Article Text

Abstract
Objectives To examine the efficacy of early intervention on the prevention of long-term sickness absence and major depression among employees at high risk of future sickness absence and with mild to severe depressive complaints.
Methods Randomised controlled trial conducted among employees working in an office environment. 139 employees were identified both at high risk of future sickness absence and with mild to severe depressive complaints through screening. Subsequently, they were randomly assigned to the intervention group (n=69) or the control group (n=70). Objective sickness absence was analysed at 12 and 18 months of follow-up. Depressive complaints were assessed by the Beck Depression Inventory (BDI-II) at baseline, and at 6 and 12 months of follow-up.
Results Intention-to-treat analyses showed a significant difference in total sickness absence duration between the intervention (27.5 calendar days (SD 44.7)) and control group (50.8 days (SD 75.8)) over 12 months of follow-up, a reduction of 46% (p=0.017). The intervention group showed a non-significantly lower proportion of long-term sickness absence spells compared with the control group (p=0.127). Statistically significant and clinically relevant differences in depressive complaints were found after both 6 months (p=0.001) and 12 months (p=0.005) of follow-up, in favour of the intervention group. Relative risk reductions (RRR) were 19.2% and 19.8% respectively. Sickness absence data were available for all participants over 18 months of follow-up. Questionnaire data were available for 99 (at 6 months) and 90 participants (at 12 months). No adverse events or side effects occurred.
Conclusions Early intervention in employees with mild to severe depressive complaints and high risk of future long-term sickness absence proved to be effective in preventing/reducing both sickness absence and depressive complaints.
- Randomised controlled trial
- prevention
- sickness absence
- epidemiology
- mental health
- intervention studies
- preventive medicine
- sickness absence
Statistics from Altmetric.com
- Randomised controlled trial
- prevention
- sickness absence
- epidemiology
- mental health
- intervention studies
- preventive medicine
- sickness absence
Introduction
What this paper adds
Work rehabilitation in case of sickness absence due to mental health complaints remains very difficult, and symptom reduction does not necessarily lead to work resumption.
A previous study on a preventive strategy aimed at early intervention among employees identified at high risk of future sickness absence proved effective in the prevention of long-term sickness absence.
Depressive complaints are highly prevalent in the working population and are associated with future long-term sickness absence.
Preventive intervention among employees identified both at high risk of future sickness absence and with mild to severe depressive complaints proved effective in the prevention/reduction of long-term sickness absence and depressive complaints.
The next step will be further implementation of the preventive strategy in the occupational health setting.
Mental health problems are highly prevalent in the labour force and constitute a source of marked distress and social impairment for the employee.1 2 Major depression is considered to be one of the more severe disorders, making up a substantial part of the mental health problems.3 Recent studies showed that depressive complaints are also prevalent in the working population on a relatively mild level.4 5 Over time, these depressive complaints may exacerbate and result in major depression.6 Depressive complaints are found to be often associated with work disability and long-term sickness absence and increased healthcare use.7 8 Work disability and especially long-term sickness absence have also increasingly been recognised as considerable public health problems, with consequences for employers and society.9 So far, work rehabilitation in case of sickness absence due to mental health complaints remains very difficult, and symptom reduction does not necessarily lead to work resumption.10 11 Conversely, sickness absence can cause and predict depressive complaints.12 13
From an occupational healthcare perspective, before treating employees with major depression or treatment of employees who are already on sick leave, a preventive strategy aimed at prevention of major depression and long-term sickness absence through early intervention might be more effective. A prerequisite for such a strategy is the ability to identify employees at high risk of future long-term sickness absence and with mild depressive complaints. To identify employees at high risk of sickness absence, a screening questionnaire, called Balansmeter in Dutch, was developed in 1998.14 The Balansmeter proved to have good properties in predicting long-term sickness absence. In an additional study by Kant et al5 conducted in 2003, it was demonstrated that early intervention among employees at risk of sickness absence proved effective in reducing future sickness absence. The current study, including a new RCT, focused on both high risk of sickness absence and depressive complaints. It was hypothesised that early intervention is effective in preventing depressive complaints and/or future sickness absence.
