Article Text

Abstract
Objectives Particulate matter has been associated with acute cardiovascular outcomes, but our understanding of the mechanism is incomplete. We examined the association between particulate matter and cell adhesion molecules. We also investigated the modifying effect of genotype and phenotype variation to gain insight into the relevant biological pathways for this association.
Methods We used mixed regression models to examine the association of PM2.5 (particulate matter ≤2.5 μm in diameter) and black carbon with serum concentrations of soluble intercellular adhesion molecule (sICAM-1) and soluble vascular cell adhesion molecule (sVCAM-1), markers of endothelial function and inflammation, in a longitudinal study of 809 participants in the Normative Ageing Study (1819 total observations). We also examined whether this association was modified by genotype, obesity or diabetes status. Genes selected for analyses were either related to oxidative stress, endothelial function, lipid metabolism or metal processing.
Results Black carbon during the 2 days prior to blood draw was significantly associated with increased sVCAM-1 (4.5% increase per 1 μg/m3, 95% CI 1.1 to 8.0). Neither pollutant was associated with sICAM-1. Larger effects of black carbon on sVCAM were seen in subjects with obesity (p=0.007) and who were GSTM1 null (p=0.02).
Conclusions Black carbon is associated with markers of endothelial function and inflammation. Genes related to oxidative defence may modify this association.
- Air pollution
- epidemiology
- genetic susceptibility
- particulates
Statistics from Altmetric.com
Background
Air pollution has been consistently associated with cardiovascular morbidity and mortality,1–3 but the underlying mechanisms are not well understood. Studies have implicated potential mechanisms of action including oxidative stress, systemic inflammation, autonomic dysfunction and endothelial dysfunction.4 5 Incorporation of biological markers of susceptibility and toxicity into epidemiological studies provides insight into the biology by which particulate matter produces cardiovascular toxicity. Previous studies examining C-reactive protein (CRP), heart rate variability and fibrinogen have suggested that particulate matter-mediated cardiovascular effects may occur through pathways involving the autonomic nervous system and systemic inflammation.6 7
Other blood markers of inflammation being evaluated for their ability to predict cardiovascular disease include the intercellular adhesion molecule-1 (ICAM-1) and the vascular cell adhesion molecule-1 (VCAM-1), which are expressed on cell surfaces and are also found, in soluble form (sICAM-1 and sVCAM-1), in the plasma.8 sICAM-1 and sVCAM-1 are markers of the inter-related processes of inflammation and endothelial function. Monocyte adhesion to activated vascular endothelial cells and their migration into the vessel wall is critical in atherosclerosis. ICAM-1 and VCAM-1 are members of the immunoglobulin gene superfamily and are the most common participants in monocyte attraction induced by different stimuli.9 Few epidemiological studies have examined the association between sICAM-1, sVCAM-1 and particulate matter.10–12 Because inflammation and endothelial dysfunction may be processes by which air pollution affects the cardiovascular system, we wanted to further examine this association. To do so, we looked at the association between sICAM-1, sVCAM-1 and particulate matter in a longitudinal study of elderly men. Multi-day average exposures have been demonstrated to better predict cardiovascular outcomes. We hypothesised that same or multi-day average exposure would be associated with sICAM-1 and sVCAM-1.
We also examined whether this association was modified in susceptible subpopulations, defined by genotype or phenotype. Genotype variation allows us to examine whether certain pathways are important in a particular particulate matter-induced response. Genes selected for analyses were either related to endothelial function or inflammation or were those that have previously been shown to modify the cardiovascular effects of particulate matter. Our choices, and the motivation for those choices, are described below.
