Article Text

Abstract
Objective The French national occupational disease surveillance and prevention network (RNV3P) includes the 30 occupational disease consultation centres in university hospitals to which patients are referred for potentially work-related diseases, and an occupational health service. The aim of this work is to demonstrate the contribution of RNV3P to national health surveillance.
Methods Data from consultations are recorded in standardised occupational health reports and coded using international or national classifications. Programmed health surveillance is carried out through annual follow-up of annual referrals to experts for pre-selected disease–exposure associations, as well as incidence estimations for the well characterised working population followed by the occupational health service. Hypotheses on new emerging diseases are generated using statistical methods employed in pharmacosurveillance and by modelling as an exposome to analyse multiple exposures.
Results 58 777 occupational health reports were collected and analysed from 2001 to 2007. Referrals to the 30 university hospital centres increased significantly for asbestos-related diseases, mood disorders and adjustment disorders related to psychological and organisational demands, and for elbow and shoulder disorders related to manual handling. Referrals significantly decreased for asthma and for rhinitis related to exposure to organic dusts (vegetable or animal) or chemicals, except for cosmetics and cleaning products. Estimation of incidences by the occupational health services showed different patterns in different sectors of activity. The methods for detecting emerging diseases are presented and illustrated using the example of systemic sclerosis, identifying new exposures and new sectors of activity to be investigated.
Conclusion The RNV3P collects data from two complementary samples: 30 university hospital centres (workers or former workers) and an occupational health service (current workers). This dual approach is useful for surveillance and for hypothesis generation on new emerging disease–exposure associations.
- Epidemiology
- statistical models
- occupational diseases
- prevention and control
- registries
Statistics from Altmetric.com
Introduction
Health surveillance is an important issue in occupational health since working conditions and occupational exposures are rapidly changing. It is therefore important that national and international systems should be available which are capable of following changes in known occupational diseases and exposures, and above all capable of detecting emerging disease–exposure associations, in particular those related to new technologies and work organisations.
The European Agency for Safety and Health at Work in Bilbao has recently made an inventory of the various national occupational safety and health monitoring systems in Europe.1 These systems cover in particular health-related events (health monitoring) such as occupational accidents, diseases and absenteeism, and monitor working conditions and professional exposure (risk monitoring).
Health surveillance in France, based on a statutory declaration system, encounters the same problem of under-reporting2 as commonly reported in other countries,3–5 and, above all, is focused on already well known risks. A national surveillance system became necessary, based on the network of occupational disease clinical centres which covers all 30 university hospitals in France and where expert physicians collect standardised reports of work-related diseases independently of compensation considerations. The national occupational disease surveillance and prevention network (Réseau National de Vigilance et Prévention des Pathologies Professionnelles, RNV3P), created in 2001 with the participation of the national health insurance system (Caisse Nationale d'Assurance Maladie, CNAM) and also supported since 2006 by the French Agency for Environmental and Occupational Health Safety (Agence Française de Sécurité Sanitaire de l'Environnement et du travail, AFSSET), every year collects more than 8000 new occupational health reports throughout France, with the exception of the overseas territories.
The aim of the present study is to describe the practical methods the RNV3P uses for health surveillance and to present some of the findings from the 58 777 occupational health reports collected by the network between 2001 and 2007, with regard both to programmed health surveillance and to detection of emerging diseases, on which research is continuing.
Methods
The RNV3P combines three different approaches: follow-up of predefined occupational diseases, estimation of annual incidences concerning the data provided by the occupational health service, and signal generation of potential emerging diseases.
Follow-up of predefined occupational diseases reported by the 30 university hospital centres
The 30 university hospitals throughout the country each have an occupational disease consultation centre to which patients are referred by their general practitioner, occupational physician or other specialist, for investigation of the possible occupational nature of their disease. The principal reasons for referring patients are a need for expert knowledge in characterising the link between exposures and diseases, or a need for technical support (diagnostic tests or strategy). Conversely, if the occupational physician himself/herself can handle the problem, patients are not referred to the university hospital centres, as is the case for most musculoskeletal disorders or cases of hearing loss. Patients are not specifically referred to these centres for compensation procedures as these do not fall within the scope of the centres. The catchment areas mainly cover most big cities and urban areas, and to a lesser extent semi-rural or rural areas (only 1.10% of our patients work in the agricultural sector, including fishing, whereas this population represents 4.16% of the working population according to the 1999 census).
