Article Text

Abstract
Objective Knowledge on the time-course (trends) of work-related asthma (WRA) remains sparse. The aim of this study was to describe WRA trends in terms of industrial activities and the main causal agents in France over the period 2001–2009.
Method Data were collected from the French national network of occupational health surveillance and prevention (Réseau National de Vigilance et de Prévention des Pathologies Professionnelles (RNV3P)). Several statistical models (non-parametric test, zero-inflated negative binomial, logistic regression and time-series models) were used and compared with assess trends.
Results Over the study period, 2914 WRA cases were included in the network. A significant decrease was observed overall and for some agents such as isocyanates (p=0.007), aldehydes (p=0.01) and latex (p=0.01). Conversely, a significant increase was observed for cases related to exposure to quaternary ammonium compounds (p=0.003). The health and social sector demonstrated both a growing number of cases related to the use of quaternary ammonium compounds and a decrease of cases related to aldehyde and latex exposure.
Conclusions WRA declined in France over the study period. The only significant increase concerned WRA related to exposure to quaternary ammonium compounds. Zero-inflated negative binomial and logistic regression models appear to describe adequately these data.
- Asthma
- occupational exposure
- statistical models
- trend
- work-related asthma
- epidemiology
- occupational asthma
- cancer
- retrospective exposure assessment
- respiratory
- cardiovascular
- statistics
- mortality studies
- mathematical models
- legal
- occupational health practice
- musculoskeletal
- back disorders
- preventive medicine
- mineralogy
- lung function
- exposure assessment
- cross-sectional studies
- man-made mineral fibers
- asbestos
- silicosis
- pneumoconioses
- mesothelioma
- allergy
- OH services
- male reproduction
- health surveillance
- clinical medicine
- biological monitoring
Statistics from Altmetric.com
- Asthma
- occupational exposure
- statistical models
- trend
- work-related asthma
- epidemiology
- occupational asthma
- cancer
- retrospective exposure assessment
- respiratory
- cardiovascular
- statistics
- mortality studies
- mathematical models
- legal
- occupational health practice
- musculoskeletal
- back disorders
- preventive medicine
- mineralogy
- lung function
- exposure assessment
- cross-sectional studies
- man-made mineral fibers
- asbestos
- silicosis
- pneumoconioses
- mesothelioma
- allergy
- OH services
- male reproduction
- health surveillance
- clinical medicine
- biological monitoring
What this paper adds
Knowledge on temporal evolution of work-related asthma remains sparse according to main agents and industrial sectors.
Based on the ‘French national network of occupational disease surveillance and prevention’, this study documents an overall decrease of work-related asthma over the period 2001–2009, particularly for cases in relation with aldehyde, latex or isocyanate exposures. Conversely, a significant increase was observed for cases associated with occupational exposure to quaternary ammonium compounds, mainly in health and social sector.
Clinicians have to be aware of the trend of main causes of work-related asthma.
Introduction
Work-related asthma (WRA) is generally defined as a type of asthma caused (ie, occupational asthma (OA)), or exacerbated, when it exists prior to exposure (work-exacerbated asthma (WEA)), by a particular work environment.1 OA has now become one of the most common occupational lung diseases in many industrialised countries. For instance, it has been estimated that the population attributable risk for occupational exposure and asthma ranges from 10% to 25%2 and may be as high as 29% (95% CI 25 to 33), when considering new-onset asthma in adults over 18 years.3 On the other hand, a 2003 ATS statement4 on the occupational contribution to the burden of airway disease reported that WEA might account for ‘much greater morbidity’ than OA.
Most knowledge on OA is derived from cross-sectional studies, involving numerous specific industrial activities or agents, the most frequently investigated, among many others, being car painting (isocyanates), woodworking, healthcare professions (latex, aldehydes) and baking (flour dust).5 WEA has been associated with various irritant environments.6
More recently, population-based registries have provided new findings on the epidemiology of WRA, with emerging risks related to the use of cleaning or hairdressing products.7 However, few data are available to describe the time-course (trend) of the disease, globally and within specific activities. One study reported an overview of trends in Finland, but with some limitations due to the small number of cases, that allowed the description of only a limited number of sectors.8 Another study, based on SWORD data, reported a slight decrease for WRA over the 1996–2005 period, depending on the reporting physicians.9 Two other studies described the trends of OA in healthcare workers (HCWs)10 and workers exposed to laboratory animals.11 Most of these studies only reported crude evolution of cases, sometimes based on non-parametric statistics or time-series analyses. However, more sophisticated methods are warranted in order to take into account bias such as variations of denominator (active workforce by example) or sources (reporter fatigue).9 In this area, recent methodological papers provided interesting tracks using incidence rate-ratio9 or zero-inflated models.12
Finally, trend analysis is a questionable approach, as several biases can be encountered9 in this type of health surveillance system.