Nitric oxide is a key regulatory molecule in the vascular system and common genetic variations of the gene encoding nitric oxide synthase 3 (NOS3, rs1800779 and rs1799983) have been associated with ischaemic heart disease, coronary artery disease and hypertension.13 14 Polymorphisms in the vascular endothelial growth factor (VEGF, rs2010963) gene have been associated with atherosclerosis, possibly through regulation of vascular endothelial growth factor expression.15 Polymorphisms in the lipid metabolic genes apolipoprotein E (ApoE, rs429358 and rs7412) and lipoprotein lipase (LPL, rs328) have both been associated with cardiovascular disease.16 Glutathione S-transferase M1 (GSTM1) and the gene encoding haem-oxygenase-1 (HMOX1) are part of the antioxidant defence system. A microsatellite polymorphism in the promoter region of HMOX1 modifies the response to oxidative stress,17 and has also been associated with cardiovascular risk, including vascular function.18 GSTM1 is part of the GST super-gene family, which produces enzymes which are involved in phase II biotransformation and also exert antioxidative effects. There is evidence that GSTM1 modifies the response of adhesion molecules to environmental tobacco smoke.19 GSTM1 has also been shown to modify the effect of particulate matter on heart rate variability.20 Polymorphisms in the haemochromatosis gene (HFE, rs1800562 and rs1799945) have been shown to modify the effects of particulate matter on heart rate variability.21 HFE is related to metal uptake and partitioning, and metals on particles have been implicated in the inflammatory and autonomic response.22
We examined whether these genes modified the effect of particulate matter on cellular adhesion molecules. We also examined whether phenotypes associated with cardiovascular disease would modify the effect of particulate matter on these molecules. In particular, obesity (defined as BMI ≥30) has been demonstrated to modify the effects of particulate matter on heart rate variability,23 and on markers of inflammation.24 In addition, particulate matter has been associated with an increase in mortality25 and an increase in sICAM-1 and sVCAM-111 in patients with type 2 diabetes. It has also been shown that the association between particulate matter and reduced heart rate variability is stronger in those with diabetes than in those without.7 Therefore, we examined modification by obesity and type 2 diabetes status.
Methods
Study population
The Normative Ageing Study is a longitudinal study established by the Veterans Administration in 1963, which enrolled 2280 men 21–80 years of age from the Greater Boston, Massachusetts area who were free of known chronic medical conditions. Further details have been described previously.7 All participants provided written informed consent. This study was approved by the Institutional Review Boards of all participating institutions.
By 1999, when measurements of sICAM-1 and sVCAM-1 began, 668 original participants had died and a number subjects were no longer being followed, the majority because they had moved out of the region following retirement. Because 97% of this population is white, the analysis was restricted to white men. A total of 811 participants were still coming in for regular examinations on a 3–5-year schedule and were measured for sVCAM-1 and sICAM-1 in at least one visit. Patients who had examinations when no air pollution or meteorology data were available were excluded, leaving 809 subjects (with 1819 observations) available for the present analysis.
sICAM-1/sVCAM-1 measurement
sICAM-1 and sVCAM-1 were measured in the plasma during medical examination visits from 1999 through 2008. sICAM-1 and sVCAM-1 were measured by an ELISA assay (R & D Systems, Minneapolis, Minnesota, USA) with a sensitivity of 0.35 ng/ml for sICAM-1 and 2.0 ng/ml for sVCAM-1.
Genotyping methods
Single nucleotide polymorphisms
High-molecular-weight DNA was extracted from white blood cells with commercially available PureGene Kits (Gentra Systems, Minneapolis, Minnesota, USA). After DNA quantification, samples were adjusted to TE buffer, partitioned into aliquots and stored at −80°C. Genotyping was performed in The Harvard-Partners Center for Genetics and Genomics. We used the TaqMan and Sequenom genotyping platforms. For further details, see online supplementary material.
GSTM1
The GSTM1 locus was amplified at exons 4 and 5 by PCR as previously described23 to differentiate between the null polymorphism and the presence of one or more copies of the gene.
HMOX1
The HMOX1 microsatellite (GT)n length assay was designed according to the method of Yamada and coworkers.26 For further details, see online supplementary material.