For each patient referred, the experts produce a structured occupational health report whose main coded items are principal disease and comorbid diseases (ICD-10), principal exposure and four other possible exposures (code developed by M Falcy from Institut National de Recherche et Sécurité (INRS) for the CNAM), occupation title (ISCO-88, developed by the ILO) and sector of professional activity (Nomenclature des Activités Françaises, NAF) related to the principal exposure.6 7 For each of the exposures recorded, the expert gives an opinion on how much the principal disease can be attributed to professional exposures: “3” for a direct and essential link, “2” for a possible or direct but not essential link, “1” for a weak or doubtful link, and “0” when the expert thinks the disease is not work-related. The level of attributability is assessed by taking into account the patient's history of occupational exposures, estimated levels of exposures, and the chronology of the appearance of the disease. Demographic characteristics and administrative information on the patient are also recorded. Coding is done by expert physicians in each university hospital centre.
Standardisation of practices and quality improvement are ensured by logistic support provided by AFSSET. Every 18 months, all experts from the university hospital centres undergo quality training to improve coding and procedures are under way for better definition of the levels of attributability. Many automated procedures are performed either during data entry on the computer in each centre (out of range data, test of missing data) or during importation into the national database (data coherence tests according to the typology of the occupational health report, age and employment status). An annual potential error report is generated for each centre and corrections are required to be made. Programmed health surveillance is carried out on the basis of the occupational health reports, from 2002 to 2007 inclusive, which have been classified by the experts as work-related diseases (attributability>0) using conventional statistical methods (χ2 tests) in order to follow, year by year, the changes in predefined groups of disease–principal exposure associations which were selected for their value in terms of prevention and their high number of reports in the network (at least 20 cases annually). This analysis does not include the year 2001, which was the first year that occupational health reports were collected, so that trends could be studied only in data that were known to have been exhaustively recorded by the centres.
Programmed health surveillance based on data from the occupational health service
This standardised data collection has been extended to an occupational health service near Grenoble university hospital since 2004, which serves a population of salaried workers of the urban and suburban population working in Grenoble and in nearby towns. The activity of the salaried workers followed by this occupational health service is presented at the top of table 1. Some activity sectors are not represented, such as agricultural activities, construction and education which all depend on specific occupational health service.
Mean annual incidences of diseases (ICD-10, two-digit level) by sectors of activity in the Grenoble occupational health service, 2004–2007 the letters D,G,H,J,K,L,N,O refer to the first level of the NAF activity sector code.
In this service, eight sentinel occupational physicians record all incident work-related diseases (attributability>0) in the employees whom they follow regularly (10 000–12 000). These employees have a medical interview and are examined by their occupational physician at least once every 2 years. During these clinical visits, the physicians note any newly diagnosed disease thought to be work-related that has developed since the last visit and produce the corresponding occupational record that is then validated by the expert in the centre.
These occupational health reports are coded in the same way as those of the university hospital network and the observations are validated with the expert from the associated university hospital centre.8 Analyses are done separately on this dataset. The incidence of the disease–principal exposure pairs can be estimated, and this was done for the years 2004–2007 through experimental extension of the RNV3P network to the occupational health service mentioned above, as the population followed by the sentinel physicians was known (number, sectors of activity). This approach to surveillance is based essentially on the ICD-10 at the two-digit level, while more detailed codes are used to separately analyse musculoskeletal disorders of the spine, musculoskeletal disorders of the upper limb, carpal tunnel syndrome and other neurological disorders. Annual incidences are calculated as the ratio of the number of new cases of disease discovered by the sentinel physicians to the number of employees that they monitor each year. Incidences are expressed as number of cases/1000 employees per year.
Signal generation of potential emerging occupational diseases
The development of original methods of detecting emerging disease–exposure associations is one of the network's essential axes of research. Two ways are currently being explored: methods issued from pharmacosurveillance and a multi-exposure approach named the exposome.