Numerous studies have investigated the effectiveness of different treatments for depression.15 16 Strong evidence exists that cognitive behavioural therapy (CBT) and problem-solving therapy (PST) are effective treatments for depression.17–20 CBT and PST have also been proven effective in reducing sickness absence.21 22 A new protocol specifically targeted at employees, who are identified both at high risk of sickness absence and with mild to severe depressive complaints, was developed based on CBT and PST, with the main focus on work-related problems. The aim of this RCT is to examine the efficacy of this new protocol among employees identified at high risk of long-term sickness absence and with mild to severe depressive complaints on the prevention of future long-term sickness absence and major depression.
Methods
Study design, procedure and participants
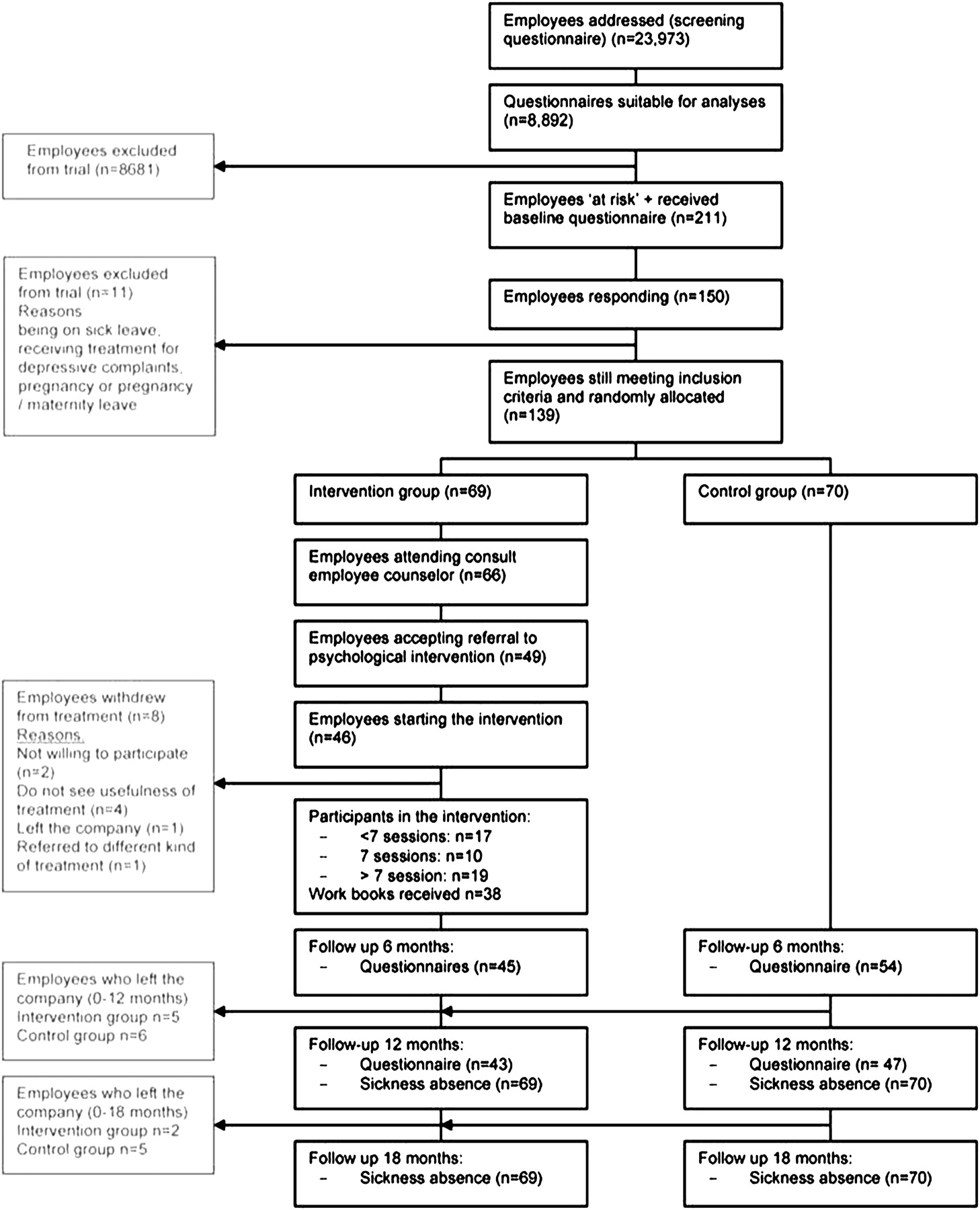
A randomised controlled trial (RCT) was conducted among employees of a large banking company in The Netherlands. Figure 1 presents the selection process of the study. In 2007, 23 973 employees received a screening questionnaire at their home address. In the invitation letter, employees were asked to provide written informed consent, which covered the usage of questionnaire data, the company data on sickness absence and the possibility of participating in the trial. In total, 9157 employees (38.2%) responded to the questionnaire; 8892 questionnaires were suitable for analyses, and 265 were discarded due to technical reasons or because no informed consent was provided. Employees identified at risk of sickness absence and with mild to severe depressive complaints (n=211) received an extensive baseline questionnaire (T0). Exclusion criteria were being (fully or partially) absent from work, pregnant or on pregnancy/maternity leave or receiving treatment by a psychologist/psychiatrist, at the time of completing the screening questionnaire. Employees who responded to the baseline questionnaire (n=150) and still met the selection criteria (n=139) were randomised into the intervention (n=69) or the control group (n=70). Randomisation sequences were generated using computerised random number generators (block size 2) by the principal investigator (ML), based on employee personnel numbers. Company counsellors and psychologists were not blind to group allocation. However, they were only aware of participants of the intervention group. Follow-up questionnaires were sent at 6 and 12 months after randomisation to assess depressive complaints and secondary outcomes. Objective sickness absence data were assessed at 12 and 18 months of follow-up. The study was covered by the medical guidelines of the occupational health service, thereby ensuring all participants' privacy and anonymity. The study was approved by the Medical and Ethical Committee of Maastricht University (MEC 06-3-018). The study was performed according to the Declaration of Helsinki.
