Article Text

Abstract
Objective To determine whether the prevalence of coal workers' pneumoconiosis (CWP) or progressive massive fibrosis (PMF) among United States underground miners is associated with mine size.
Methods We examined chest radiographs from 1970 to 2009 of working miners who participated in the National Coal Workers Health Surveillance Program for the presence of small and large opacities consistent with pneumoconiosis, based upon the International Labour Organization classification system.
Results A total of 145 512 miners contributed 240 067 radiographs for analysis. From the 1990s to the 2000s, the prevalence of radiographic CWP increased among miners in mines of all sizes, while miners working in mines with fewer than 50 employees had a significantly higher prevalence of CWP compared to miners who worked in mines with 50 or more employees (p<0.0001). When adjusted for age and within-miner correlation, the difference in prevalence of CWP by mine size was significant for all decades. Since 1999, miners from small mines were five times more likely to have radiographic evidence of PMF (1.0% of miners) compared to miners from larger mines (0.2% of miners) with a prevalence ratio of 5.0 and 95% CI 3.3 to 7.5.
Conclusion The prevalence of CWP among United States coal miners is increasing in mines of all sizes, while CWP and PMF are much more prevalent among workers from underground mines with fewer than 50 workers.
- Epidemiology
- health and safety
- coal dust
Statistics from Altmetric.com
Introduction
Since 2000, pneumoconiosis among miners examined in the National Institute for Occupational Safety and Health (NIOSH)-administered Coal Workers' Health Surveillance Program (CWHSP) has increased markedly.1 Additionally, recent findings suggest changes in the epidemiology and clinical features of pneumoconiosis among underground coal miners, characterised by an increase in severity and rapid disease progression.2–5 Excessive inhalation of coal dust is the only recognised cause of coal workers' pneumoconiosis (CWP), although multiple factors are likely responsible for the increased prevalence and severity. Hypothesised explanations include: over-exposure to silica dust, increased production and increasing hours worked.5 An additional risk factor may be employment size of the mine.
Data from the Mine Safety and Health Administration (MSHA) show that fatality rates of US miners are highest among workers in the smallest mines.6 Resources likely influence the mine size/fatality rate association. Smaller mining operations may have limited capital to upgrade safety equipment and dedicated safety and health personnel are less likely to be available to workers in smaller mines.7 Lack of resources may determine the effectiveness of dust monitoring and control, and thus have the potential to influence pneumoconiosis prevalence and severity.
To assess whether CWP prevalence and severity are associated with mine size, we examined chest radiographs from miners who participated in the NIOSH CWHSP for the presence of small and large opacities consistent with pneumoconiosis based upon the International Labour Organization (ILO) classification system.
Methods
Data were derived from the CWHSP and the enhanced CWHSP (ECWHSP). Characteristics of the surveillance program, including data collection and historical perspectives, have been described elsewhere.8–10 In brief, all US underground coal miners are eligible for a chest radiograph prior to working underground, 3 years after the initiation of employment and then every 5 years thereafter. For the CWHSP, radiographs are obtained from NIOSH-approved health facilities. In 2006, NIOSH enhanced this program by collecting radiographs at or near mine sites with a mobile examination unit (ECWHSP). Additional information regarding this program including survey sites is publicly available.11
The radiographs were classified by NIOSH certified readers for the presence, profusion and type of lung parenchymal abnormalities consistent with pneumoconiosis using the ILO Classification of Radiographs of Pneumoconioses.12 A final determination of the classification of each radiograph was made using a standardised procedure, and required agreement between at least two NIOSH certified readers.8 For the present analysis, presence of CWP was defined as an ILO classification of 1/0 or greater for small pneumoconiotic opacities and/or progressive massive fibrosis (PMF). PMF was defined as the presence of any large opacity (category A, B or C).