The first method applies data mining methods of signal generation used by international pharmacosurveillance databases,9 10 including proportional reporting ratios (PRR)11 as employed by the British Medicines Control Agency to analyse the data of the pharmacosurveillance computer system Adverse Drug Reactions On-line Information Tracking (ADROIT). The term “signal” in pharmacovigilance is defined by WHO as “reported information on a possible causal relationship between an adverse event and a drug, of which the relationship is unknown or incompletely documented previously”. In our context, we are interested in reported information on a possible causal relationship between an adverse medical event and an occupational exposure. These safety data mining methods generate a statistical signal when there is a discrepancy between the true number of a disease–nuisance pair reported in the RNV3P database and the expected number for this same pair in the database. Disease–nuisance association giving entitlement to compensation are then excluded, because they refer to an already well characterised occupational risk. This approach has been presented in a preliminary publication,12 where the use of this method was restricted to occupational health reports with attributability at least equal to 1, and taking only the principal exposure into account. In the present study, the same method is applied to 2001–2007 data (one more year), taking into account all exposures recorded, even when attributability is nil, in order to look for previously unknown associations (n=58 777 occupational health reports). The same analysis is also done by sectors of activity and occupations, detecting disease–exposure, disease–occupation and disease–sector activity pairs which generate a “signal”.
The emerging signals are then complemented by the corresponding internal data from the occupational health reports: centres which sent in the reports, level of attributability, associated coexisting exposures, etc. The associations identified in this way are then submitted to national experts for further external investigation, in particular a search for what is known concerning these disease–exposure associations in toxicological and epidemiological publications. The present work takes as an example the results yielded by the PRR method for systemic sclerosis (ICD-10 code M34), a serious disease in which certain occupational factors are established and others suspected.
The second approach uses “exposomes” in a network-based approach that we used to present groups of common exposures shared by patients with multiple exposures and the same disease. The reports are displayed graphically as a network linking occupational situations which share at least one exposure. This approach, familiar to sociologists,13 14 is known in molecular biology as an interactome and describes the network of interactions between proteins or amino acids within a cell.15 Within the RNV3P, methodology using exposomes has previously been described for displaying occupational health reports in the network.16 This was developed with Ucinet 617 and NetDraw software.18 The exposome has many uses in terms of hypothesis generation. First of all, it allows identification of the main exposures shared by patients presenting the same disease, in particular the exposures that are not currently known as risk factors. Secondly, taking the time (on a yearly base) into account, it identifies the appearance of new nodes (new exposures notified for patients presenting the disease), and the speed of growth of all the nodes. If one node is growing faster than another, this is a signal that should be analysed: does it testify better referral to experts and better recognition of a disease–nuisance association, or a diffusion of a new risk factor? An other point of interest of the exposome is the analysis of occupational health reports that are common to different groups of exposure. It may testify that some groups reported with a known risk factor of a disease, may also be exposed to an other under-reported exposure that could also be a risk factor. To illustrate the exposome, we keep the same example consisting of occupational health reports in which systemic sclerosis was the principal disease.
Results
Programmed health surveillance based on patients referred to the university hospital centres
Between 1 January 2001 and 31 December 2007, the network collected 58 777 occupational or environmental health reports concerning potentially work-related diseases. The majority (79%) were potentially related to occupational exposures (attributability>0), 1% were attributed to environmental exposure and in 20% the experts were unable to attribute the disease to either type of exposure (attributability=0). Changes from 2001 to 2007 in the number of occupational health reports, patients' demographic characteristics and type of referring physician are shown in table 2.
Number of occupational health reports, patients' demographic characteristics and type of referring physician in the 30 university hospital centres, 2001–2007
The number of occupational health reports showed a moderate increase over the years. The trend to an increase in patients' mean age, a higher proportion of referring physicians who were not occupational health specialists, and an increase in the proportion of retired patients confirmed that the network continued to be accessible both to a working population and to those no longer in employment.
Table 3 shows the yearly change in the 20 preselected disease–exposure pairs among the 40 819 health reports from 2002 to 2007 with attributability>0.
Annual variation in numbers of preselected disease–exposure pairs in the 30 university hospital centres
The main significant increase in referrals to the expert network concerns adjustment disorders attributed to mental exposures and organisational stress (about 2.3% increase per year), followed by primary lung cancer attributed to asbestos, and musculoskeletal disorders of the shoulder and elbow related to manual handling. Referrals for asthma and rhinitis showed a significant annual decrease in exposure to organic dusts (vegetable or animal) as well as in exposure to chemical products other than cleaning products and cosmetics.
Programmed health surveillance based on data from the occupational health service
From 2004 to 2007, the eight physicians in the occupational health service followed a population of 10 725 to 12 781 employees, depending on the year, and collected 907 occupational health reports. Table 4 shows estimated annual incidences listed in the reports by type of disease (ICD-10).