Air pollution data
Ambient PM2.5 (particulate matter ≤2.5 μm in diameter) and black carbon were measured hourly at a stationary monitoring site located at the top of a building 1 km from the examination site with a tapered element oscillating microbalance (TEOM; model 1400A, Rupprecht & Pataschnick, Albany, New York, USA) and aethalometer (Magee Scientific, Berkeley, California, USA), respectively. These monitors are operated by the Harvard School of Public Health and measure urban background pollution. Daily averages are calculated when at least three-quarters of the hourly values for a given day are available. We used 24 h, 2- and 3-day moving averages for the pollutants matched on the time of examination for each subject as our exposure indexes. The moving average is the mean exposure for the immediate time period before each examination. Due to occasional equipment problems, air pollution measurements were not available for every 24 h period prior to a patient's medical examination. A total of 5 days were excluded from the analysis for this reason.
Statistical methods
sICAM-1 and sVCAM-1 measurements were log transformed to improve normality in the residuals. The following potential confounders or predictors of sICAM-1 and sVCAM-1 were chosen a priori and included in the analysis: age, apparent temperature, obesity (defined as BMI≥30), cigarette smoking (never/former/current and pack-years smoked), statin use and diabetes mellitus (defined as either physician-diagnosed or fasting blood glucose greater than 126 mg/dl). A cubic spline with 4 degrees of freedom per year of study was used to model the potential relationship between season and time trends with sICAM-1 and sVCAM-1. Covariate information, such as age, BMI, cigarette smoking, medication use and diabetes status, were assessed at each medical examination.
Due to repeated measures of sICAM-1 and sVCAM-1 for many participants, our data may lack independence. Accordingly, we fit a mixed effects model (lme in R 2.9.2 software; The R Foundation of Statistical Computing, http://www.r-project.org). We assumed:
Results
Complete information on the sICAM-1 and sVCAM-1 outcomes and covariates used for the regression was available for 809 participants (table 1). Of these participants, 360 (44.5%) had three visits, 290 (35.8%) had two visits, and 159 (19.7%) had only one visit. Subject characteristics were also examined by genotype and no differences in subject characteristics were observed among these subpopulations.
Characteristics of subjects in the Normative Ageing Study (mean (SD) or n (%))
Table 2 shows the results for the analysis of the association between both PM2.5 and black carbon and changes in sICAM-1 and sVCAM-1 in the entire population. Results are presented as per cent change in mean outcome per 10 μg/m3 (PM2.5) or 1 μg/m3 (black carbon) increase in pollutant. For both sICAM-1 and sVCAM-1 we ran three separate models for each pollutant (in effect, six separate models), estimating the effect of PM2.5 and black carbon for each averaging period ranging from 1 to 3 days before the study visit. There was a significant association between the 2-day black carbon average and an increase in sVCAM-1. Although not statistically significant at the p=0.05 level, 1- and 3-day black carbon averages were also associated with an increase in sVCAM-1. An increase in 1 μg/m3 of black carbon was associated with increases in sVCAM-1 of approximately 5%. PM2.5 was not associated with a change in sVCAM-1. Neither PM2.5 nor black carbon were significantly associated with changes in sICAM-1. For comparison, a 1-year increment of age was associated with an increase in sVCAM-1 levels of approximately 1.7% (95% CI 1.4% to 2.0%) in this cohort.