Data were restricted to radiographs of underground coal miners acquired from 1 January 1970 to 15 May 2009. Complete information for mine location, employment size (ie, number of underground employees) and date of the radiograph was required for inclusion into the analytic dataset.
Approximately one third of miner participants contributed more than one radiograph over the 39-year study period. To account for within-miner correlation, we estimated prevalence ratios (PR) and 95% CIs using generalised estimating equations (GEE) employing a first order auto-regressive correlation structure. We adjusted all prevalence ratios in the GEE models for age at the time of radiograph acquisition.
Results
A total of 145 512 miners were included in the analysis. Study participants were predominantly white (96.3%) and male (97.5%) with an overall mean age of 35.8 years (range 16.1–83.1). Mean and median miner age significantly increased over time with mean age in the 1970s being 33.7 years compared to 41.4 years in the 2000s. Mines with 50 or more employees tended to have a slightly older workforce compared to mines with fewer than 50 miners. From 1970 to 2009 a total of 240 067 radiographs were eligible for analysis. Of the 145 512 miner participants, 86 915 (59.7%) contributed one radiograph, 36 164 (24.9%) two radiographs, 13 915 (9.6%) three radiographs, 5148 (3.5%) four radiographs and the remaining 3370 (2.3%) five or more.
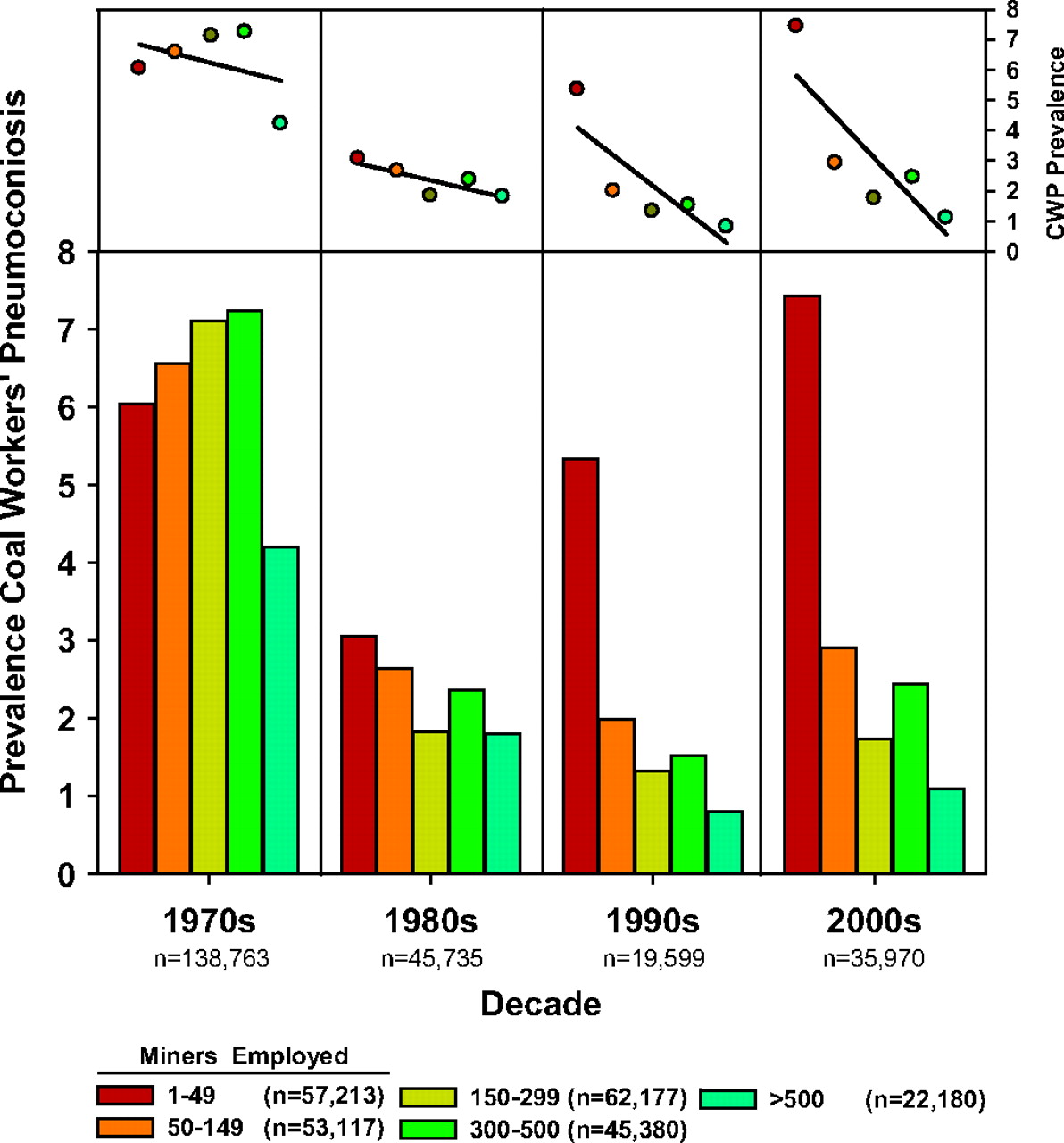
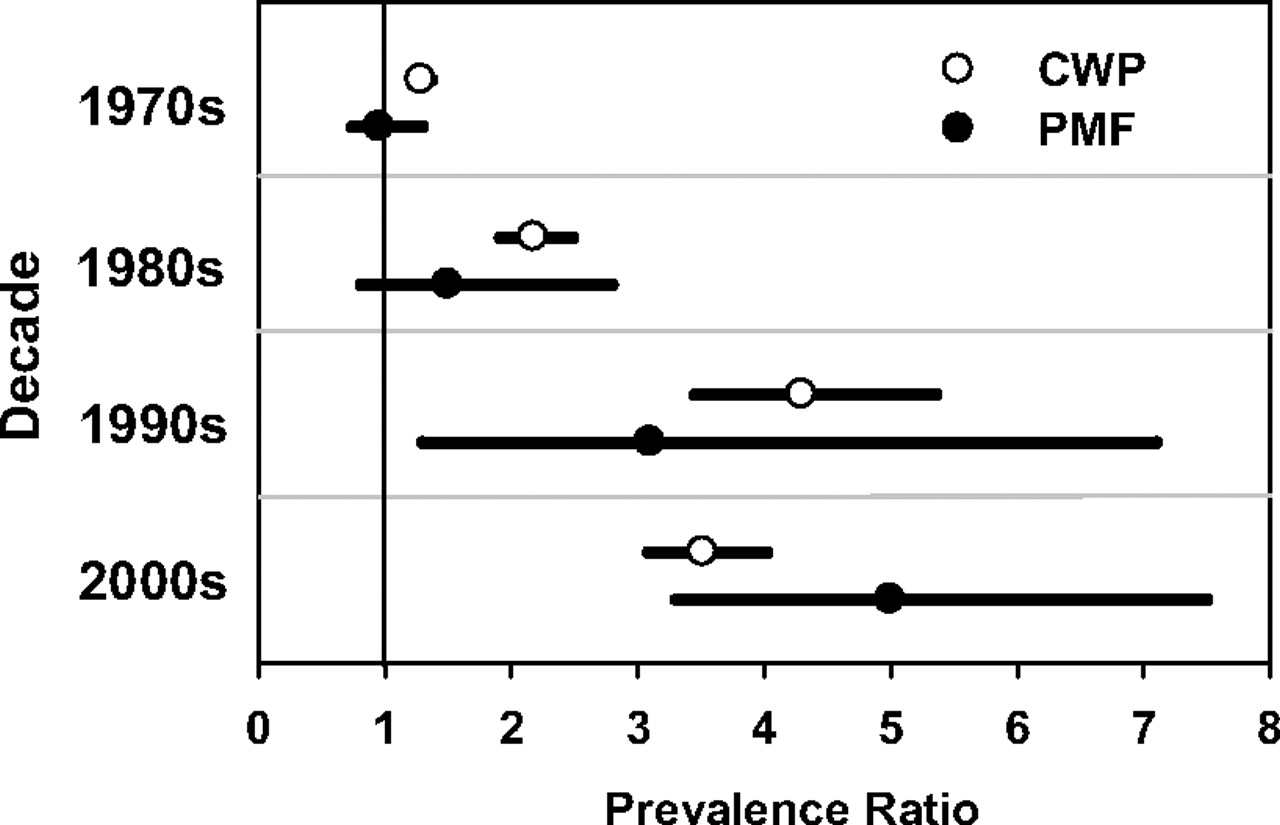
A classification of CWP was present for 11 753 radiographs (4.9%) and 653 radiographs had a final determination of PMF. Prevalence of CWP was 6.5% in the 1970s, 2.5% in the 1980s, 2.1% in the 1990s and 3.2% in the 2000s. Within-decade prevalence of CWP differed by mine size (figure 1). In every decade examined, the prevalence of CWP was lowest among miners who worked in mines with 500 or more employees. Linear regression demonstrated a modest association between mine size and CWP prevalence in the 1970s and 1980s but a significant trend in the 1990s and 2000s (top panel, figure 1). In the 1990s and 2000s, miners from mines with fewer than 50 employees had a higher prevalence of CWP compared to radiographs from miners who worked in mines with 50 or more employees (p<0.0001). When adjusted for age and within-miner correlation, the difference in prevalence of CWP by mine size was significant for all decades (figure 2, white circles).

Coal workers' pneumoconiosis (CWP) prevalence by decade and mine size. Bars represent CWP prevalence among all radiographs. Totals (n) in the key are individual miners. Totals (n) on the x axis represent total number of radiographs by decade. Some miners contributed more than one radiograph. Top panel shows linear regression.

Coal workers' pneumoconiosis (CWP) and progressive massive fibrosis (PMF) prevalence ratios and 95% CIs for mines with fewer than 50 employees compared to mines with 50 or more employees in the United States (prevalence of CWP in small mines/prevalence CWP in larger mines). Generalised estimating equation models were used for calculation of values presented and adjusted for miner age at date of radiograph.
Although a regional analysis at the state level was not possible due to small numbers in some states, an aggregated regional analysis was conducted to assess whether the mine size association with CWP varied by region. The mine size effect was similar across all regions. For example, the adjusted prevalence ratio (aPR) for the states of Kentucky, Maryland, Pennsylvania, West Virginia and Virginia for the 2000s was 2.9 (95% CI 1.7 to 4.7), compared to the overall United States aPR of 3.5 (95% CI 3.1 to 4.0).
