Article Text

Abstract
Background/objective: Textile manufacturing is a complex industry that has frequently been associated with bladder cancer. However, results have not been consistent. This study investigated the risk of bladder cancer in Spanish textile workers.
Methods: We analysed data from a multicentre hospital-based case-control study carried out in Spain (1998–2001) including 1219 cases of bladder cancer and 1271 controls. Of those, 126 cases and 122 controls reported a history of employment in the textile industry. Lifetime occupational history was obtained using a computer-assisted personal interview. Occupations, locations and materials used in the textile industry were assessed using a detailed questionnaire and expert assessment.
Results: Overall, no increased risk of bladder cancer was found for textile workers, including duration of employment analysis. Increased risks were observed for weavers (OR = 1.82, 95% CI 0.95 to 3.47), for workers in winding/warping/sizing (OR 4.11, 95% CI 1.58 to 10.71) and for those exposed to synthetic materials (OR 1.89, 95% CI 1.00 to 3.56). Working for more than 10 years appeared to be associated with an increased risk for weavers (OR 2.27, 95% CI 0.97 to 5.34), for those who had ever worked in winding/warping/sizing (OR 11.03, 95% CI 1.37, 88.89), for workers in the weaving room (OR 2.94, 95% CI 1.24 to 7.01) and for those exposed to synthetic (OR 2.62, 95% CI 1.14 to 6.01) or cotton (OR 2.00, 95% CI 1.04 to 3.87) materials. Statistically significant higher risks were also found for specific combinations of occupations or locations with exposure to synthetics and cotton.
Conclusions: There was no overall increased risk for textile workers, but increased risks were found for specific groups of workers. Our findings indicate that observed risks in previous studies may be better evaluated by analysis of materials used or section worked within the industry and occupation.
Statistics from Altmetric.com
Bladder cancer is a common malignancy in industrialised countries.1 In Spain, both bladder cancer incidence and mortality are elevated, with this disease ranking as the second cancer site among men.2
Tobacco smoking and occupational exposures are the leading risk factors for bladder cancer.3–5 The textile industry has been traditionally associated with an increased risk of bladder cancer although results have not been consistent.5 It is an old, diverse and complex industry that comprises a wide variety of manufacturing activities, from the preparation and production of textile fibres and yarns from raw materials (cotton, wool, silk, flax, jute, etc) or manmade fibres, the production of woven and knitted fabrics (that is, weaving and knitting) to finishing activities aimed at giving fabrics the visual, physical and aesthetic properties that consumers demand (bleaching, printing, dyeing, impregnating, coating, plasticising, etc) and the transformation of those fabrics into products (garments or clothing industry, carpets, home textiles, technical or industrial textiles, etc). In addition to fibres, workers are exposed to a number of chemical compounds used mainly during finishing, dyeing and printing. Chemical finishing includes bleaching, crease-resistant, flame-retardant, water-repellent, anti-soiling and antimicrobial treatments. Artificial dyes are used and some of them require additional chemical carriers such as aromatic hydrocarbons or halogenated hydrocarbons.6 7 Although the use of chemical compounds is limited during spinning and weaving, yarn lubricants (spinning oils and polymers) and sizing agents are used in these activities. Sizing, a process of preparing the yarn by stiffening the yarns before they are woven, uses starches, polyvinyl alcohols and polyacrylic acids.8 Exposure to asbestos has also been reported in the textile industry.9
The increased risk of bladder cancer that has been observed for textile workers is thought to be explained by exposure to aromatic amine-based dyes in dyers, and fibres and yarns in weavers,10–13 but scientific evidence is not yet conclusive and thus this industry deserves further attention.6 Some studies found increased risks also for spinners, tailors and mechanics,7 10 11 14–22 and there is some evidence that exposure to silk and synthetic materials could be associated with the disease.23 Despite the many studies published on textiles and bladder cancer, analyses have generally been based only on job and industry titles,6 with no detailed information on specific processes and potential exposures.
We report results of a more detailed exposure-oriented analysis on the association between work in the textile industry and bladder cancer among participants in the Spanish Bladder Cancer Study.
