remission or response (p>0.05; CI −0.281 to 1.353). For participants who achieved remission, the average time to first remission was 6.5 months in the collaborative care group (N=27/65) and 7.9 months in the usual care group (N=29/61). However, this difference was not significant. Collaborative care participants did differ significantly from usual care participants in the time to response (p<0.05; 95% CI −1.684 to −0.027). For the participants who achieved response, the average time to response was 5.0 months in the collaborative care group (N=15/65), and 7.8 months in the usual care group (N=14/61). Table 2 shows the mean PHQ-9 scores of the collaborative care group and the usual care group at baseline and at 3, 6, 9 and 12 months after baseline. Both groups did not differ significantly from each other on the continuous measure on any of the follow-up measurements. The interaction effect that was found previously at 3 months after baseline, showing that collaborative care was more effective than usual care among those with moderately severe depression, was not found for the subsequent follow-up measurements.23
Depressive symptoms in the study population
Return to work
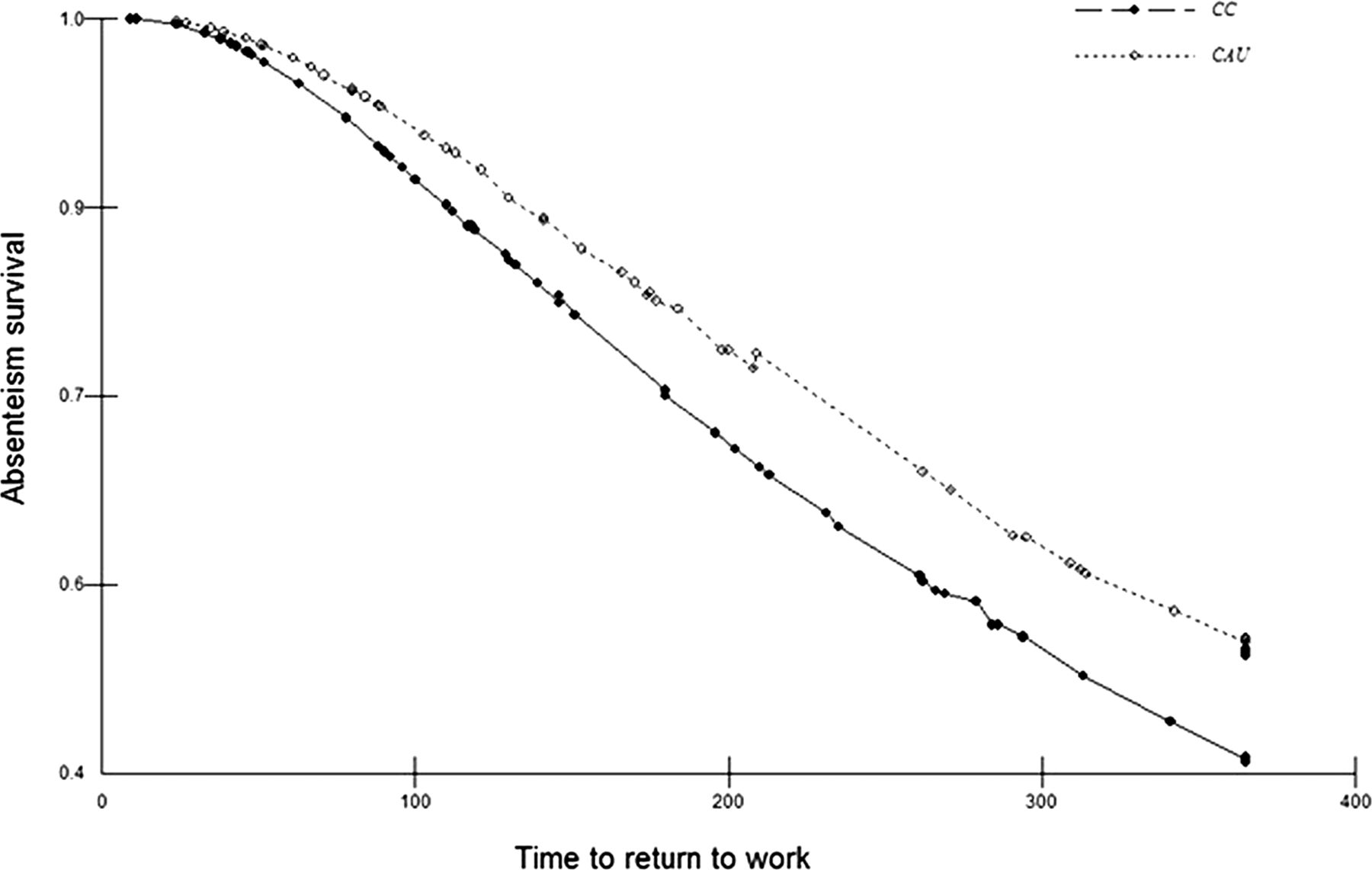
Within 1 year follow-up, 64.6% of the collaborative care participants and 59.0% of the usual care participants had achieved lasting, full RTW. The mean duration until lasting, full RTW, calculated from the day of randomisation, was 190 days (with a SD of 120 days) in the collaborative care group, and 210 days (with a SD of 124 days) in the usual care group. In the collaborative care group, 13.8% of the participants (N=9) were censored because they resigned, compared with 13.1% of the participants (N=8) in the usual care group. Figure 2 shows the survival curve. The results of the accelerated lifetime (log-duration) model showed that the two groups did not differ significantly from each other in the duration until lasting, full RTW (B=−0.198, SE=0.234, p>0.05; 95% CI −0.657 to 0.261). The mean number of sickness absence days in the entire follow-up period was 198 in the collaborative care group (SD 120 days) and 215 in the usual care group (SD 118 days) and did not differ significantly between both groups (p>0.05).
{kind=link}
{kind=link}
Survival curve.
Interventions