This study was designed to describe recent trends in the incidence of WRA with respect to industrial activities and the main causal agents, in France, over the 2001–2009 period, based on a population-based national occupational health network. Several statistical approaches to measure trends were also compared.
Methods
Overall design
The French national network of occupational health surveillance and prevention (Réseau national de vigilance et de prevention des pathologies professionnelles (RNV3P)) has been described elsewhere.13 Briefly, this network comprises all 32 occupational health departments located in French University Hospitals. Patients with suspected work-related disease are referred to these centres, mainly by occupational physicians (about 60% of all cases) and by general practitioners or specialists (about 20% of all cases). Since 2000, experienced occupational physicians in these departments systematically complete standardised forms for each patient referred. Data are systematically recorded in a nationwide database. Recorded information includes the main diagnosis and comorbid diseases (ICD-10), main occupational exposure and four other possible agents, occupation (ISCO-88, edited by ILO) and sector of industrial activity (NAF, edited by INSEE). The strength of the association between a disease and each suspected causal agent is rated by the medical expert on a four-class scale (nil, possible, probable and certain). The quality of data is optimised by the use of a computerised tool for entering, coding and monitoring data consistency, annual training in quality assurance for users, the creation of a national coding group and centralised quality controls.
Cases included
Data analysed in this study were exported from the national database after excluding cases with incomplete data. Data from the first year of recording (2000), which were considered not to be representative of annual collection, were also deleted. Only reports concerning WRA (ICD-10 J45.0 to J45.9), with at least a probable or certain association with one occupational agent, were included. Agents were coded according to their chemical identification and/or their common use according to a classification established by four of the authors (JA, LB-C, DD and CP).
Statistical analysis and trend analysis
Overall, the incidence of WRA for a given year was defined as the number of observed cases in the validated national database. The proportion of a specific occupational exposure (namely a causal agent, an industrial activity or a combination of these two variables), for a given year, was defined by the ratio of the number of outcomes relative to all subjects with WRA.
Four methods were used for trend calculation (see online appendix I).
First, we calculated the non-parametric Kendall rank correlation test between year and number of cases for selected agents and sectors. This method is considered to be the reference method, as it does not require any distribution hypothesis by definition.
Second, we adapted the method described by McNamee et al9 to our data. Briefly, this paper reported annual incidence trends of some forms of work-related dermatitis and respiratory diseases in the UK. This study was based on data collected monthly, from 1996 to 2005, by three groups of reporting physicians all over the country. Changes in annual incidence were estimated using a two-level (hierarchical) Poisson regression model, with gamma-distributed random effects. The dependent variable was the number of cases, including zeros, per reporting physician, per month. These analyses estimated annual percentage change in incidence over the time span of the study, based on the assumption that change was constant from year to year. Although this assumption is not true, this estimate can be considered to be an approximate measure of average change or trend. If rate denominators are constant over time, then the ratio of case counts from one calendar year to another can be interpreted as an incidence rate ratio and can be plotted as a function of the year. In our study, we replaced the Poisson model by a zero-inflated negative binomial (ZINB) regression model.12 The negative binomial model allows for greater variation than the Poisson model. The zero-inflated version allows the possibility of excessive zero counts in the data. In our study, the dependent variable was the number of cases per month and the covariables were the seasons (winter, spring, summer and autumn) and year considered as categorical variables. The reference season was summer, and the reference year was 2004. We checked that these arbitrary choices did not have any impact on the trends of our data.
The third method used a time-series approach, based on the fact that if a trend was present, then it would be observed on the time-series plot of the number of cases per month. Consequently, we modelled the number of cases by month for all the survey and graphically represented the simple-linear trend. As a result, this approach was only descriptive.