METHODS
The Spanish Bladder Cancer Study is a multicentre case-control study of bladder cancer from 1998 to 2001 in Spain. Subjects were identified in 18 hospitals from five areas: Asturias, Alicante, Barcelona, Tenerife and Valles/Bages. Eligible cases were patients aged 20–80 newly diagnosed with primary bladder cancer who lived in the catchment area of the participating hospitals. Diagnostic slides for each case were reviewed by a panel of expert study pathologists to confirm diagnosis and to ensure uniformity of classification criteria, based on the 1998 World Health Organization/International Society of Urological Pathology system.24 The great majority of cases were transitional cell carcinomas (98.7%). Controls were patients hospitalised for conditions considered unrelated to the exposures under study including textile work. For each case we selected one control individually matched to the cases by gender, age group (5-year strata) and residence area. Control patients were admitted to the hospital for the following reasons: 37% hernias, 11% other abdominal surgery, 23% fractures, 7% other orthopaedic problems, 12% hydrocele, 4% circulatory disorders, 2% dermatological disorders, 1% ophthalmological disorders and 3% other diseases. In all, 1219 cases (84% of eligible cases) and 1271 controls (88% of eligible controls) agreed to take part in the study and were interviewed.
Information on known or suspected risk factors for bladder cancer was collected by means of computer-assisted personal interviews during the hospital stay. It included lifetime history of tobacco consumption, lifetime occupational history, water and fluid intake and diet, and exposure to some environmental factors. The study proposal was approved by the ethics committees from all participating centres and all participants provided signed informed consent.
Occupational exposure
We obtained lifetime history of all jobs held for at least six months for each participant at interview. Each job was classified according to the standard industrial25 and occupational26 classifications. Detailed information on occupational exposure was obtained through 63 job-specific or industry-specific comprehensive modular questionnaires. The module for the textile industry included 75 questions and was administered to subjects who, in the occupational history section, had reported having worked in the textile industry. Information was gathered on specific locations, materials, dust and chemicals within this industry, and on frequency and duration of exposure. Respondents were asked whether they had been exposed to yarn, fabric or clothing, as well as the type of fibres or materials used in their job. Seven types of textile fibres were identified: cotton, wool, synthetic, artificial, silk, linen and other. Work in a list of 30 different textile locations was also recorded. For each location in the production area, information on frequency of work in the area (hours/week), duration (year the job began and ended) and perceived level of dustiness was requested. Exposure to a variety of chemical substances in this industry was also included in the questionnaire.
In total, 248 subjects had ever been textile workers and they had held 456 textile jobs. Information for all these jobs was available from the main job questionnaire. More detailed information from the textile module was available for 118 textile workers (47.6%) and for 184 (40.4%) textile jobs. For each of the identified 456 textile jobs, detailed exposure assessment was carried out by a panel of four experts blind as to case-control status: an industrial engineer (AS) who specialised in the textile industry in the province of Barcelona, which includes two of the areas where most textiles workers (80.7%) in the study came from; a Spanish industrial hygienist (SG), an occupational epidemiologist (FGB) and an occupational physician (CS) with experience in the textile industry. The expert panel used both information collected in the lifetime occupational history and the textile module, when available, including the tasks performed during each job, their frequency and duration, possible chemicals and tools that had been used and details on the company’s name, address and the service provided. We used a special software program (ExamCC) that was designed at the National Cancer Institute to more easily review the detailed information collected from the interviews.27 The program was modified to allow exposure assessment data entry for the present analysis. For each job, the occupation, materials used and place of work (location) within the company were coded according to the following classifications. We used nine codes for occupations (fibres preparer, spinner, weaver, finisher/dyer, machine setter, tailor/clothing, supervisor, general or non-classifiable textile worker/apprentice, and non textile worker), seven for materials (cotton, wool, synthetic, silk, rugs, linen, and other), and 33 for locations (maintenance, quality control, utilities, engineering, administration, research, environmental control, receiving/shipping docks, warehouse, carding/garneting/combing/worsted areas, drawing, spinning/twisting/roving, winding, warping, sizing, dressing, weaving, knitting, scouring/blending/mercerising, making the fabric resistant, dyeing/printing, finishing, inspecting, dye room, dope preparation, extrusion, spinning dope into fibre, treatment, cutting/sewing, pressing/ironing, design/patterns making, packaging and recycling). Each textile worker could have had more than one textile occupation, used more than one type of material and had worked in more than one location within the textile industry.