{kind=link}
Flow diagram of recruitment, allocation and outcome assessment.
Preventive intervention
The intervention consisted of a psychological treatment based on the principles of PST and CBT. The main goal of the intervention, which had an individual orientated approach, was to offer guidelines to enhance problem-solving skills in order to prevent long-term sickness absence and to reduce depressive complaints and to stimulate personal well-being. The intervention was specifically developed for our target population by four experts in the field of psychology. A treatment protocol and workbooks for practical assignments were developed for the trial based on two main sources.23–26 The focus of the protocol was on employees with relatively mild complaints and who were still at work. The intervention was preventive because of its timing, treatment before sickness absence occurs and because it focused on relatively mild complaints. Therefore, the intervention consisted largely of PST. CBT/PST often consist of 10 to 12 sessions. This new intervention consisted of a basic part and a specific part. The basic part contained seven sessions of 45 min each, based on the major steps of PST. Through all sessions, principles of CBT were applied. The seventh session consisted of an evaluation session. Since it was unknown at the start of the study if seven sessions would be sufficient for every participant, the intervention could be extended with a maximum of five sessions. In the seventh session, the psychologist and employee decided in consultation to end treatment in case the participant had recovered or to move on with the specific part of the protocol. For the specific part, the employee could indicate the subject to focus on during the sessions, such as training of social skills or cognitive restructuring. At the end of each session, homework assignments were given which were discussed in the next session. The intervention was conducted by 10 psychologists from a company consisting of a nationwide network of registered psychologists (Cenzo BV). This company regularly provides psychological healthcare for the banking company. The psychologists received 2 days of training before the study started and a 1-day booster session during the study. Participants in the control group received care as usual from the occupational health services. Care as usual when the employee asks for help included consultation with an occupational physician and, if necessary, referral to other disciplines. Care as usual in case of sickness absence included social medical counselling.