Annual incidence of diseases (ICD-10, two-digit level) expressed as number of cases per 1000 employees followed in the Grenoble occupational health service
The two disease categories with the highest annual incidence were diseases of the musculoskeletal system (upper limb) and mental and behavioural disorders. The latter increased steadily from 2.5/1000 in 2004 to 6.8/1000 in 2007. Table 1 shows the mean annual estimated incidences (2004–2007) of diseases (ICD-10, two-digit level), analysed by sector of professional activity.
For greater clarity, the columns contain only the sectors in which at least 1500 employees were followed during that period, and the rows give only the groups of disorders with at least 10 incident cases. Patterns of disease incidence differed according to sector of activity. Musculoskeletal disorders of the upper limb were most frequent in the hotel and catering business (p=0.012), mental and behavioural disorders in the transport and communication sector (p<0.001), and musculoskeletal disorders of the spine in health care and social work (p<0.001).
Detection of potentially emerging associations by methods used in pharmacosurveillance: the example of systemic sclerosis
Among the occupational health reports classified as work-related diseases, there were 76 cases of systemic sclerosis. This number rose to 106 when occupational health reports with attributability of nil and systemic sclerosis coded as co-morbidity were also taken into account. All these observations taken together generated 68 different systemic sclerosis×exposure associations, of which seven generated a signal with the PRR method. Associated systemic sclerosis×silica gives entitlement to compensation, whereas the other six associations do not. They are considered as potentially emerging.
Table 5 shows these disease–exposure associations, as well as the disease–sector of activity and disease–occupation pairs which also generate a signal. For each of these associations, the number of cases, the number of hospital university centres which reported these associations, and the years in which the emerging signal was observed are also given.