Statistical analysis
Odds ratios (OR) and 95% confidence intervals (95% CI) were calculated using unconditional logistic regression, with the package Stata/SE 8.1. All analyses were adjusted for age (<55, 55–64, 65–69, 70–74, 75+ years), gender, smoking (never/former/current smoker), region and exposure to other high-risk occupations or industries (that is, metal workers, hairdressers and barbers, painters, chemical, leather, transport and rubber industries). Adjustment for socioeconomic status did not modify results. Analysis for more detailed smoking categories including pack-years gave very similar results and are not reported. Risks were examined by duration (⩽10 years and >10 years) and period of employment (before 1960, 1960–74, after 1974), according to relevant changes that occurred in the textile industry of Catalonia.28 Periods of employment were mutually adjusted in subjects who had worked in more than one period.
The non-exposed group was defined as those subjects who reported having worked during their lifetime for at least six months but who had never worked in textiles. We excluded from analyses 37 cases and 50 controls who reported they had never worked in any occupation. In addition, 17 cases and five controls were excluded because the quality of the interview was poor, yielding a total sample of 1182 cases and 1221 controls for this analysis. Of those, 126 subjects were cases and 122 were controls who had worked in the textile industry.
RESULTS
The characteristics of the 248 textile workers are shown in table 1. Cases and controls were comparable in age, gender and educational level. The majority were men, had an age of 65 or more years and had only achieved primary education or less. More cases than controls had ever smoked (p<0.05). A similar proportion (48%) of cases and controls responded at least to one textile module. Compared to the whole study sample (table 1), textile workers had a similar age, educational level and smoking status. However, the proportion of women among textile workers was twice as high as in the whole sample. Most textile workers came from two study areas (Valles/Bages and Barcelona) (80.7%), where more than 20% of controls had ever been textile workers.
Table 2 shows the analysis for main textile occupations, places of work (locations) and materials used. Overall, no increased risk was found for textile workers compared to non-textile workers. Increased risks were found for weavers (odds ratio (OR) = 1.82, 95% confidence interval (CI): 0.95 to 3.47), with loom weavers contributing to most of this risk, and fibre preparers (OR 1.69, 95% CI 0.68 to 4.22). No increased risk was found for dyers and finishers, or for other occupations within the textile industry, including non-production workers. Regarding locations, elevated odds ratios were observed for those who had ever worked in winding (OR 2.70, 95% CI 0.92 to 7.98) and in warping and/or sizing locations (OR 13.40, 95% CI 1.62 to 111.06). Winding, warping and sizing are usually located in the same area. A combined analysis for these three locations showed a high statistically significant elevated risk (OR 4.11, 95% CI 1.58 to 10.71). A non-statistically significant increased risk was found for those working in the weaving room and the dye house. Working in any other locations, including non-production and clothing, was not associated with an increased risk of bladder cancer. With regard to materials, subjects ever exposed to synthetic fibres were found at increased risk of bladder cancer (OR 1.89, 95% CI 1.00 to 3.56), as well as those exposed to cotton materials (OR 1.49, 95% CI 0.92 to 2.40). Little or no increased odds ratios were found for those ever exposed to wool, silk or other materials.
Analysis by duration of exposure (table 3) showed that working for more than 10 years was associated with an increased risk for weavers (OR 2.27, 95% CI 0.97 to 5.34), for those who had ever worked in winding/warping/sizing (OR 11.03, 95% CI 1.37 to 88.89), for workers in the weaving room (OR 2.94, 95% CI 1.24 to 7.01) and for those who had ever been exposed to synthetic (OR 2.62, 95% CI 1.14 to 6.01) and cotton materials (OR 2.00, 95% CI 1.04 to 3.87).