Main effect of particulate matter on sICAM-1 and sVCAM-1
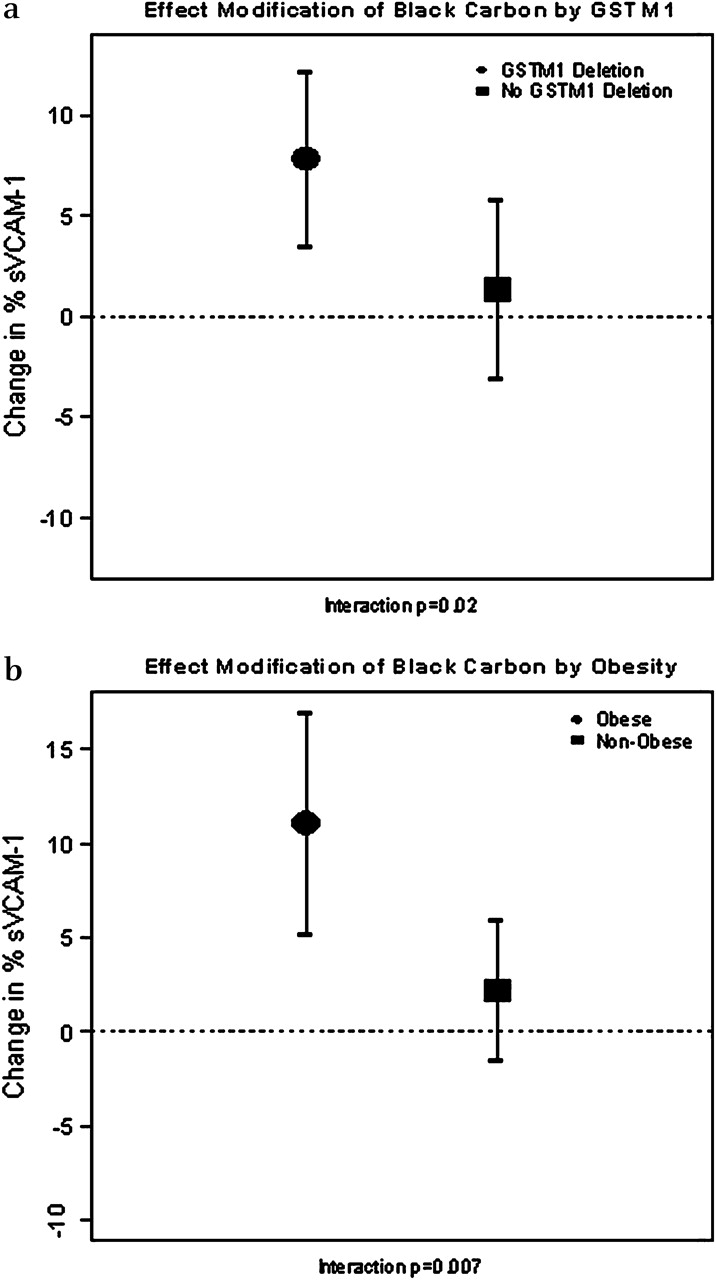
We then examined whether the effect of black carbon exposure on sVCAM-1 was modified by genetic polymorphisms. A complete list of genes, along with the genotype frequencies and the Hardy–Weinberg equilibrium statistics, can be found in table 3. Except for HFE H63D, the distributions of all genotypes in this subcohort were in Hardy–Weinberg equilibrium. However, the overall prevalence for HFE H63D genotypes in the Normative Ageing Study cohort was in Hardy–Weinberg equilibrium (χ2=2.91, p=0.09). We ran regression models including an interaction term between black carbon exposure and having any genetic variant at each of the loci investigated. We found evidence for differential effects of black carbon exposure by GSTM1 status (interaction p=0.02). Figure 1 displays the magnitude of the change in sVCAM-1 in subjects with and without a GSTM1 deletion.
Genotype prevalence and Hardy–Weinberg (H–W) statistics

{kind=link}
Per cent change and 95% CIs in soluble vascular cell adhesion molecule (sVCAM-1) per 1 μg/m3 increase in black carbon. Estimates are from models adjusted for age, obesity, smoking, statin use, diabetes status, apparent temperature and season. GSTM1, glutathione S-transferase M1.
Finally, we examined whether the association between black carbon exposure and cellular adhesion molecules was modified by phenotype. Obesity status significantly modified the effect of black carbon (p=0.007) on changes in sVCAM-1. In obese subjects, black carbon was associated with an increase in sVCAM-1 levels of approximately 11.0% (95% CI 5.4% to 16.9%), as is shown in figure 1. There was no significant interaction between black carbon and diabetes status (p=0.78).