Systemic sclerosis×exposure, systemic sclerosis×sector of activity and systemic sclerosis×occupation associations generating a signal with the PRR pharmacosurveillance method
As an illustration, the association systemic sclerosis×installation of heating and air conditioning equipment generated a signal because three plumbers/heating engineers working in this activity sector were reported. This signal is interesting because the three cases come from different centres, and has been recently strengthened by new data (>2007, data not shown). It is noteworthy that some exposures, sectors of activity or occupations generated an emerging signal every year, whereas others only generated a signal after the collection of cumulative data over 6 years.
In the second stage of analysis of emergence, these data are compared with those of the literature and a simple classification is proposed according to the level of epidemiological evidence on the one hand and of toxicological evidence on the other. In the present case, among the associations which generate a signal, the relationship with solvents, and with halogen solvents in particular, appears almost constantly in the literature.19 20 Some of the other associations observed have already been mentioned (vibration, welding fumes).21 22 The term pesticide is too vague in itself to attempt to draw a conclusion as regards pesticides, although this risk has recently been suggested in the literature.23 With regard to temperature conditions, it is probable that cold has been a factor leading to diagnosis (triggering Raynaud's phenomenon).
Multiple exposures and the exposome
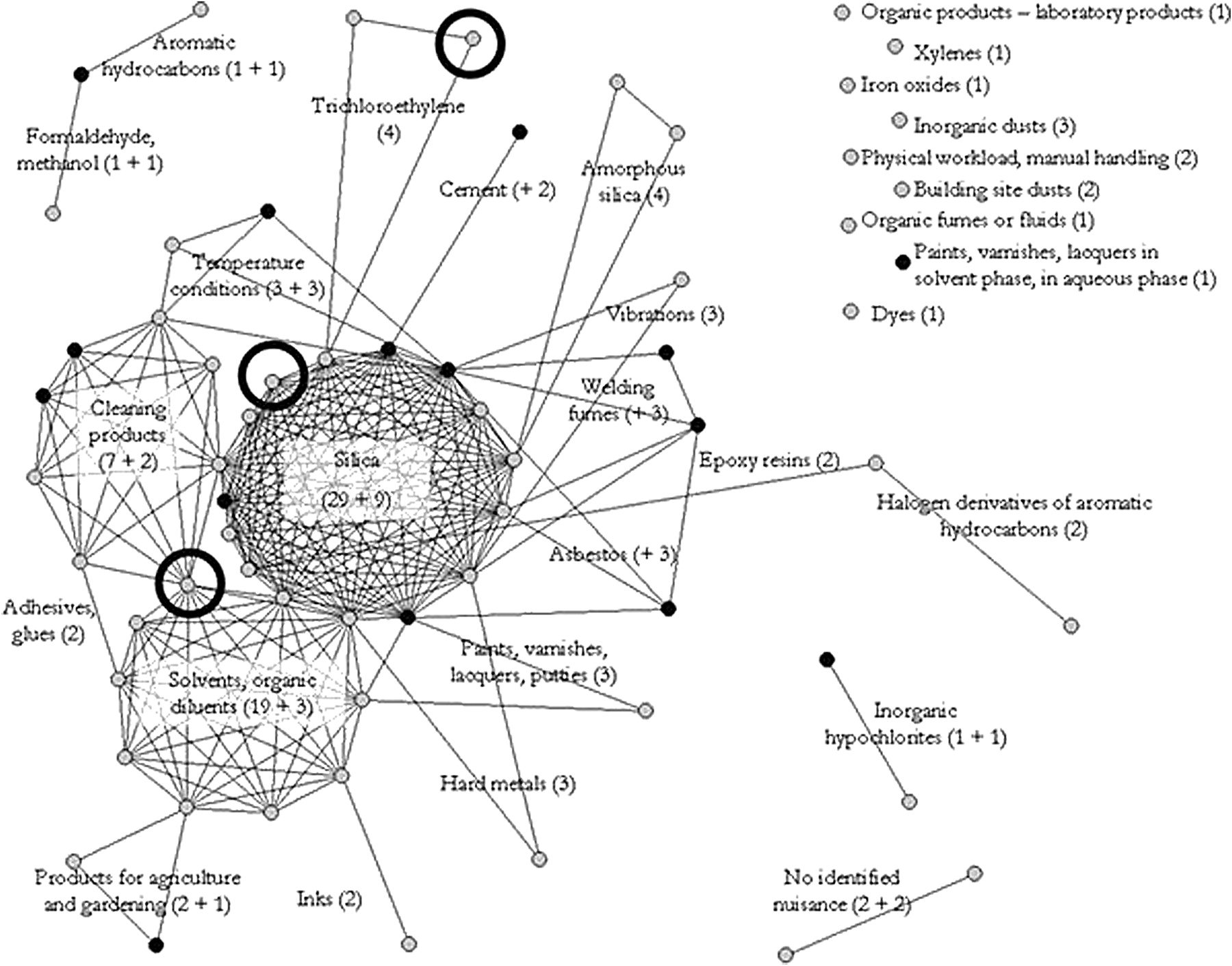
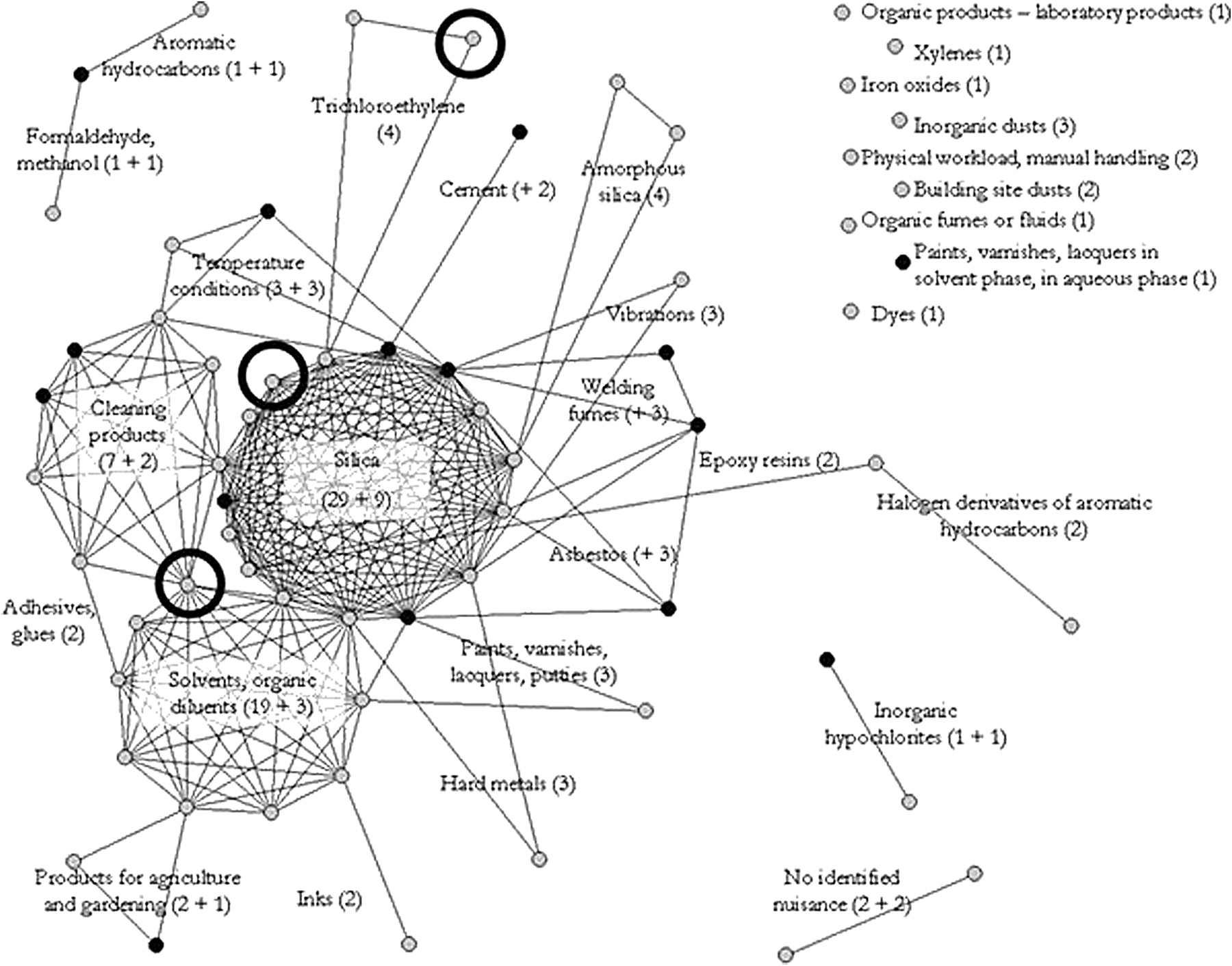
The 106 occupational health reports in which systemic sclerosis was the principal disease or one of the comorbidities are shown in figure 1. Each node is characterised by a weight equal to the total number of copies of identical occupational health problem in the database. Each link illustrates shared exposures between nodes. The nodes that do not share any exposure with the others nodes are considered as isolated and are shown separately to the right of the figure. The diagonal lines represent