Finally, we calculated the reporting odds ratio (RoR).14 In this approach, we chose the proportion of WRA cases associated with a specific exposure relative to all other cases in 2004 as reference. We then assessed OR associated with each other year according to the variation of the presence of this exposure in cases, using a logistic regression model. The trend was then tested by a Kendall rank correlation test between ROR and years.
The results from the four methods were compared for selected agents, chosen on the basis of a p value <0.20 obtained with the first approach (Kendall rank correlation test). As no formal tests are available to compare these different models, discussion on model comparisons was based on a qualitative approach considering values of correlation coefficients and their p values, agreement between results and graphical comparisons from different models.
Statistical analyses were performed on SAS V.9.2 and R software.
Results
The study sample comprised 2914 cases of WRA, including 1689 men (58%), with a median age of 40 and approximately the same age in men and women (40.3 and 39.5 years, respectively) (table 1). However, significant differences by gender were observed for the main industrial activities.
Characteristics of the population by gender (n=2914)
Overall, a significant decrease was observed in the global number and in the number of recorded cases in men alone, over the years (table 2 and supplement figure E1a). A significant decrease was also observed in the number of cases with a link considered to be definite between exposure and disease (see supplement figure E1b). WRA cases decreased in most industrial sectors, albeit this decrease was significant only in some sectors (manufacture of food products, p=0.012; manufacture of plastic products, p=0.011; manufacture of basic metals, p=0.027; manufacture of fabricated metal products, p=0.006; personal service activities, p=0.025). On the other hand, an increase of WRA cases, albeit non-significant, was observed in general service sectors, particularly in the education and public administration sectors.
Annual distribution of work-related asthma (WRA) cases according to gender, strength of the association with exposure and selected industrial activities
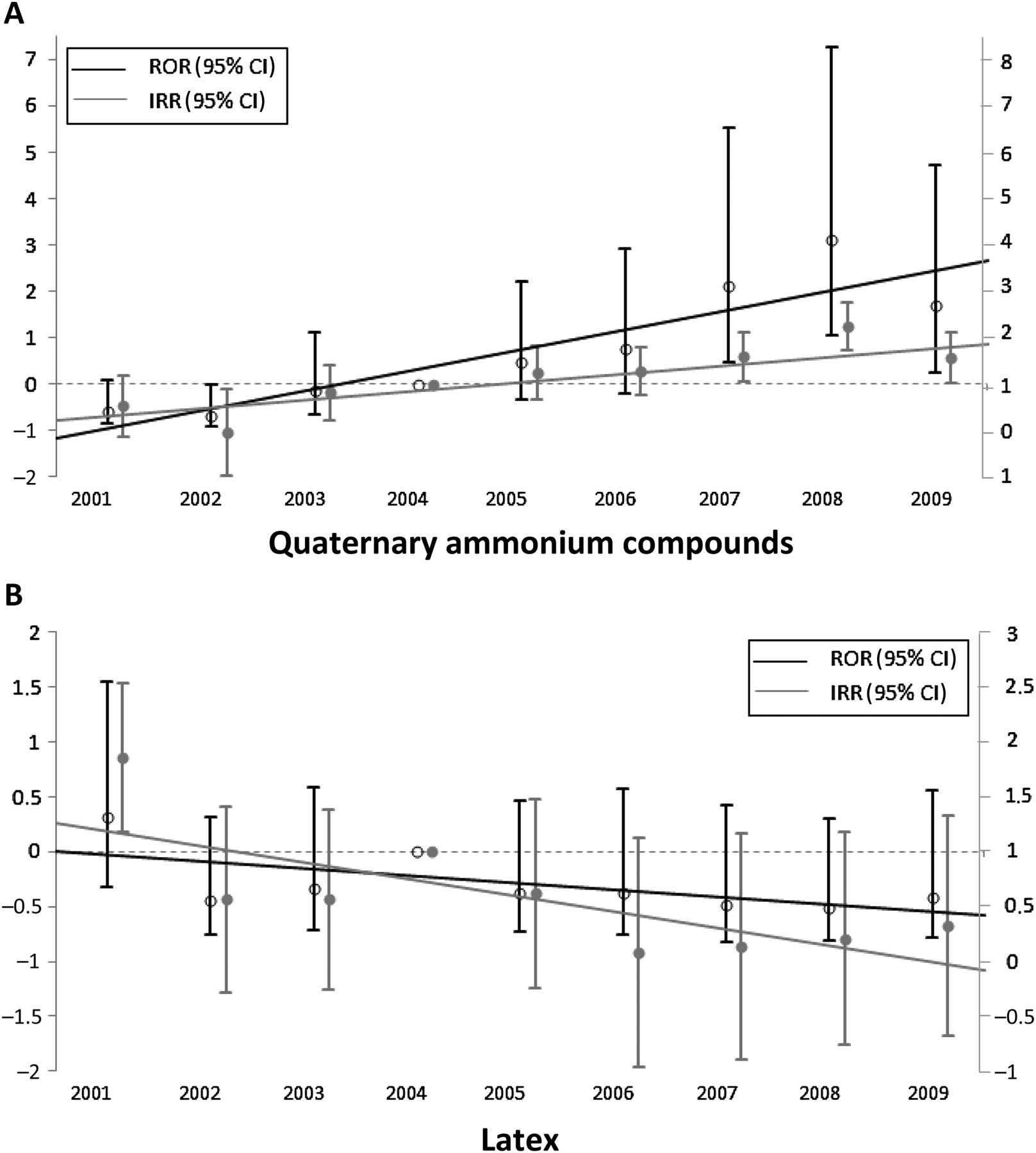
Analyses by causal agents (table 3) showed that only WRA related to exposure to quaternary ammonium compounds (used as sterilising or cleaning agents) increased significantly over the observation period (p<0.003). A slight (but non-significant) increase was also observed for cleaning products other than quaternary ammonium compounds (p=0.451) (figure 1A). Conversely, agents such as aldehydes, wood, flour, isocyanates, various metals and latex (figure 1B) significantly decreased over the observation period. Analyses combining industrial sectors and causal agents (table 4) provided