Discussion
We examined the effect of particulate matter exposure in a large cohort and found an association between black carbon and increases in sVCAM-1, which was greater in magnitude than that associated with a 1-year increase in age. We also examined modification by genetic and phenotypic subtypes. We found that variants in a gene related to the oxidative stress pathway modified the association with black carbon. The effect of black carbon was also modified by obesity.
Seaton has proposed that particles may increase pulmonary inflammation, possibly penetrate into the bloodstream, interact with platelets and trigger systemic increases in coagulability and other risk factors for acute myocardial infarctions.27 It has been hypothesised that airway injury or activation of blood cells, such as monocytes, caused by particles deposited in alveoli, leads to a release of proinflammatory cytokines, activating mononuclear as well as endothelial cells and initiating synthesis of proteins such as CRP and upregulation of adhesion molecules.10 Studies have shown particulate air pollution increases levels of these and other markers of inflammatory and endothelial function. Acute increases in ambient particulate matter levels were associated with an elevation in fibrinogen in a large epidemiological study,28 and Peters and coworkers29 reported associations between daily air pollution concentrations and increased plasma viscosity during a period of elevated air pollutant concentrations.
Limited research has provided evidence for an association between air pollution and adhesion molecules. In type 2 diabetes, air pollution was shown to have a positive association with the inflammatory markers, sICAM-1 and sVCAM-1, as well as the von Willebrand factor (vWF), however many of the results lacked statistical significance.11 Although a smaller cross-sectional study, the associations observed between black carbon and sVCAM-1 were statistically significant, consistent with our results.
In a study of 57 elderly male patients with coronary heart disease, a number of inflammatory markers were evaluated for an association with particulates.10 In logistic regression, the odds of sICAM-1 levels above the 90th percentile was increased for an IQR (interquartile range) increase in particulate matter for 1- and 2-day exposure lags. However, when these outcomes were analysed continuously, no significant association was seen. These results are consistent with the hypothesis that individuals in the upper end of the distribution for certain subclinical parameters are the most sensitive.10 30
We found that the association between black carbon and sVCAM-1 was modified by a GSTM1 deletion. In patients with a GSTM1 deletion there was a black carbon-associated increase in sVCAM-1, while in patients without a GSTM1 deletion there was no effect on sVCAM-1 of black carbon, Glutathione pathways are important in cellular defence against reactive oxygen species (ROS). Our findings support the evidence that pathways involving oxidative stress are important mediators of the effects of black carbon on the cardiovascular system.
We found synergistic effect modification between obesity and black carbon for the effect on sVCAM-1. Obesity represents a pro-inflammatory state and as such may increase susceptibility to air pollution by increasing the response to inflammatory stimuli. Obesity was also shown to be associated with an increased response of heart rate variability and other inflammatory markers in this cohort.23
Other investigators have found associations between particulate matter and endothelial function. Schneider et al investigated this relationship through brachial artery ultrasound and pulsewave measurements in a repeated measures study of patients with diabetes. They found that PM2.5 was associated with decrements in endothelial function between 24 h and 3 days prior to the measurement. Similar to our study, greater effects were found among those with the null polymorphism of GSTM1 and those with high BMI.31 O'Neill et al32 studied 270 Greater Boston, Massachusetts, residents. In a subgroup of 182 individuals with type 2 diabetes, they found a decrease in flow mediated dilation associated with exposure to sulfates and black carbon. Similar to this study, the effects for PM2.5 were not statistically significant.
The literature is inconsistent about whether particulate matter is more closely associated with sICAM-1 or sVCAM-1. Our study, like others, showed an association between particulate matter and sVCAM-1, not sICAM-1.11 33 Differences in the molecules may be relevant to interpretation of these results. ICAM-1 is expressed by many cell types, including endothelial cells, fibroblasts, epithelial cells and multiple cells of haematopoietic lineage, while expression of VCAM-1 mostly occurs on atherosclerotic plaques and is limited to activated vascular endothelial and smooth muscle cells.34 35
We also saw an effect of black carbon, but not PM2.5, on sVCAM-1, which is consistent with previous studies and may be due to the differential makeup of the two pollutants.11 PM2.5 is composed of primary and secondary particulate matter, including sulfates and secondary organic aerosols, whereas the greater effect may be due to the primary particulate matter (from traffic-related combustion).