at least one exposure shared between nodes. The higher the density of the diagonal lines, the more nodes share a common exposure. This revealed three clusters around exposures to silica, solvents and, more precisely, cleaning products. The numbers of observations in each node are shown as the sum of incident cases for 2001–2006, followed by the + sign and by the number of incident cases in 2007 in order illustrate the change produced by the data of the last year analysed. In 2007 there were 27 new observations of systemic sclerosis associated with 15 new exposures (black nodes). Some of these new exposures only occurred once (eg, paints, varnishes and lacquers with aqueous-phase solvents), while others were associated with pre-existing nodes (cement, temperature conditions, epoxy resins, asbestos, formaldehyde and welding fumes). The exposome can also project occupations and sectors of activity: the three cases of systemic sclerosis in the sector of installation of heating and air conditioning equipment are displayed in the exposome as a black circle (see figure 1).
{kind=link}
Exposome of the 106 cases of systemic sclerosis. Data are from the 30 university hospital centres. Grey dots, nodes created by analysis of the data for 2001–2006; black dots, nodes where the number of cases increased with inclusion of the data for 2007; black circles, projection of the sector of activity “installation of heating and air conditioning equipment”. The numbers of observations in each node are shown as the sum of incident cases for 2001–2006, followed by the + sign and by the number of incident cases in 2007.
Discussion
The RNV3P intervenes in health surveillance independently of any statutory considerations related to occupational diseases. The network collects data on all cases where a physician, of any speciality, and throughout metropolitan France, referred a patient to a university hospital centre to establish the relationship between the disease observed and one or several factors to which the patient had been exposed. This approach is particularly interesting for health surveillance and the detection of potentially emerging disease–exposure associations.