A stratified analysis of main textile occupations and high-risk locations by exposure to cotton, wool and synthetic materials showed an overall tendency for an increased risk among workers exposed to synthetics (table 4). A statistically significant increased risk was observed for weavers (OR 2.24, 95% CI 1.03 to 4.86), mechanics (OR 9.43, 95% CI 1.05 to 84.79) and workers in the winding/warping/sizing section exposed to cotton (OR 5.75, 95% CI 1.55 to 21.31) and synthetic material (OR 15.39, 95% CI 1.89 to 125.29).
No clear pattern was observed regarding period of exposure (data not shown). Increased risks were found for weavers exposed after 1974 (OR 5.85, 95% CI 1.4 to 24.63). Also, increased risks were found for those exposed to winding/warping/sizing before 1960 (OR 7.71, 95% CI 1.32 to 45.24) and after 1974 (10 cases and 0 controls), and for workers in the dye room between 1960 and 1974 (OR 6.94, 95% CI 0.98 to 49.31).
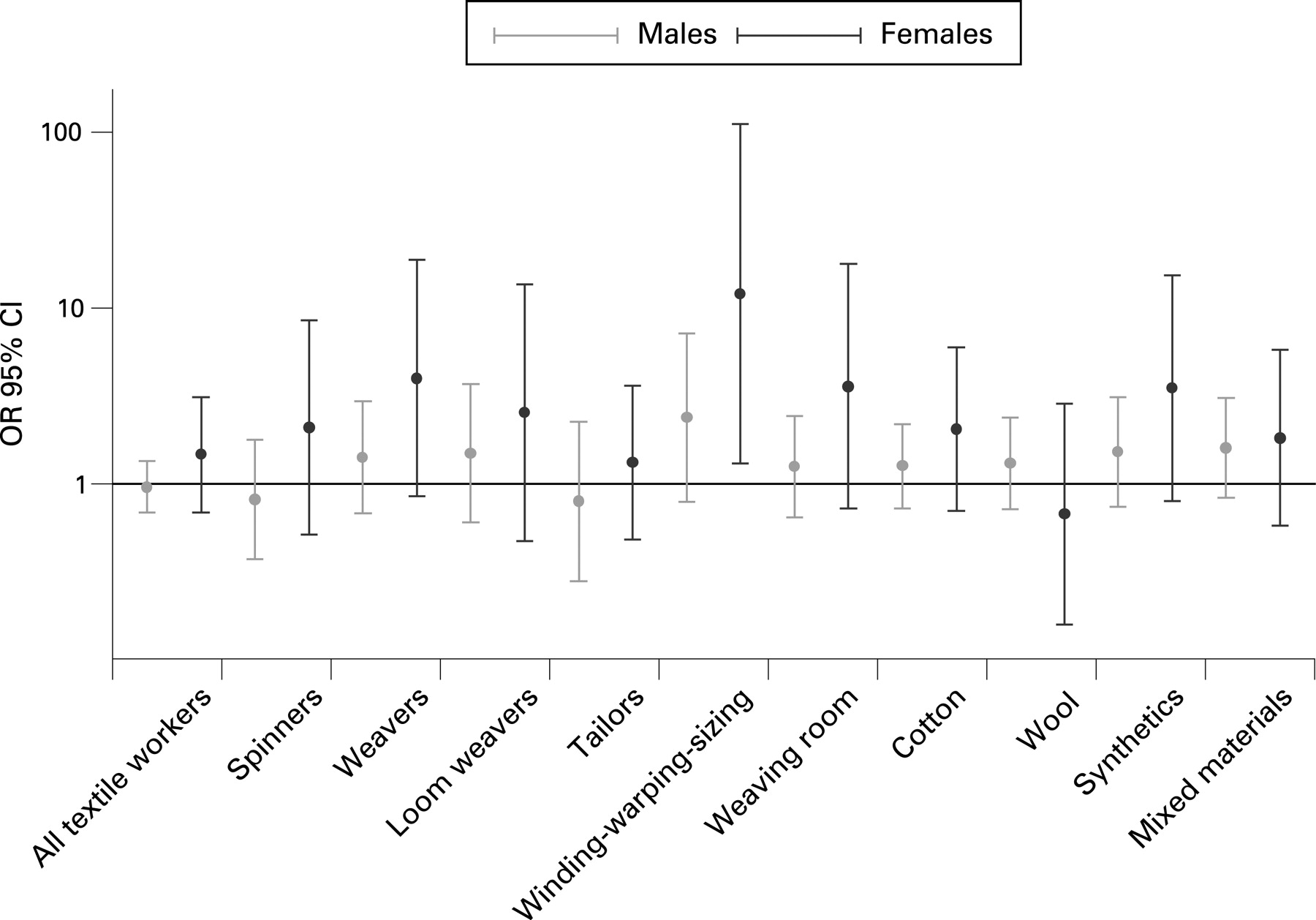
Overall, 20% of textile workers were women. Occupations with a higher proportion of women were tailors (55%), spinners (32%) and weavers (25%). Point estimates were higher for women than men for all major textile occupations with a high number of women textile workers (fig 1). However, none of these gender differences were statistically significant (p values for interaction >0.05). Because of a potential residual confounding as a result of the very different distribution of smoking status by gender,29 when we restricted this analysis to never smokers (611 participants, 82 textile workers), we observed a similar pattern as for all subjects.

