Article Text

Abstract
Although limited evidence is available, organisational change is often cited as the cause of mental health problems. This paper provides an overview of the current literature regarding the impact of organisational change on mental health. A systematic search in PUBMED, PsychInfo and Web of Knowledge combining MeSH search terms for exposure and outcome. The criterion for inclusion was original data on exposure to organisational change with mental health problems as outcome. Both cross-sectional and longitudinal studies were included. We found in 11 out of 17 studies, an association between organisational change and elevated risk of mental health problems was observed, with a less provident association in the longitudinal studies. Based on the current research, this review cannot provide sufficient evidence of an association between organisational change and elevated risk of mental health problems. More studies of long-term effects are required including relevant analyses of confounders.
- Organisational change
- mental health
- psychosocial environment
- psychology
- organisation of work
- post-traumatic stress disorder
- psychiatry
- epidemiology
- sickness absence
Statistics from Altmetric.com
- Organisational change
- mental health
- psychosocial environment
- psychology
- organisation of work
- post-traumatic stress disorder
- psychiatry
- epidemiology
- sickness absence
Introduction
The last decade has brought increased attention to the possible detrimental effects of work on mental health. Existing research has focused on work strain and occupational health and found consistent evidence for associations.1 Organisational change is often cited as a harmful exposure but few studies have been published to support this assumption.2–6 One of the first studies on health risks was a study from Finland7 where they found that the risk of health problems was at least two times greater after major downsizing than after no downsizing. A longitudinal study published few years later found a significantly faster decline in self-rated health even 4 years after downsizing among employees who had experienced major downsizing.8 The increase in health problems was partially explained by concomitant increases in physical demands and job insecurity and a reduction in job control.8 ,9 Besides, downsizing and repeated exposure to rapid personnel expansion may predict long-term sickness absence and hospital admissions.10 Although these studies did not specifically address mental health problems, they should be interpreted within the framework of work stress.
Employees are increasingly confronted with frequent minor daily stressors related to changes in technology and workplace practices as well as the major upheavals of mergers, downsizing and restructuring.11 ,12 The imminence, duration and temporal uncertainty surrounding events of change can have a negative impact on employees.13 Indeed, the increased uncertainty regarding job future or the direction of organisational change has been suggested to be a principal cause of stress.14 ,15 Others propose that organisational change acts as a stressor through the individual's negative appraisal of the changes.16
The well-documented risks that might follow organisational changes are: intensification of job strain, time pressure, reduction of social support, lack of control and role ambiguity, which all have been associated with mental health problems.17–19 Two systematic reviews of psychosocial factors at work and depression found evidence of a relation between perceived psychosocial job strains and an elevated risk of depressive symptoms or major depressive episode.20 ,21 Job insecurity has also been consistently linked with detrimental mental health effects in both meta-analysis and reviews.22 ,23 Another potential factor affected by organisational change: job dissatisfaction has shown strong associations with depression and anxiety according to meta-analysis.24 Examining organisational change as a potential work stressor yields a certain benefit because organisational change is more tangible in nature than for instance change in meaningfulness of work is to the individual. Empirically it is possible to determine whether or not a change has happened and whether or not the employees are feeling worse (or better) hereafter.
The health effects of workplace reorganisation in intervention studies have previously been reviewed by Egan et al25 and Bambra et al26 who found small evidence for beneficial effects of increased employee participation and control. However, the reorganisation that occurs in intervention studies is typically aimed at addressing unhealthy environments, which is different from the economic motives of, for example, company downsizing.
Therefore, the objective of this paper is to provide a systematic review of observational studies on associations between organisational change and employee mental health problems.
Methods
The review was conducted in accordance with the PRISMA statement.27
Eligibility criteria
Participants
The study population of interest was individuals employed in companies undergoing some sort of organisational change. Relevant comparators were either employees not exposed to change or employees exposed to different levels or types of changes.