We admit that data concerning patients attending the university hospital centres are still of limited classical epidemiological value, as the population to which these patients belong has not been sufficiently characterised to allow the use of conventional epidemiological indicators. For example, if we look at the cases of systemic sclerosis, the mean age (at first consultation) is 51.9 (SD 10.4) years, with no difference between men and women, which is consistent with a French study estimating the prevalence of systemic sclerosis in a large county (n=104, mean age at onset 50.2 (SD 14.7) years), whereas the sex ratio we report is really unusual with nearly twice as many men as women (69 men and 37 women), when all the prevalence studies estimate the sex ratio to be two- to ninefold higher in women24 (92% being female in the above cited French study). This inverse sex ratio confirms that physicians do not notify us of all their patients with a specific disease but just the patients who have specific occupational exposures. Another point is that greater social concern for some diseases, such as adjustment disorders, could explain part of the observed trends (“circularity of argument with referrals”), even if physicians are probably less susceptible to fads than the general population.
Nevertheless, programmed health surveillance by these 30 centres makes it possible to follow the annual referrals to experts for pre-selected disease–exposure associations observed in sufficient numbers. Observation over the years of a significant increase or decrease in referrals to the expert network is a valuable surveillance signal which deserves interpretation: does it indicate less need for expert referrals (progress in diagnostic methods, better knowledge of the disease and its causal factors) or a true impact of preventive measures. Thus, the continuous decrease in referrals for asthma and rhinitis related to exposure to organic dusts and to chemical products, other than cosmetics and cleaning products, is probably meaningful because, during these 6 years of surveillance there has been no substantial change in the characteristics of the 30 centres (number and type of physicians providing consultations, pattern of physicians referring patients). These observations with regard to asthma are in agreement with the statistics of the national health insurance organisation (CNAM) on respiratory allergies,25 26 which also recorded a decrease in allergic asthma and rhinitis compensated during the last four years (2001: n=456; 2002: n=458; 2003: n=474; 2004: n=467; 2005, n=403; 2006: n=379; 2007: n=386) and with data from the THOR network.27 28
Naturally, all such interpretations have to take into account conditions in the centres such as participation in clinical studies, which modifies the recruitment pattern of these centres but is easily characterised (eg, the increase in lung cancers in 2006 and 2007 is mainly due to a clinical research program conducted by five centres). Trends will also be affected by modifications in the occupational consultation supply (eg, if new consultation schedules for adjustment disorders begin, the observed trend could be artificially increased due to greater recruitment). In order to improve the quality of the health surveillance interpretations, research projects designed to better characterise the centre effect and the socioeconomic background in the recruitment area of each centre are currently planned in the network.
Another way to compensate for this epidemiological shortcoming was to extend the methodology to an occupational health service with eight sentinel physicians in the Grenoble area. This venture validated the technical feasibility of estimating annual incidence by sector of activity. Extension of data collection, which has begun with four more occupational health services in France in 2007 (Bordeaux, Clermont-Ferrand, Paris, Rouen), will reinforce these estimations of incidence by considerably increasing the numbers of persons followed and will cover regions with differing occupational activities. It is important to note that the very marked increase in referrals for mental and behavioural disorders is consistent with the rising incidence of these disorders observed in the occupational health services by the sentinel physicians. The expected goal of extension to other occupational health services is to provide national estimations of incidences of occupational health reports according to sectors of activity in order to interpret, with regard to employed persons, the trends in referrals to university hospital centres. In each occupational health service, these statistics are useful for the sentinel physicians so that they can evaluate their professional practices and the direction of their prevention strategies. Ensuring the exhaustive collection of occupational health reports is a recurrent problem with any system of declaration. The funding of one of the sentinel physicians as a coordinator for their colleagues aims to improve exhaustiveness, with 6-monthly coordination meetings with the experts of the associated university hospital centre.
Early, systematic detection of potentially emerging new occupational risks by the RNV3P is based on systematic data mining methods employed in pharmacosurveillance, in order to identify potentially emerging associations which would not have been recognised by the clinicians. To be detected, a potentially emerging disease must have been coded in a relatively uniform way for at least two of the four principle variables of interest (disease, exposures, occupation, sector of activity). The greater the role which can be attributed to an exposure in a disease, the sooner a potentially emerging disease–exposure association will generate a signal.