Measurements
Screening measures
Risk of sickness absence
The Balansmeter, developed in 1998 for employees working in an office work environment, was used to identify employees at high risk for future long-term sickness absence. The Balansmeter was developed and internally validated on data of the Maastricht Cohort Study and was externally validated in 2003 on a large sample of employees of the same company at which the current RCT was conducted.14 For the present study, a cut-off point with 87.9% specificity and 52.6% sensitivity in women and 87.8% and 65.1% in men was applied.
The BM includes risk of sickness absence in general, not necessarily due to depressive complaints. A second measure was included to assess depressive complaints.
Depressive complaints
Presence and severity of depressive complaints were assessed using the depression scale of the Hospital Anxiety and Depression Scale (HAD Scale). The HAD Scale is a 14-item self-report questionnaire, which was originally developed to indicate the presence and severity of both anxiety (HAD-A) and depression (HAD-D) separately.27 28 With respect to the cut-off values, we used the values suggested by Zigmond et al.28 A higher score on HAD-D indicates more severe depressive complaints. Employees were defined as having mild to severe depressive complaints when they scored 8 points or higher on HAD-D.
Primary outcome measures
Sickness absence duration
Sickness absence duration was measured objectively (in calendar days) through record linkage on an individual level with the company registers on certified sickness absence from 2 months after employees received the screening questionnaire until 18 months of follow-up. Long-term sickness absence was defined as a sickness absence spell lasting for more than 28 consecutive days. Sickness absence was assessed for 12 and 18 months of follow-up. Measurement of sickness absence started 2 months after completing the screening questionnaire. This is in line with the development of the Balansmeter.14 Returning and processing of the questionnaires could at most take 2 months.
Depressive complaints
Depressive complaints are viewed as a continuous spectrum of complaints, ranging from no to severe depressive complaints, with major depression at the end of the spectrum. While the screening instrument included the HAD Scale, to assess severity of depressive complaints more extensively the commonly used Beck Depression Inventory-II (BDI-II) was used.29 For our focus on relatively mild complaints, the BDI-II was too extensive and included too ‘heavy’ items, on for example suicidal thoughts, to include in the screening questionnaire. We therefore included the BDI-II in the baseline questionnaire and at 6 and 12 months of follow-up. Scores on the BDI-II can range from 0 to 63, with higher scores indicating more severe depressive symptoms.30 Scores from 0 to 13 points were defined as not/minimally depressed, 14–19 points as possibly/lightly depressed, 20–28 as moderately depressed and 29–63 points as severely depressed.29 31
Secondary outcome measures
Data on secondary outcome measures were gathered by means of self-administered questionnaires at baseline, and at 6 and 12 months of follow-up.
Self-rated health
Self-rated health was assessed with one item from the Short Form Health Survey (SF-36), widely used to measure general health status.32 33 ‘In general, would you say your health is’. This item was scored on a five-point scale (1=excellent, 2=very good, 3=good, 4=moderate, 5=bad). The Brief Symptom Inventory (BSI), a short version of the Symptom Checklist 90 (SCL-90), was used to measure general psychological distress, with higher scores indicating a higher degree of symptoms (range 0–212).34 35 Scores on HAD-D at 6 and 12 months of follow-up were defined as a secondary outcome measure.
Work characteristics
A validated Dutch version of the Job Content Questionnaire was used to measure psychological job demands, decision latitude and social support at work.36 Additional data on job insecurity and commitment were gathered with questions adapted from the Questionnaire on the Experience and Evaluation of Work (VBBA).37
Cointerventions
Cointerventions in the past 6 months, such as treatment by a general practitioner, an occupational physician, a psychologist, a psychiatrist or a company counsellor and the use of medication (including antidepressants, sleeping medication, tranquillisers, painkillers or other) were assessed by self-report.