Exposure
Our definition of organisational change was inspired by Rafferty's definition of transformational change and refers to modifications made to the core systems of an organisation including traditional ways of working, values, structure and strategy. Transformational changes can either be changes to the normal operational procedures (tasks, working hours) or changes in the system itself (eg, downsizing, changing the organisation's hierarchy or incorporating a new organisational system).28 Only studies with organisational change explicitly listed as the primary exposure were considered.
Outcome
This review was limited to studies examining mental health problems, specifically with a focus on depression, anxiety and stress. All health variables had to be measured by validated scale or based on diagnosis made by a mental health professional. Conversely studies where the outcome measured was readiness for change, commitment to change, coping with change or job satisfaction after change were not included.
Study design
We focused on observational studies and in the case of duplicate publications of data from the same study, the paper with the most relevant analysis and risk estimate was chosen.
Information sources
A series of computerised librarian-assisted systematic searches were undertaken in PubMed, PsycInfo, Excerpta Medica Database (EMBASE), EBSCO Business Source Complete and Web of Knowledge using a broad search strategy to find peer-reviewed articles of relevance. The searches were carried out using MeSH terms (medical subject headings) or free text when no MeSH term was available, and limited to English journal articles with abstracts. To find the most recent articles not yet indexed by MeSH terms, free text words were included for the period 2010-search date. The searches were performed in October 2011. Organisational change was operationalised in the search strategy as ‘organizational change’, ‘organizational innovation’, ‘organizational restructuring’, ‘organizational transition’, ‘work change’, ‘downsizing’ and ‘reorganization’. The search terms for mental health problems were ‘anxiety’, ‘depression’, ‘mental disorders’, ‘mental health’, ‘stress’, ‘occupational stress’ and ‘psychological stress’. Search terms were derived from keywords and titles of known core papers.
Study selection
Initial eligibility assessment of titles was performed by the first author (SGB) under careful supervision of senior researcher ØO. Both ØO and SGB screened articles by abstract. Difficult judgements on relevance among reviewers were resolved by consensus.