It is just as interesting to look at the exposures suggested by case reports in the literature but which do not generate signals with the pharmacosurveillance methods used in the RNV3P. Taking the previous example of systemic sclerosis, epoxy resins (code 36410), which have been suggested in the literature as a possible causal agent,29–31 are only reported with systemic sclerosis (M34) twice in the whole database, but they are also reported twice with localised sclerosis (L94) and epoxy paints (code 36217), and once again with another systemic involvement of connective tissue (M35). A more global coding of the disease under the name of connective tissue disorders generates a signal with the PRR method. Moreover, there are numerous observations of systemic sclerosis in which, according to available data, use of epoxy resins was a possibility, and the original dossier would deserve review if the exposures “paints” or “resins” were not precisely coded or in the numerous cases relating to masons (some resin cements for specific uses contain epoxy resins). Similarly, a recent publication32 reported a cluster of systemic sclerosis in typography workers exposed to polyvinyl-acetate glues containing up to 1% of vinyl acetate. In the RNV3P data, two cases of systemic sclerosis were reported with inks, two further cases and two cases of lupus were reported with glues of unspecified type, and a single case of systemic sclerosis was linked with the use of cyanoacrylate glues.
The exposome helps in interpreting emerging data by drawing particular attention, for selected diseases, to the occupational health reports which share the same exposure. The nodes “glues and adhesives”, “epoxy resins” and “inks” are visible before a signal emerges using pharmacosurveillance methods (see figure 1).
Lastly, it is interesting to consider these two methods as complementary and to display on the exposome the sectors of activity or the occupations which generate a signal. The variables exposures, occupation and sector of activity in fact each only give a partial reflection of reality. For instance, three plumbers who installed heating and air conditioning equipment are displayed in different nodes because they were reported with different exposures (see figure 1). However, they may well have shared other exposures in common which the expert did not consider it useful to report or which were not recognised during the consultation (for example, welding fumes, galvanised and stainless steel, refrigerating gases such as chlorofluorocarbons or hydrochlorofluorocarbons, exposures which already appear in other nodes). However, the exposome needs further improvement in order to define thresholds of alerts and to validate its usefulness for the experts. All the emerging signals detected by the automated methods aim to generate hypotheses. It is important to return these signals to the experts with as much documentation as possible, so that after complementary investigations of the literature, they can decide the type of further action required. With logistic support from the AFSSET, network members are now setting up a cell for the management of alerts.
What this paper adds
Association of the occupational and environmental disease consultation centres of French university hospitals with national organisations responsible for disease prevention (health insurance organisations, and national agencies for health and safety) led to the creation in 2001 of the national occupational disease surveillance and prevention network (RNV3P), which collects systematic and standardised records of the patients referred to its consultation centres.
This paper shows how the RNV3P is contributing to occupational health surveillance.
Not only does the RNV3P monitor referrals to experts in occupational diseases at the French national level (follow-up of predefined disease–exposure associations), but it also draws attention to emerging signals with the application of pharmacosurveillance methods and the development of an original network-based approach (taking into account multi-exposure) called the exposome.
These hypotheses (or signals) have to be further investigated by the experts and partners of the network for validation and further action.
References
Footnotes
RNV3P: C Doutrellot-Philippon (Amiens), D Penneau-Fontobonne, Y Roquelaure (Angers), I Tahon (Besançon), P Brochard, C Verdun-Esquer (Bordeaux), JD Dewitte, B Lodde (Brest), M Letourneux (Caen), MF Marquignon (Cherbourg), A Chamoux, L Fontana (Clermont-Ferrand), JC Pairon (Créteil), HJ Smolik (Dijon), J Ameille, A D'Escatha (Garches), A Maitre, E Michel (Grenoble), A Gislard (Le Havre), P Frimat, C Nisse, (Lille), D Dumont (Limoges), A Bergeret, JC Normand (Lyon), MP Le Hucher-Michel (Marseille), C Paris (Nancy), D Dupas, C Geraut (Nantes), D Choudat, L Bensefa (Paris – Cochin), R Garnier (Paris – Fernand Widal), D Leger (Paris Hotel Dieu), E Ben-Brik (Poitiers), F Deschamps (Reims), C Verger, A Caubet (Rennes), JF Caillard, JG Gehanno (Rouen), D Faucon (Saint-Etienne), A Cantineau (Strasbourg), JM Soulat (Toulouse), G Lasfargues (Tours).
RNV3P is indexed in PubMed.
Funding The RNV3P network receives financial support from the Caisse Nationale d'Assurance Maladie (CNAM), the French Agency for Environmental and Occupational Health Safety (AFSSET) and the university hospitals.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.