Treatment adherence
For each participant in the intervention group, it was assessed whether the intervention was conducted according to the protocol. Adherence to the protocol was defined as being exposed to all essential predefined steps of the intervention. For the per-protocol analyses, those participants who received at least one treatment session were included, which is a rather conservative approach.
Power calculation
In calculating sample size, sickness absence was chosen as the main outcome measure of the study. Based on sickness absence data from the Maastricht Cohort Study on fatigue at work, it appeared that 60% of employees with psychological complaints were absent from work for at least 2 weeks over a period of 12 months of follow-up.2 The assumption was that the intervention would be effective by reducing this percentage to 35%. Power calculation, using a two-sided significance level of 5% and a power of 80%, indicated a minimum of 59 participants in each group. Taking into account a potential attrition of 15%, a final sample size of 136 should be sufficient.
Statistical analysis
First, data were analysed according to the intention-to-treat principle. Difference scores on continuous outcomes were used for both sickness absence (0–12 months and 0–18 months) and depressive complaints (T0–T1 and T0–T2). To estimate the efficacy of the intervention, Poisson regression analysis was used for the outcomes sickness absence duration and sickness absence frequency. Risk ratios were calculated for dichotomous outcomes. Linear regression analysis was used for continuous outcomes, adjusted for baseline differences. Multivariate Cox regression analysis was used to test differences in time to onset of the first sickness absence spell. Clinically meaningful changes on the BDI-II were determined by calculating the Reliable Change Index as developed by Jacobson and Truax.38 This approach is based on two components: reliable change, that is a decrease of at least 7 points; and clinically significant change, that is post-treatment score below 14.29 31 Chi-square tests were used to test frequency differences in reliable and clinically significant change.
Second, for the per-protocol analyses, outcomes were compared between those employees who received at least one treatment session and the control group.
All analyses were performed using SPSS version 15.0, Stata statistical software package 8.0 and SAS.
Results
Participants
Figure 1 presents a flow chart of the study. Recruitment started in February 2007 and was completed in October 2007. A total of 139 employees were enrolled in the trial and randomised into the intervention group (n=69) or the control group (n=70). At 6 and 12 months of follow-up, questionnaire data were available for 99 and 89 participants respectively. Objective sickness absence data were available for all participants for 18 months of follow-up. The baseline characteristics of the trial population are listed in table 1. Except for BDI and BSI, baseline characteristics were comparable between the intervention and control group.
Baseline characteristics of the trial population
Effects of the intervention on the primary outcomes sickness absence duration and depressive complaints
Table 2 presents the results of the intention-to-treat analysis for the primary outcome measures sickness absence duration at 12 and 18 months of follow-up and depressive complaints at 6 and 12 months of follow-up. A significant difference in total sickness absence duration was found between the intervention (27.5 days) and control group (50.8 days) at 12 months of follow-up, a reduction of 46% (p=0.017). The intervention group showed a non-significantly lower proportion of long-term sickness absence spells (nine of 69) compared with the control group (17 of 70) (p=0.127) at 12 months of follow-up. At 18 months of follow-up, the total sickness absence duration was 45.0 days in the intervention group and 62.6 days in the control group, a reduction of 28.0%. However, this result failed to reach statistical significance (p=0.150). No significant difference was found in the proportion of long-term sickness absence as well (p=0.175). Regarding depressive complaints, significant differences in change scores were observed for both T1–T0 (p=0.001) and T2–T0 (p=0.005) between the intervention and control group, in favour of the intervention group. Depressive complaints decreased in the intervention group during follow-up and increased in the control group. The intervention group showed a significantly higher proportion of participants with a reliable change in depressive complaints (15 of 43) versus the control group (8 of 51) at 6 (p=0.031) and 12 months (p=0.022) of follow-up (proportion reliable change in the intervention group 13 of 42, in the control group 5 of 45). RRR were 19.2% and 19.8%, NNT were 5.2 (95% CI 2.7 to 55.5) and 5.0 (95% CI 2.7 to 32.1) respectively, for 6 and 12 months of follow-up. The proportion of clinically relevant change in the intervention group was 27 of 44 versus 26 of 53 in the control group at 6 months of follow-up (p=0.225). At 12 months, the clinically relevant change in the intervention group was 28 of 43 and 20 of 45 in the control group (p=0.052).