The healthcare utilisation within 12 months after baseline was assessed in both groups by questionnaire.31 The proportions of participants that had had contact with the different healthcare professionals are presented in table 3. In most cases, usual care involved contact with the OP (87.3%), the general practitioner (GP, 89.1%) and a mental health professional (83.6%). In the collaborative care group, the majority of the participants visited the OP (89.1%), the GP (83.6%) and a mental health professional (78.2%). Compared with the collaborative care group, more participants in the usual care group had received day treatment for mental health problems (14.5% vs 1.8%).
Healthcare utilisation in the study population within 12 months after baseline†
Treatment integrity
In the collaborative care group, almost two-thirds of the participants (N=40/65) visited the OP-CM and started collaborative care treatment including PST. For 17.5% of those (N=7/40), the psychiatrist was consulted by the OP-CM and 47.5% of them (N=19/40) used antidepressant medication. The workplace intervention was applied in 12.5% of the participants who visited the OP-CM (N=5/40). Objections by both the worker and the OP-CM were reported as reasons for not applying the workplace intervention, indicating that both did not feel comfortable with applying this intervention within the depression treatment. During the recruitment of participants, waiting lists of workers occurred due to a lack of available OP-CMs. On average, the collaborative care treatment started 29 days after randomisation, with a SD of 16 days. Mean duration of the collaborative care treatment was 82 days, with a SD of 49 days.
Per-protocol analyses
In the per-protocol analyses, collaborative care participants who visited the OP-CM (N=40) were compared with usual care participants (N=61). The per-protocol analyses did not result in different findings than the intention-to-treat analyses. On average, collaborative care participants who had visited the OP-CM and received PST only, had had their first response at 3.5 months after baseline, which was significantly faster than usual care participants (p<0.05; 95% CI 0.148 to 2.442). Collaborative care participants who had visited the OP-CM did not differ significantly from usual care participants in the duration until RTW (B=−0.305, SE=0.316, p>0.05; 95% CI −0.924 to 0.314). Receiving additional collaborative care elements, such as antidepressant medication or psychiatric consultation, did not result in a shorter duration until first response or a shorter duration until RTW.