The present study has several limitations including use of a single ambient monitoring site as a surrogate for personal exposure to particles. The potential for exposure misclassification will be greater for spatially heterogeneous pollutants. PM2.5 concentrations in eastern USA are relatively uniform over large areas, including metropolitan Boston.21 Ambient PM2.5 measurements have been shown to be a good surrogate for personal exposures. In a panel study in Boston, where participants were longitudinally followed, ambient PM2.5 concentrations were strongly correlated with corresponding personal PM2.5 exposures.36 Although we would expect some exposure misclassification due to the use of a single ambient monitoring site as a surrogate for personal exposure, we would expect this misclassification to be greater for spatially heterogeneous pollutants (such as black carbon) than for PM2.5. Black carbon concentrations are more spatially heterogeneous because of the numerous local (mobile) sources.21 Even then, the spatial heterogeneity is mostly in level, and not temporal. That is, while black carbon in a higher traffic neighbourhood is higher than in a lower traffic neighbourhood, the same processes (mixing height and wind speed) drive daily variation, and the longitudinal correlation is much better than the cross-sectional one. Nevertheless, we expect greater exposure error for this metric. Classical measurement error tends to bias the effect downward, while Berkson measurement error tends to increase the SE of the estimate. As discussed by Zeger et al,37 when looking at longitudinal air pollution, most error is of the Berkson type. To the extent that it is classical, simulation studies have shown that it is highly unlikely to bias away from the null even in the presence of covariates. Therefore, measurement error in our black carbon exposure metric would likely attenuate the true association. Given that we found significant positive associations for black carbon, it is unlikely that this error would impact our conclusions.
sICAM-1 and sVCAM-1 were measured in the plasma. Whether or not plasma concentrations are accurately capturing the relevant biomarker is unclear. Measurement of plasma concentrations of adhesion molecules are thought to derive from cleavage and shedding from endothelial cells, but factors influencing clearance of these immunological markers remain uncertain. Some have speculated that the shedding process may be different for different CAMs, which could be one factor accounting for differences in measures of association found in epidemiological studies of the two molecules.35 This may be a source of measurement error in the present study.
We can not rule out the possibility of residual confounding. In order to control for possible time-varying confounders which we did not have data on and that may have affected trends in sICAM-1 and sVCAM-1, we used natural splines in our model to control for season and trend. We used four degrees of freedom per year, allowing the seasonal patterns to vary by year. We also included a random intercept for each subject, which should control for unmeasured, time-invariant confounders across subjects.
Very few studies have looked at the association between air pollution and cellular adhesion molecules. By examining the association between such biomarkers and air pollution, this paper adds to the growing body of evidence that elevated levels of particulate air pollution may induce cardiovascular effects through an inter-related process of inflammation and endothelial dysfunction. It also demonstrates that the null polymorphism of GSTM1 and obesity status may modify this effect and suggests that traffic particles, in particular, are important in this association.
What this paper adds
The mechanisms by which particles affect cardiovascular morbidity and mortality are not entirely clear.
Limited, mostly cross-sectional, studies have examined the relationship between particulate matter and cellular adhesion molecules as a potential mechanistic pathway.
This longitudinal study demonstrates that black carbon exposure is associated with an acute increase in soluble vascular cell adhesion molecule (sVCAM-1).
Men who are GSTM1 null or obese are particularly susceptible to this effect of black carbon.
References
Footnotes
Funding This study was funded by the National Institutes of Health, the US Environmental Protection Agency and the US Department of Veterans Affairs.
Competing interests None.
Ethics approval This study was conducted with the approval of the Harvard School of Public Health Institutional Review Board, Boston, MA, the Partners Healthcare Human Research Committee, Boston MA and the Veterans Administration Hospitals Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.