Data collection process
Data were extracted systematically from each study following a standardised format. Data were extracted by SGB under supervision of ØO. Information was extracted on: (1) Participants: (including nationality, sample size, type of organisations, work type, controls); (2) Exposure (type of organisational change); (3) Type of outcome measure (mental health problems using validated scale or other type of diagnostic tool); and (4) Study aim and design, follow-up time, statistical analysis used, adjustments, bias and conclusion/results.
Results
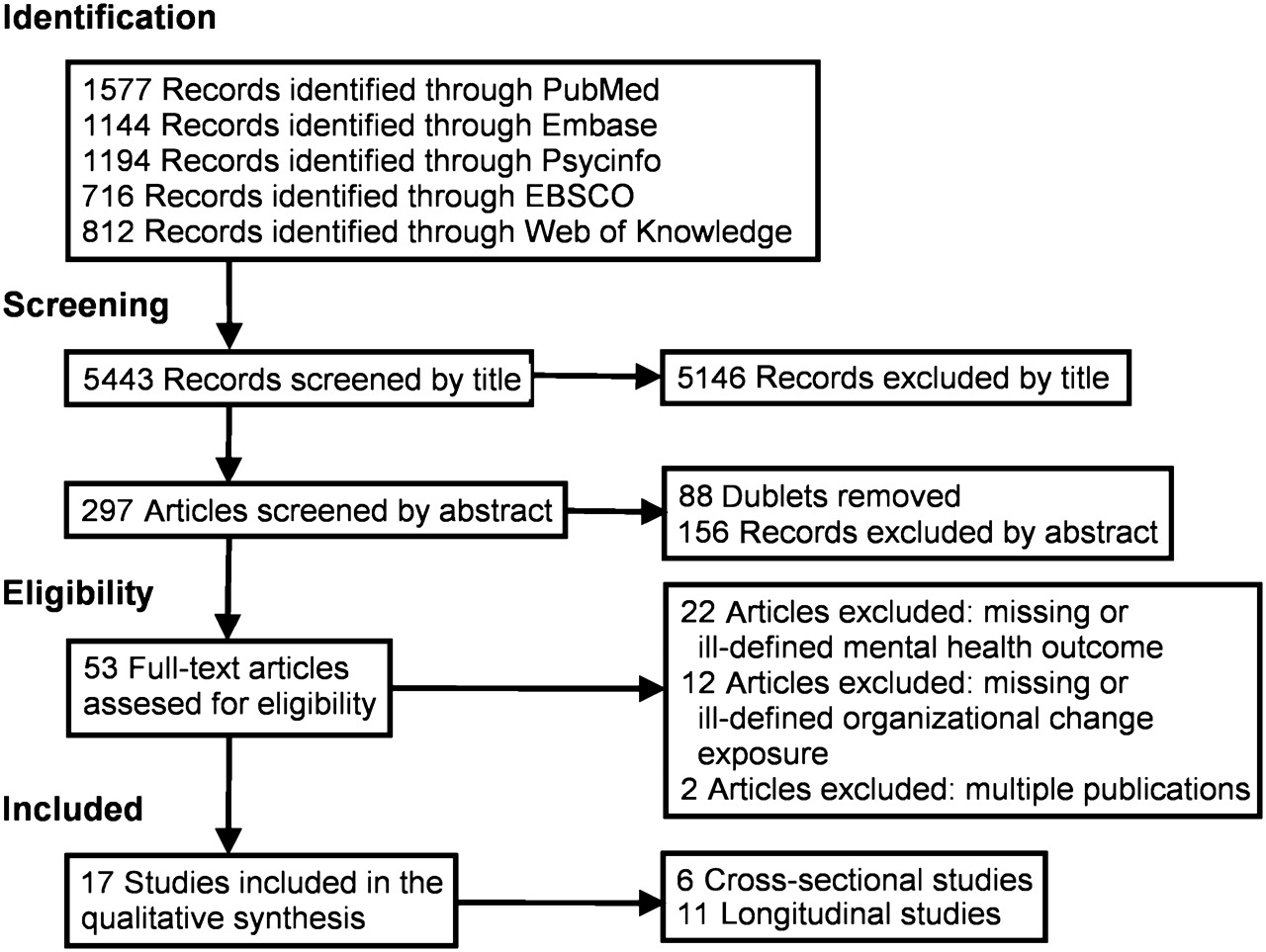
The search strategy yielded 5443 records, which were screened for relevance based on title by one of the authors (SGB) and 5146 records were excluded. A duplicate search was performed and further 88 articles were removed. At step two the remaining 209 records were screened by abstract by SGB and ØO, and 156 records were removed. The reasons for exclusion was missing or ill-defined mental health outcome (57 studies), theoretical articles (22 studies), lack of organisational change as exposure (20 studies), intervention studies (17 studies), coping studies (17 studies), duplicate publications of data from same study (five studies), managers as study population (four studies) and otherwise irrelevant study design (14 studies).
At step three 53 full text articles were assessed for eligibility and 17 articles were included in the final synthesis. The reasons for exclusions were missing or ill-defined mental health outcome (22 studies), missing or ill-defined organisational change as exposure (12 studies), and duplicate publications of data from same study (two studies). The selection process is depicted in figure 1.

{kind=link}
Flowchart of the number of articles in different stages of the selection strategy.
Descriptive statistics of the 17 eligible studies included in the review are listed in table 1. Six studies used a cross-sectional design29–34 and 11 were longitudinal.2 ,3 ,35–43 All but three studies2 ,32 ,43 were published within the last 10 years. The included studies involved 40 993 participants, excluding the population and registry studies30 ,35 ,37 which accounted for a total of 142 110 individuals. Besides the three large studies of the general working population, hospital staff and civil servants were the most frequent study subjects (table 1).