additional information. In particular, an increase of WRA linked to quaternary ammonium compounds was observed in HCW, whereas a significant decrease in the number of cases associated with aldehyde use and an almost significant decrease for latex were observed in this occupational activity sector, Interestingly, trends appeared to be different from one sector to another for the same agents. For instance, a significant (or almost significant) decrease was observed with flour in industrial settings and sales sectors but not in the catering industry.
Annual distributions of work-related asthma (WRA) cases by selected causal agents and trend tests, based on Kendall rank correlation test

{kind=link}
(A) Comparisons of incidence rate ratio (IRR) and reporting odds ratio (ROR) for work-related asthma (WRA) to quaternary ammonium compounds. ROR was obtained using a logistic regression model, and IRR was obtained using the zero-inflated negative binomial (ZINB) model. All models took year 2004 as reference. ROR, Kendall correlation test: +0.833, p=0.001; IRR, Kendall correlation test: +0.340, p<0.001. (B) Comparisons of IRR and ROR for WRA to latex. ROR was obtained using a logistic regression model, and IRR was obtained using the ZINB model. All models took year 2004 as reference. ROR, Kendall correlation test: −0.666, p=0.012; IRR, Kendall correlation test: −0.402, p<0.001.
Annual distributions of work-related asthma (WRA) cases by selected causal agents according to selected industrial sectors and trend tests
Comparative approaches using the four models for trend estimates are presented in online supplement table E1. Overall, no marked discrepancies for trend estimates were observed between the four methods. An increased incidence of WRA due to quaternary ammonium compounds and a decreased incidence due to aldehydes and latex were confirmed by the four methods. Cleaning products other than quaternary ammoniums were associated with a slight rise, only with the Kendall rank correlation test based on RORs (p=0.037), whereas other methods also demonstrated a positive but non-significant trend. Interestingly, the incidence rate ratio and RORs showed fairly similar graphical patterns (figure 1 and online supplement tables E2 and E3).
Discussion
This study documented an overall decrease in the number of WRA cases, in France, mainly in men, over the observation period. However, this decrease was not homogeneous. A significant decrease was observed for some agents such as isocyanates, aldehydes and latex, while a significant increase was observed for quaternary ammonium compounds and possibly for cleaning products other than quaternary ammoniums. Concerning industrial activities, some sectors showed contrasting trends, such as health and social work, with a decrease of WRA related to latex and aldehydes but an increase of WRA related to quaternary ammonium compounds.