Outcomes of the intention-to-treat analysis, with objective sickness absence measured at 12 months and 18 months of follow-up and questionnaire data measured at baseline (T0), 6 months (T1) and 12 months (T2) of follow-up.
Effects of the intervention on secondary outcomes
Table 2 also presents the results of the intention-to-treat analysis for the secondary outcomes. Comparable with the results on BDI-II, statistically significant differences in change scores on HAD-D were found in favour of the intervention group, between T1–T0 and T2–T0. Significant differences were found for change scores for T1–T0 and T2–T0 on BSI as well. Again, scores decreased in the intervention group and increased in the control group. No significant differences were found between T1–T0 and T2–T0 between both groups on self-rated health and work characteristics (results not shown).
Per-protocol analysis
Table 3 presents the results of the per-protocol analyses. Sickness absence and depressive complaints were compared between the intervention group, including those employees who received at least one session, and the control group. The intervention group demonstrated a significantly lower sickness absence duration of 52.2% after 12 months (p=0.021) and 47.1% after 18 months (p=0.021) compared with the control group. The latter result of sickness absence duration at 18 months of follow-up differs with the result of the intention-to-treat analysis, in which a non-significant reduction of 28.0% was found. No significant difference was found for the proportion of sickness absence spells >28 days at 12 months (p=0.160) and 18 months (p=0.078) of follow-up. Regarding depressive complaints, similar to the results of the intention-to-treat analysis, statistically significant lower scores on BDI-II were found between T1–T0 (p=0.004) and T2–T0 (p=0.006) in the intervention group. HAD-D also showed significantly lower scores at T2-Screening in the intervention group, and for BSI significant differences were found between both T1–T0 and T2–T0 (results not shown).
Outcomes of the per-protocol analysis, objective sickness absence measured at 12 and 18 months of follow-up and questionnaire data measured at baseline (T0), 6 (T1) and 12 months (T2) of follow-up.
Treatment received and cointerventions
Of the 69 employees allocated to the intervention group, 38 employees completed the intervention and returned their workbooks. The mean number of sessions was 7.5 (SD 2.5). The mean protocol adherence of the psychologists was 95% (SD 12.6). With respect to the use of cointerventions (table 4) only a small number of employees received cointerventions specifically for depressive complaints. No significant and clinically relevant differences were found between the intervention and control group at baseline, 6 and 12 months of follow-up in their use of cointerventions.
Cointerventions used 6 months before completing questionnaires T1 and T2
Discussion
Principal findings and interpretation of outcomes
The aim of this study was to evaluate the effect of a preventive intervention among employees identified at high risk of future long-term sickness absence and with mild to severe depressive complaints in a RCT. The preventive intervention had a substantial effect on sickness absence duration and depressive complaints in favour of the intervention group. During the years in which this study was conducted, sickness absence rates in the company under study were 3.83% (in 2007) and 3.77% (in 2008). Sickness absence rates were 13.93% in the control group and 7.53% in the intervention group over 12 months of follow-up, which indicates that indeed a high-risk group was selected. Although sickness absence was substantially lower in the intervention group than in the control group, the sickness absence rates of the company could not be reached during the follow-up of 18 months. The proportion of long-term sickness absence spells showed no significant difference between the intervention and control group, despite a reduction of 40% as described in the power calculation. This may be explained by the decrease in sickness absence rates in The Netherlands, from approximately 6.0% in 1999, the year in which the power calculation was conducted, to 4.3% in 2009. Results may have failed to reach statistical significance due to the lower prevalence of sickness absence in the population. Sickness absence frequency and time to onset of the first sickness absence spell may have been influenced by the intervention as well, but no significant differences were found between the groups, which may have been because the power was too low.