Studies of organisational change and mental health problems
Data were primarily collected by questionnaire, though two studies were strictly registry based,35 ,37 three studies used structured interviews29 ,30 ,41 and finally one study36 collected blood samples. The studies had a mean baseline response rate of 64%, with three studies below 50%3 ,39 ,43 and one longitudinal study3 was even below 20%; however, this was partly redeemed by a high retention rate. The median follow-up time of the longitudinal studies was approximately 2 years (ranging from 1 to 7). Four studies assessed participants twice36 ,39–41 and four studies2 ,3 ,38 ,43 assessed them thrice, while one study assessed participants a total of four times.42 The two remaining longitudinal studies were registry based and contained annual information from a 6-year35 and 7-year period.37
Various types of organisational change were assessed in the 17 studies ranging from major changes like downsizing, mergers and reorganisations to lesser (though perhaps not less intrusive) job content changes. Downsizing as the best described exposure was analysed in two cross-sectional studies30 ,33 and three longitudinal studies.37 ,38 ,41 The three longitudinal studies37 ,38 ,41 examined different degrees of contact with downsizing over time, that is, exposure–response relationships. One of the cross-sectional studies33 used downsizing ratio as the exposure that is also a type of exposure–response study. The last downsizing study30 simply examined the exposure–effect relationship of downsizing on mental health. Two longitudinal studies examine the effect of company mergers39 ,42 while two other longitudinal studies3 ,35 examined the effect of multiple types of organisational changes both quantitatively and qualitatively. Restructuring was assessed in one cross-sectional study29 and three longitudinal studies.36 ,40 ,43 Finally, job changes were examined by one longitudinal study2 and three cross-sectional.31 ,32 ,34
Only one study42 used clinical psychiatric criteria (International Classification of Disease) to define the mental health outcome. The remaining studies primarily relied on self-rated questionnaires or registry information to determine the mental health effects. Depression31 ,32 ,38 ,39 ,41 ,43 and anxiety31 ,41 ,43 were the most specific mental health problems reported; however, all the studies utilised different measurement scales. One study37 used the ambiguous ‘psychotropic drug use’ as mental health indicator. Finally, a large part of the studies relied on the vague term ‘distress’29 ,33–36 or general measures of self-rated mental health2 ,3 ,30 ,33 ,40 as indicators of mental unbalance. Due to the disparity of the outcome data extracted from the studies and the heterogeneity of the outcome we chose not to perform a meta-analysis or any other type of data synthesis.
Most of the studies2 ,3 ,29–32 ,34 ,35 ,37–39 ,42 adjusted results for socio-demographic factors such as age, gender, marital status and education. Work-related factors such as employment status and different job characteristics were less commonly adjusted for.2 ,3 ,29–31 ,35 ,37 ,39 ,42 Only three studies adjusted for personality traits like type A behaviour,29 neuroticism3 or sense of coherence.42 Though there is evidence of exacerbated risk of reoccurrence of mental health problems like depression,44 only three studies3 ,40 ,42 analysed for effects of previous mental health status. Five studies33 ,36 ,40 ,41 ,43 did not adjust results for any possible confounders. Almost all of the studies lacked a non-respondents analysis and for the longitudinal studies analysis of attrition.
Associations between organisational change and mental health problems were found in five29–32 ,34 of the six cross-sectional studies. The remaining study33 found no association between downsizing rate and mental health effects, but did report lower mental health scores than national norm for all participating study sites. The longitudinal studies presented mixed results as only six out the 11 studies3 ,35 ,37 ,41–43 found associations between exposure to organisational change and subsequent mental health problems, and one study2 only found significant effects for men.
Three30 ,37 ,41 out of five of the studies on downsizing found an association between mental health problems and exposure, and of these two37 ,41 studies were longitudinal. In two29 ,43 out of four studies on restructuring an effect on mental health was observed, and of these studies one was longitudinal.43 The two negative studies36 ,40 were both longitudinal. The effects of mergers on mental health have been analysed in two studies.39 ,42 Netterstrøm et al39 did not find an association between mergers and depression while Väänänen et al42 found an association between the exposure and postmerger psychiatric events. Concerning the studies on exposure to multiple types of organisational changes both studies3 ,35 found an association with negative health effects. All four studies on job changes2 ,31 ,32 ,34 found an association between the exposure and mental health problems; however, in one study this association was only evident for men.