First of all, the validity of these trends needs to be discussed, as many causes may interfere with time-courses. The diagnosis of OA is complex and a structured approach has been proposed comprising key steps.15 Overall, no major diagnostic method, developed over the last 10 years, has dramatically changed the epidemiology of OA.16–18 At the same time, the definition of OA for compensation purposes in France remained unchanged over the period, and the same global decreasing trend was observed from 2003 to 200819 for OA compensation. We can therefore assume that progress in diagnostic procedures cannot explain the decreased incidence of WRA in our study. Trends may also be related to changes in industrial activities in France. Overall, changes in industrial activities represented <1% of the total active population for all main activity sectors, except for ‘other manufacturing sectors’ (−1.8%) and ‘education sector’ (−1%).20 Thus, although we cannot rule out that observed changes could be partly related to changes in the numbers of workers in various industrial activities, the order of magnitude of the changes is insufficient to explain our results. The inclusion rate among centres during the study period also needs to be discussed. In contrast with many other surveillance programmes, case reporting was systematic and mandatory in our network, on the basis of the financial contract with both Sécurité Sociale (French National Health Insurance) and the Agence nationale de sécurité sanitaire de l'alimentation, de l'environnement et du travail (French National Food, Environment and Work Health Safety Agency) (‘ANSES’). Consequently, the decreased number of reported cases was unlikely to be attributed to fatigue, which avoids a major bias in trend assessment. Finally, statistical interpretation of these trends is questionable. Both Kendall statistics and ZINB models are only based on case numbers and do not depend on the proportion of WRA cases to overall reported cases, in contrast with logistic regression models. However, the results were consistent for most agents with these three methods and we decided to only interpret those results not presenting any discrepancies. The existence of a difference between the true number of WRA cases and the number of patients referred to the centres, resulting in case under-reporting, is often described for this type of population-based registry. We can assume that this is also true for our data collection and that our cases were not representative of the French population. The possibility of referral to one of our centres may also vary according to industrial sector. We tested the possible role of centres by introducing the 32 centres as variables in the ZINB regression models for overall trend of WRA. This approach did not modify our results and the trends were confirmed. The same results were obtained with multilevel logistic regression models, with centres as random variable (data not shown). Under-reporting may also influence rate estimates by sectors, which is why we did not calculate the corresponding rates, but they may have only a minor impact on time trends.9
Finally, we are confident that the trends observed in this study reflect the course of WRA in France, although we cannot rule out that some particular trends may reflect centre-dependent changing practices in relation to the diagnosis of WRA.
Previous studies have reported an increased incidence of OA in industrialised countries21 but with no clear data concerning recent trends,8 17 as very few longitudinal WRA incidence data are available. A non-significant decrease of WRA was reported by occupational physicians in the SWORD programme9 for the 1995–2005 period (−1.9%, 95% CI −5.2% to −1.4%). Piipari and Keskinen,8 in Finland, also reported a decrease of OA, for the 1995–1998 period, mainly in cases due to animals, flour and grain and, to a lesser extent, chemical compounds (isocyanates), followed by a plateau. Conversely, an increase was observed for moulds and hairdressing during the same period. In France, the ONAP (Observatoire National des Asthmes Professionnels) programme reported a non-significant increase of cases of OA over a 4-year observation period between 1996 and 1999.22 This programme also suggested an increased incidence for hairdressing and cleaning products, particularly in women.
The trends observed in the present study are in line with data of the recent literature reporting certain specific risk factors for WRA. It is well known that HCWs frequently experience WRA, as these workers are exposed to numerous allergens or irritants.23 24 Vandenplas reported that modification of gloves policies, with decreased use of powdered latex gloves,10 has resulted in a decrease of latex-induced OA, in agreement with our results and a recent meta-analysis.25 The present study also demonstrated that WRA in HCW is now often related to quaternary ammonium compounds, used for general disinfection at work and in hospitals for infection prevention rather than aldehydes or latex.
We report a possible increase of WRA due to cleaning products. This association has already been reported by several authors.26 27 However, although no trends could be calculated, these compounds appeared to be also involved in sectors such as public administration and educational services, as they were the agents most frequently founds in these sectors (data not shown). We also observed a significant decrease in WRA, mainly due to chemical compounds, such as isocyanates, confirming previously published reports.22 However, no clear explanation can be provided for these phenomena between deindustrialisation and prevention effects. Some other activities, such as hairdressing, another well-known cause of asthma,28 did not show any significant trend. These findings may be related to the low statistical power due to the small sample sizes, particularly for activity/agent combinations. On the other hand, if correct, these results also underline the need to complete prevention efforts against possible new causes, as well as better known classical agents.