With regard to depressive complaints (BDI-II), substantial effects were found in the intention-to-treat analysis, again in favour of the intervention group. Scores on BDI-II increased over time in the control group and decreased in the intervention group. Participants in the intervention and control group did not differ in their use of cointerventions. Cointerventions were not likely to have influenced the results, but this could not be completely ruled out. Cointerventions might have reduced the contrast between the groups, and this might have led to an underestimation of the effects found.
Regarding the per-protocol analysis, sickness absence duration was significantly lower in the intervention group at 12 months but also at 18 months. These results indicate that when participants received at least one session, the reduction of sickness absence duration remained approximately 50% until 18 months of follow-up. Regarding depressive complaints, similar results to the intention-to-treat analysis were found. Again, scores on BDI-II increased in the control group and decreased in the intervention group over time. Thus, these results demonstrate that even a small number of sessions seems to be effective. For the per-protocol analysis, a rather conservative approach was used, which also indicates that our results may be an underestimation.
Methodological considerations
Strengths of the study include the randomised design, the availability of a nationwide study population of employees, the objective measurement of sickness absence, the intervention for which a specific protocol was developed, the long follow-up period of 18 months and the monitoring of cointerventions.
Some considerations should be taken into account when interpreting the results of the study. During the pilot study conducted prior to the RCT, a smaller-than-expected overlap between the concepts of risk for future sickness absence and depressive complaints was found. To guarantee sufficient numbers of participants, two adjustments to the original study design were required. First, the screening questionnaire was sent to more employees than originally planned. Second, the cut-off point on the Balansmeter was adapted to a cut-off point with a higher sensitivity to improve the overlap between the concepts. The original cut-off point on the HAD-D was maintained, since this cut-off point has been used in many studies. The smaller-than-expected overlap between both concepts may be explained by differences in the background of the concepts. Risk of sickness absence has a multifactorial aetiology, which does not necessarily include health complaints.
The HAD-D was used to identify employees with mild to severe depressive complaints. To study the course of depressive complaints, the more widely used and more extensive questionnaire BDI-II was used. Our results indicate that many of those employees identified with mild to severe depressive complaints by HAD-D (48.2%) scored in the no to minimal depressive complaints range of the BDI-II at baseline. The mean BDI-II score was 9.77 (SD 3.35) in this category. Regardless of the relatively low score of the employees identified, scores were still in the upper part of the lowest category of BDI-II (range 0–13). So, a reliable and relevant change on BDI-II (>7 points) could still occur.
With regard to blinding, the researcher analysed all data anonymously using personnel numbers. Participants in the RCT were not blinded, since they were aware into which group they were randomised. However, little influence on the results was expected, since no differences in the use of cointerventions were observed. Company counsellors and psychologists were partially blinded, as they were only aware of participants in the intervention group. Therefore, no influence on the contrast between the intervention- and control group was expected. Incomplete blinding may have had some influence on the outcome depressive complaints and the secondary outcomes. However, sickness absence was measured objectively and blinded for the researcher and could therefore not have influenced the results.