Discussion
Despite the broad search profile we found few studies which analysed the association between organisational change and mental health. A total of 17 studies were found eligible for this review, surprisingly few considering the high number of records initially evaluated by title, a finding experienced by others.2 ,3 An association between exposure to organisational change and decreased mental health was found in 11 out of the 17 studies with a less provident association in the longitudinal studies. This might be explained by an observed acute short-term effect on mental health during the actual change process that later disappears or normalises over time such as the results by Dahl suggest.35 Another reason for the discrepancy could be that the mental health impaired has already left work, or have not the energy to participate in such a study. None of the longitudinal studies provide drop-out analyses to counter this argument; however, three studies3 ,40 ,42 at least take previous mental health status into account. The prospective cohort study by Kivimäki et al37 included all employees who were at work before downsizing. The use of psychotropic drugs was examined in employees who kept their jobs after major downsizing and among those who lost their jobs during the downsizing, compared with the employees who did not experience downsizing. This strategy specifically allowed examination of the role of drop-out in the results.
An important aspect all but three of the studies33 ,34 ,42 omit is the employees' individual perception of change. The individual categorisation of a specific organisational change as threatening or not is connected to the psychological reaction. This process can be influenced by several factors like coping strategies,45 negative affectivity,46 stress prior to change,47 perceived social support48 or length of employment.49 Personal characteristics such as personality type, temperament, intelligence and genetic constitution may all affect the way in which an individual understands and reacts to life experiences. Mental health problems can take years to develop but the studies explore a snapshot of a particular time period.50 The effect of these confounding factors may influence the estimate. Kivimäki et al37 also notes that survival bias may prevent detection of the adverse effects of work, as major psychiatric disorders are commonly related to work disability and, furthermore, a potential selective factor for unemployment.
Recall bias may influence the results as employees who experienced organisational change as traumatic might be more inclined to remember the experience than employees who were less affected. In relation to this, utilising self-reported data like Verhaeghe et al34 introduces the risk of circular reasoning51; those who rate the organisational change as stressful are the stressed employees. In a broader perspective this approach addresses the issue whether organisational change really is harmful in itself, or if merely the employees' individual perception of the change makes it harmful. This type of bias is avoided in population studies where the exposure (typically downsizing) is determined by registry data. These types of studies, however, provide little information on the actual process of implementing the organisational change. Research into change processes suggests that the readiness for organisational change and the subsequent healthiness of the change process may reduce the experience of stress and increase the employees' abilities to cope with the changes,45 ,52 ,53 that is, mediate or even moderate the change effect. Due to the number of different workplaces included in the population studies no specific information on the change process is reported. Furthermore, there is a risk of misclassification when organisational change is assessed at workplace level, as the particular change may have affected only parts of the organisation. Therefore, it would be preferable to use an independent measure of exposure in these studies.
Additional risk of misclassification is related to the possible effect of preceding organisational changes. This could skew the results in either way making the employees more vulnerable or resilient to mental health problems.38 Pepper et al33 noted that downsizing (as well as merger) is usually a change existing in a complex network of events. This would add to the likelihood of concomitant organisational changes such as restructuring or contract changes making it harder to measure the effect of downsizing as an independent exposure and increasing the risk of misclassification. Another important aspect emphasised by Dahl35 is the rationale behind companies' change in the first place. He hypothesises that employees might be experiencing increased stress because their firms are poor performers trying to regain momentum by implementing organisational change. Thus, the mental health problems are related to the companies' poor performance and not the organisational change itself. If job insecurity is a central component in the pathway between organisational change and mental health problems as suggested,14 ,15 ,23 then organisational changes in branches or industries with high competition might be at further risk. Indeed, the results of Dahl35 suggest that performance variables influence the effect of change on stress; however, this needs to be further examined.