Discussion
Main findings
With regard to depressive symptoms, over the entire follow-up period, collaborative care did not lead to more treatment response among sick-listed workers with MDD than usual care. Nevertheless, collaborative care was more effective than usual care in reducing the time to response. The time to response was significantly shorter, with a difference of 2.8 months in favour of collaborative care. No difference was found between the two groups in terms of the time to remission or on the PHQ-9 as continuous outcome measure. Also, collaborative care was not found to be superior to usual care in reducing the duration until lasting, full RTW.
Interpretation of results
Despite that collaborative care reduced the time to response, the results of this study can be interpreted as modest since the intervention did not have an effect on the duration until RTW, on the odds on response and remission and on the continuous outcome measure. As was reported elsewhere, collaborative care was more effective than usual care in terms of response at 3 months after baseline.23 The present findings, that collaborative care led to a faster response but not to more response, suggest that collaborative care did have an immediate effect, but that this effect decayed during the 12-month follow-up. These results need to be interpreted in view of the poor implementation of the collaborative care intervention in this study. First, a substantial number of collaborative care participants did not start the collaborative care treatment, because waiting lists occurred of participants waiting for the treatment to start. Ironically, the idea to move treatment to the occupational healthcare setting in order to avoid waiting lists for referral to the specialty mental health setting created waiting lists and lack of treatment in the occupational healthcare setting. Perhaps it was not realistic to expect physicians to provide an intervention of this magnitude. Moreover, because of the separation of treatment and sickness certification in the Dutch legislation, workers may not be used to the treatment role of the OP-CM, which may have inhibited them as well in visiting the OP-CM. Second, despite training and close supervision of the OP-CMs, the workplace intervention was applied to a low extent, thereby eliminating the most important contrast in the intervention aimed at RTW. It may have felt unsafe for workers to be guided in the workplace intervention, with also the employer participating, by the OP-CM who also provided their depression treatment. In addition, the OP-CMs as well felt uncomfortable with the workplace intervention in their treatment role. Perhaps the workplace intervention would have been better implemented if a different occupational health professional, such as a company social worker or a labour expert, would have guided the workplace intervention.36 Interestingly, a difference in mean duration until RTW of 20 days was found in this study, in favour of collaborative care. Although this difference was not significant and SDs in the RTW durations were large, it may be a relevant difference. Particularly since 80% of the costs of MDD are due to production losses, reducing the duration until RTW in this population has the potential to accomplish important cost savings.37 Moreover, with respect to RTW, this study may have been underpowered. In studies on RTW, hazard rates of 2.0 are often assumed, based on studies in workers with low back pain.38 However, for workers with mental health disorders, particularly those with MDD, RTW may be more difficult than for workers with low back pain. As a consequence, smaller HRs and larger sample sizes may be applicable.39 Thus, given the poor implementation of the intervention and the underpowered sample size in the present study, we cannot conclude that collaborative care is not effective in the occupational healthcare setting. However, the poor implementation suggests that, although patients recovered faster from depressive symptoms, the model as operationalised here does not attain the results wanted in terms of RTW in practice and that the (implementation of the) intervention protocol needs adaptation before larger studies are performed.
Comparison with other studies
To our knowledge, this was the first study examining the effectiveness of collaborative care in sick-listed, depressed patients, aimed at reducing the duration until RTW and the depressive symptoms. Compared with other studies in the Dutch working population, our participants had comparable levels of depressive symptom severity and durations of sickness absence.5 ,12 ,22 In a meta-analysis, collaborative care was shown to be more effective when CMs have a specific mental health background, which was not the case in our study.20 Also, studies with all three elements of collaborative care (a CM, physician and consultant psychiatrist) tend to be more effective than studies with less fidelity to the original collaborative care model.20 Although our study included three roles (the company's OP for the regular sickness guidance, the OP-CM for the collaborative care treatment and the consultant psychiatrist), these were implemented differently in our study than in the collaborative care studies in primary care. In a previous study, it was found that psychiatric consultation provided to the OP resulted in a faster RTW.22 However, in that model, the OP did not try to provide curative treatment himself, but referred for this purpose to the GP. Therefore, the combination of treatment by the OP and psychiatric consultation does not seem to be an improvement in comparison to the simpler psychiatric consultation model. In a recent study among workers with chronic low back pain, the workplace combined with a graded activity programme reduced sickness absence with a median of 120 days, compared to usual care.38 In another study, the workplace intervention was evaluated among sick-listed workers with distress.39 In that population, the workplace intervention only reduced the duration until RTW in the subgroup of workers who had at baseline the intention to RTW despite still having symptoms.39 Unfortunately, that interaction effect could not be examined here, since the intention to RTW despite still having symptoms was not measured in our study. Moreover, evaluating the added value of the workplace intervention is not possible in this study since that intervention was applied in only a few participants.