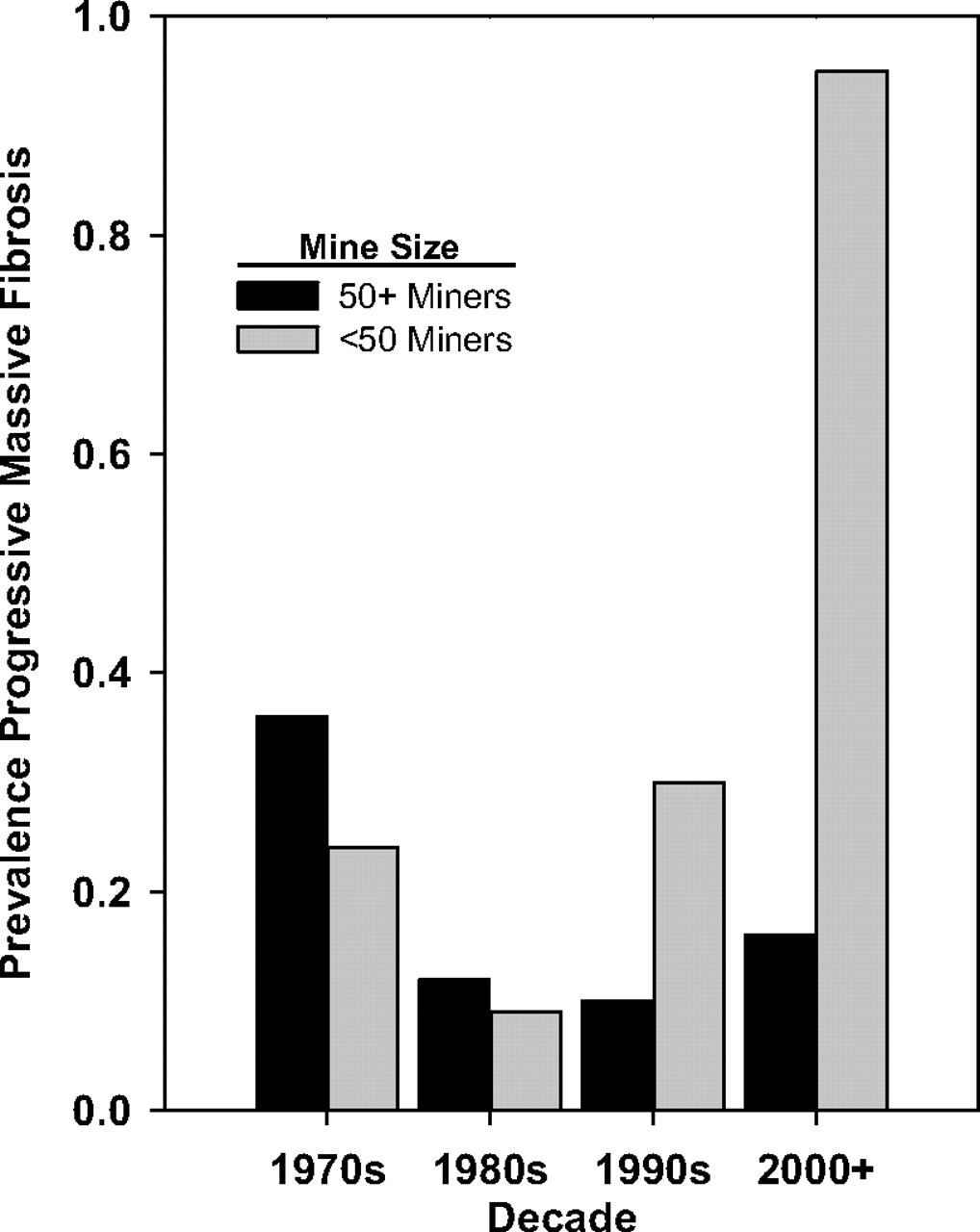
The 653 radiographs with PMF were contributed by 485 miners. The percentage of radiographs with a determination of PMF in the 1970s was 0.33%, 0.11% in the 1980s, 0.14% in the 1990s and 0.31% in the 2000s. In the 1970s and 1980s the prevalence of PMF was higher among miners in larger mines (figure 3). In the 1990s and 2000s PMF was more prevalent among miners working in mines with fewer than 50 workers (p<0.0001). When adjusted for miner age and accounting for within-miner correlation, miners from small mines were five times more likely to have radiographic evidence of PMF compared with miners from larger mines (figure 2, black circles).

{kind=link}
{kind=link}
{kind=link}
Prevalence of radiographs with progressive massive fibrosis in the National Institute for Occupational Safety and Health-administered Coal Workers' Health Surveillance Program by decade and mine size in US underground coal miners.
Discussion
The increase in the occurrence and severity of CWP and PMF in United States coal miners since 2000 has been well documented. However, the factors driving theses increases are not properly understood. We examined whether differences in prevalence existed between large and small mines. Our findings demonstrate increased prevalence and severity in mines of all sizes in the United States. However, CWP and PMF are more prevalent among workers from underground mines with fewer than 50 workers.