Only 38 employees of the 69 employees who were randomised into the intervention group received the intervention according to protocol, implying 44.9% incomplete interventions. A withdrawal rate of 35.3% was found on the questionnaires at 12 months of follow-up. Drop-outs and loss-to-follow-up in the intervention group could have affected the results. However, since objective sickness absence data were available for all 139 randomised employees, there were no consequences for this outcome. For depressive complaints, no selective attrition was found, and no differences in baseline values on BDI-II were found between respondents and non-respondents on T1 and T2. The high number of employees dropping out after consultation with the company counsellor may be explained by the fact that the focus of the RCT was on relatively mild depressive complaints and an increased risk for a future event. Many employees reported not to experience health complaints at the moment of completing the screening questionnaire and therefore may have refused participation.39
Implications and future research
This study focused on prevention of sickness absence and major depression; however prevention will never completely compensate treatment, since there will always be employees who will develop a clinical depression, who have depressive complaints but do not lose their work ability, who will go on sick leave or who do not benefit from preventive intervention. As a result, treatment remains very important.
The focus of our RCT was on employees with relatively mild depressive complaints. Within this mild level, complaints vary in severity. Our results demonstrated that 17 of the 46 employees who started participation in the intervention received fewer than seven sessions of the basic part of the intervention. From a research perspective, it was preferable to indicate a fixed number of sessions the participants should receive in the intervention, to be able to exactly define completion of the intervention. However, in practice this approach was not feasible, since it was unknown how many sessions were required for the mild level of complaints. The per-protocol analysis showed that receiving even a small number of sessions seems already effective. This may indicate that the intervention should be tailored to an employee's individual level of complaints.
The efficacy of the preventive intervention was evaluated among employees in an office work environment. Therefore, this study is not fully representative for the general working population. Nevertheless, it is believed that the intervention may be suitable for similar companies in the occupational healthcare setting, because of the occurrence of comparable kinds of complaints/problems, characterised by stress-related (mental) disorders.
When considering implementation of the preventive strategy into daily practice, employers and policymakers should weigh the effects against the costs of the intervention. Evaluation of the cost-effectiveness was not part of the study. However, based on the intention-to-treat analysis, a decrease of 555 working days of sickness absence between the intervention and control groups was calculated over 18 months of follow-up. The mean labour costs account for €200 per working day. Thus, the profits of reduction of sickness absence amounted to €111 000. Besides benefits in terms of money due to sickness absence, it is known that depression is associated not only with absenteeism but also with presenteeism.40 The positive effect of the intervention on depressive complaints may lead to increased at-work job performance and productivity. In future research, a more extensive cost–benefit analysis should be performed including all facets of the preventive strategy.
In conclusion, the results of this study showed strong preventive effects on both long-term sickness absence and major depression. In the light of the difficult return to work in employees who are already on sick leave, this study clearly demonstrated that a new preventive intervention is a more promising approach in the prevention and reduction of sickness absence and improvement of mental health among employees.
Acknowledgments
The authors thank A Arntz and M Huibers (Maastricht University), T Bouman (University Medical Center Groningen) and A van den Hout (Academic Community Health Centre Maastricht), experts in the field of psychology, for development of the protocol and workbooks for the preventive intervention and training of the participating psychologists. The authors also thank D de Bruyn, S Dijkstra, H Kalter, W ten Haaf and P Batting, company counsellors from Occupational Health Services ‘Beter,’ for performing the consultations. The authors also thank I Pos, director of Cenzo BV, for coordination of execution of the intervention, and J Biemans, S Decoz, J Haasnoot, A Janssen, A Kuipers, G Langenhuizen, M Ooms, G Oppewal, R Verhoog and M Udenhout, psychologists from Cenzo BV, for providing the psychological intervention. The authors thank J Slangen and P Brouns (Maastricht University), B Couwenberg and M Binsbergen (Occupational Health Services ‘Beter’), for their contribution to data management.
References
Footnotes
Funding This study was financially supported by The Netherlands Organisation for Health Research and Development (Zon Mw), grant no 62200024, by CAPHRI School for Public Health and Primary Care, Maastricht, The Netherlands and by the Occupational Health Services ‘Beter’ (ABN AMRO Arbo Services), Amsterdam, The Netherlands.
Competing interests None.
Ethics approval Ethics approval was provided by the Medical and Ethical Committee of Maastricht University (MEC 06-3-018), Maastricht, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.