Strengths and limitations
This was an innovative study, aimed at reducing both the depressive symptoms and the duration until RTW in depressed, sick-listed workers. However, the poor implementation and underpowered sample size for RTW prevents us from drawing firm conclusions on the effectiveness of collaborative care in the occupational healthcare setting. Nevertheless, there was a significant difference in favour of collaborative care in terms of time to response and a non-significant difference in duration until RTW, indicating that there may be grounds to further explore the model in future research.
Implications for practice and further research
The results of this study do not justify a widespread implementation of collaborative care, as it was operationalised here, in the occupational healthcare setting. Although collaborative care had a positive effect on the time to response, collaborative care did neither have an impact on RTW, nor on the odds on response or remission and the PHQ-9 as continuous outcome measure. However, this study was probably underpowered with respect to RTW and therefore, larger studies are recommended. Moreover, since treatment integrity was low, future studies in occupational healthcare need to operationalise collaborative care differently. The dual focus on RTW and depressive symptoms remains important in the treatment of depressed, sick-listed workers, but it needs to be examined how that focus can be best put into practice. As seems from this study, it is not wise to combine both strategies in one intervention by one OP. Future research may focus on improving referral to, and monitoring of, adequate treatment by OPs and on improving collaboration between OPs and the curative sector.
Acknowledgments
This study was part of the Depression Initiative, a national programme aimed at supporting depression care in the Netherlands.
References
Footnotes
-
Contributors CFC was the principle investigator of the study, she participated in conducting the study and in data analyses and in writing this article. HJA conducted data analyses and participated in writing the article. JRA participated in the design of the study and in conducting the study and advised on data analyses and on writing the article. RH advised on the design of the study, participated in the coordination of the study and advised in writing the article. WvM participated in the design of the study and advised on the data-analyses and on writing the article. ATFB participated in the design of the study, and gave advice on data-analyses and on writing the article. MCV participated in the design of the study, conducted the study and data-analyses and wrote the article. All authors read and approved the final manuscript.
-
Funding This study was funded by the Foundation for Innovation of Health Insurers ('Innovatiefonds Zorgverzekeraars’) in the Netherlands.
-
Competing interests MCV: Received a payment from Achmea Schade & Inkomen, 365/ArboNed and Lundbeck B.V. for the printing of her PhD thesis. CFC: The Trimbos-institute received funding for the study from the Foundation for Innovation of Health Insurers (‘Innovatiefonds Zorgverzekeraars’), received payment for a presentation at the JIC conference, received grants for Collaborative Care trials for anxiety (from the Netherlands organisation for health research and development, ‘ZonMw’) and for return to work (from Achmea), and received a payment from Eli Lilly for a lecture on diabetes and depression. CFC received royalties for books on psychiatry. HJA: Received a fee from the Trimbos-institute for consulting on the statistical analyses and comments on the draft manuscript. JRA: Is shareholder of a VU University Medical Center spin-off company, Evalua Nederland B.V. (http://www.evalua.nl). RH: None. WvM: Is director-shareholder of a VU University Medical Center spin-off company, Evalua Nederland B.V. (http://www.evalua.nl). ATFB: received grants for research support from Eli Lilly, Astra Zeneca, Jansen, and Shire; and as a speaker from Eli Lilly and Lundbeck.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Ethics approval Medical Ethics Committee of the VU University Medical Center in Amsterdam.
-
Data sharing statement The Netherlands institute of mental health and addiction is owner of all available data from this study.