Previous reports have demonstrated that non-fatal disabling injuries and fatalities are more common in smaller mines.6 7 13–15 Why smaller mines have higher injury rates has not been thoroughly examined. One study suggested that smaller mines may have a younger, less experienced, workforce compared to larger mines.13 Our data confirm that mines with fewer than 50 employees have a younger workforce. This association was statistically significant for all decades examined; however, the actual mean age difference between small and large mines was relatively modest. In addition, the measure of effect was age-adjusted for the CWP/mine size comparisons. Therefore, we consider this finding to be robust, and discount age as an explanation for the results.
Geographical region is a surrogate for coal rank which is known to be associated with CWP. Had the small mines been concentrated in areas where the coal rank is higher, the findings might have been a reflection of confounding between mine size and coal rank. We were unable to undertake a complete analysis by geographical region (state) because of lack of sufficient data for some states. However, the findings we were able to derive showed the same pattern of findings across states for the CWP/mine size association. Overall, we do not believe that the small mine effect is due to confounding with coal rank or geographical region.
Other possible dust-related factors relate to excessive exposures to silica and mixed-mine dust. It may be that small mines work thinner seams of coal, in which there is greater risk of silica exposure from cutting the mine roof or floor to gain adequate access. In part, this hypothesis is not supported because thin seam mines are primarily concentrated in Kentucky, Virginia and West Virginia; however, the small mine effect was evident in other states.
With respect to mixed-mine dust, the results from a sampling exercise undertaken in the 1990s by MSHA are informative.16 MSHA inspectors made unannounced visits to coal mines and sampled the airborne dust levels at the mine faces. These data were compared with operator-sampled dust levels which showed a decreasing trend in dust levels with decreasing mine size. In contrast, the unannounced operator samples showed an increasing trend in dust levels with decreasing mine size. While for large mines the inspector samples were less or about the same level as the operator samples, the inspector samples in small mines were about twice the level of those from operator samples. The findings of the MSHA study may provide an explanation for our results, as these data suggest that dust levels in small mines may be substantially higher than in larger mines. However, a limitation of this study is that consistent reliable information regarding the cumulative dust exposures for those with CWP and PMF was not available.
To our knowledge, this is the first study to directly examine miner respiratory health and mine size. There are distinct differences between large and small mines which potentially influence the amount and type of exposures experienced in these different environments. Our observation that miners working in smaller underground mines have a greater risk of CWP and PMF is a first step towards targeted prevention efforts. The next step is to systematically identify the factors most likely responsible for the increases in CWP and PMF in small mines through exposure assessments and observation of workforce practices.
Although the focus of this report has been on mine size, it is important to highlight that CWP and PMF prevalence increased between the 1990s and 2000s for mines of all sizes. The ultimate goal must be to return to and surpass the historic reductions in CWP prevalence seen in the 1980s and 1990s, regardless of mine size.
What this paper adds
There has been an increase in the occurrence and severity of coal workers' pneumoconiosis (CWP) and progressive massive fibrosis (PMF) in US coal miners since 2000.
However, the factors driving theses increases are not properly understood.
This is the first study to directly examine underground miner respiratory health and mine size (as measured by the number of employed workers).
CWP and PMF are significantly more prevalent among workers from underground mines with fewer than 50 workers compared to larger mines.
Acknowledgments
The authors would like to thank the Coal Workers' Health Surveillance Program team under the leadership of Anita Wolfe. The authors would like to thank the B-Readers for participation in this study.
Footnotes
Linked articles 53934.
The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the National Institute for Occupational Safety and Health.
Competing interests None.
Ethics approval This study was conducted with the approval of the National Institute for Occupational Safety and Health.
Provenance and peer review Not commissioned; externally peer reviewed.