Limitations
The epidemiologic evidence this review provides is limited mainly due to the low number of published relevant studies. Second, the definition of organisational change is at best vague including both major and minor changes to the organisation and work environment. To some extent, we compare the effect of major downsizing30 ,33 ,37 ,38 ,41 and work schedule rearrangement2 ,32 ,34 as being equal.
Subsequently, the definition of mental health as outcome is also marred by confinements. Limiting mental health to minor psychiatric disorders and not just mental discomfort narrows the available material considerably. Numerous studies otherwise relevant use job security, job satisfaction and morale as psychological outcome which can be relevant in other contexts but hardly describe mental health on a psychiatric level.54–61 The most optimal mental health outcome would be diagnosis by psychiatrist; however, we had to settle for registry data, self-reported data or proxies like psychotropic drug use and stress hormone levels.
Several of the studies were cross-sectional leaving out any causality from the conclusions. However, it could be argued that it is probable that poor psychosocial work environment could be a reason to implement job changes and doubtful that the employee's mental health status is the cause of the major changes like downsizing and mergers.31
In three3 ,36 ,38 of the included studies there is a high risk of confounding. The study by Hansson et al36 identifies hormone markers of mental distress, but fails to define valid baseline hormone levels. The analysis does not control for individual differences in cortisol awakening response, seasonal and diurnal variation, and lifestyle factors such as intake of coffee and alcohol, smoking and physical exercise.62 Moore et al38 comment in their discussion that due to small cell sizes, the results should only be regarded as exploratory, which is a conclusion we support. The study by Loretto et al,3 otherwise solid, has a low response rate (18.4%) and no analysis of non-responders. The results might, therefore, be heavily biased. However, for the majority of the studies2 ,29 ,31 ,32 ,35 ,37 ,39 ,41–43 we have no reason to believe that the results were confounded in such a degree that the associations would be altered significantly. Taken this into account and restricting the analyses to 14 studies with no major confounding errors, 10 studies29–32 ,34 ,35 ,37 ,41–43 report a positive association between organisational changes and mental health, one study2 reported an association for men but not women and finally three studies reported no association.33 ,39 ,40 However, this restriction would alter the effect on the estimate increasing the positive association from ∼65% including all 17 studies to ∼71% when limited to the 14 studies. Both numbers are significantly lower than the ratio of 85% positive studies that Quinlan and Bohle23 reported in their 2009 review on health and safety effects of downsizing and job insecurity. However, Quinlan and Bohle23 included a wider array of (softer) outcomes and considered job insecurity an exposure in itself, and consequently their ratio is not directly comparable with the ratio found in this study.
Conclusion
The exposure variables are multi-dimensional, and have been described, evaluated or measured differently. Multiple study designs have been used and the size of the population analysed has varied substantially. The outcomes in the analyses are inconsistent and similar outcomes have been defined differently among the studies. In 11 out of 17 studies an association between organisational change and elevated risk of mental health problems was observed, with a less provident association in the longitudinal studies. Given the heterogeneity of the studies, and the large number of cross-sectional studies this review cannot provide convincing evidence of an association between organisational change and elevated risk of mental health problems. The studies are scarce and the findings should be considered with great care. Further analysing is needed to determine if the observed effect is of temporary or of more persistent nature. More studies with relevant analyses of confounders are recommended.
What is already known on this subject
The psychosocial work environment affects the mental health of employees.
Perceived psychosocial job strains elevate the risk of depressive symptoms, anxiety and work stress.
Organisational change is related to temporal increase of job insecurity.
What this paper adds
The first systematic review of the association between organisational change and employee mental health problems.
No convincing evidence of an association between these was found; however, studies are scarce and results should be considered with care.
Acknowledgments
We wish to thank Hjørdis Rasmussen who helped with the literature search.
References
Footnotes
Funding This research was financed by grant: 20080053113/12-2008-09 from the Foundation for Research of Work Environment (Denmark). The funders played no part in the conduct or reporting of the research.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.