This study presents certain limitations and a number of strengths. Despite the publication of several statements on OA diagnosis,1 29 persistent discrepancies are observed concerning the diagnosis of OA by clinicians.30 Consequently, differences in diagnostic procedures may exist between centres31 both for OA and WRA. Moreover, the absence of specific challenge test procedures in most centres prevented us from distinguishing between WEA and OA with a reasonable level of confidence. Taken into account, the strength of causality does not modify our findings (data not shown). In particular, analyses restricted to associations described as ‘definite’ did not markedly alter our results, and we hypothesize that these results may be applied to OA as well. Obviously, this particular point needs more in-deep investigations. Moreover, the real influence of all these discrepancies on the observed trends is difficult to determine.
Compared with most other studies in the field, based on questionnaires, referral to occupational physicians for the diagnosis of each case of asthma is an important strength of this study. Comparisons with other medical surveillance programmes, involving general practitioners, occupational physicians or chest physicians, are therefore difficult and may not be appropriate. In a recent study, Turner et al32 demonstrated that although the level agreement was only fair between occupational and chest physicians, no systematic errors were observed. Consequently, these findings only apply to France. One of the interesting findings of this study is confirmation of the value of the measure proposed by McNamee for trend assessment and the possibility of using logistic regression models, rather than Kendall correlation tests.
In summary, we report a negative trend in the number of WRA cases, in France, over the 2001–2009 period. Despite certain limitations inherent to the study design, the results of this study show that trends in the distribution of WRA causal agents are not homogeneous across industrial sectors or causal agents. The most prominent finding is the significant increase of WRA related to quaternary ammonium compounds observed in well-known high-risk sectors such as health and social sectors. Attention would be addressed in other sectors where these products are also widely used such as Education and Personal Service Activities. Comparisons of trends based on ZINB or logistic models with Kendall correlation tests were found to be useful and demonstrated good consistency.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
RNV3P members: Angers (Roquelaure Y., Petit A.), Amiens (Doutrellot-Philippon C.), Bobigny-Avicenne (Guillon F.), Besançon (Aptel M., Thiebaut A.), Bordeaux (Rinaldo M., Verdun-Esquer C.), Brest (Dewitte J.D., Lodde B.), Caen (Clin B., Marquignon M.F.), Cherbourg (Marquignon M.F.), Clermont-Ferrand (Chamoux A., Dutheil F.), Créteil (Pairon J.C., Andujar P.), Dijon (Smolik H.J.), Garches (Ameille J., d'Escatha A.), Grenoble (de Gaudemaris R., Bonneterre V.), Le Havre (Gislard A., Rollin L.), Lille (Frimat P., Nisse C.), Limoges (Druet-Cabanac M.), Lyon (Bergeret A., Normand J.C.), Marseille (Lehucher-Michel M.P.), Montpellier (Roulet A.), Nancy (Paris C., Penven E.), Nantes (Géraut C., Dupas D.), Paris-Cochin (Choudat D., Bensefa-Colas L.), Paris-Hôtel-Dieu (Léger D., Prevost Balensi E.), Paris-Fernand Widal (Garnier R., Villa A.), Poitiers (Ben-Brik E., Berson C.), Reims (Deschamps F., Lesage F.X.), Rennes (Verger C., Gouyet Ahu T.), Rouen (Gehanno J.F.), Saint-Etienne (Fontana L., Pélissier C.), Strasbourg (Cantineau A., Nourry N.), Toulouse (Soulat J.M., Hérin F.), Tours (Lasfargues G., Haguenoer K.).
Funding This network was funded by the French Agency for Food, Environmental and Occupational Health & Safety (Anses), the National Health Insurance system for employees (CNAM-TS), the French Occupational Medicine Society (SFMT), the National health insurance system for agricultural workers (CCMSA) and the French Institute for Public Health Surveillance (InVS).
Competing interests None.
Patient consent Obtained.
Ethics approval Agence Nationale de Sécurité Sanitaire, Alimentation, Environnement, Travail.
Provenance and peer review Not commissioned; externally peer reviewed.