{kind=link}
DISCUSSION
We analysed the risk of bladder cancer associated with textile exposures as part of a large case-control study carried out in five areas in Spain. In three of these areas, the textile industry had been prevalent until the 1990s. The main findings from this analysis are that, overall, working in the textile industry did not entail an increased risk of bladder cancer but that working in specific textile occupations (for example, weavers) and locations (winding, warping and sizing, and the weaving room) and with specific materials (synthetics and cotton) was associated with increased risk of bladder cancer, with a duration-response relation.
The increased risk of bladder cancer observed among weavers is consistent with previous studies in Spain and other countries,7 10 12 but we also found for the first time an increased risk of bladder cancer for workers in warping and sizing. Warping and sizing usually share a common physical space, adjacent to the weaving room. Sizing is done before weaving to stiffen the yarn to make it more resistant and prevent breakage during the weaving process. Chemicals used in sizing include starches, used until the 1970s, and polyvinyl alcohols and polyacrylic acids, which were used mostly after the 1970s.8 These agents are not considered to be carcinogens.30 31 There exists some evidence for an association between exposure to polyvinyl alcohols and reproductive outcomes.32 The risk identified in our cohort in winding/warping/sizing coincided with the exposures after the 1970s. Yarn lubricants (spinning oils and polymers) also are used in spinning and weaving.
We observed an increased risk for workers exposed to synthetic materials, after adjusting for potential confounders. These results are consistent with findings from a few studies,16 33 34 but not others.35 Synthetic fibres, such as polyester and nylon, may contain chemical additives including metal salts and oxides (for example, titanium dioxide), phosphorous compounds, cyclic dimers and trimers, caprolactam, cyclic oligomers and antistatic agents (for example, amine derivatives or polyethers). Other synthetic fibres are made from copolymers of acrylonitrile, vinyl chloride and/or vinylidene chloride, and other chemicals, such as organohalogen compounds and antimony oxide, are often added. Manmade fibres based on natural polymers, such as rayon, are made from cellulose or cellulose acetate. During its production, carbon disulfide is added to convert the material to cellulose xanthate. Rayon is usually contaminated by zinc salts and other metallic compounds, and also with polyvinylpyridine and polyvinylpyrolidine (to increase its basic dyeing capability) or polyacrylic acid (to increase its absorbance). We asked about specific types of synthetics but for most, the numbers were not large enough. An increased risk was also found for those exposed to cotton materials, especially for weavers. Cotton may have toxic chemical residues such as chemical defoliants, applied after the cotton balls have matured and opened, including arsenic, which has been reported to be present in cotton fibres.36 37 The lack of available scientific evidence on the association of specific fibres and bladder cancer does not allow us to draw any conclusions. We also observed an excess risk among mechanics, which could be due to exposure to chemicals incidental to the production process, such as machinery cleaning chemicals.
Because a relatively high proportion of women are employed in textiles compared to other industries, we explored whether there were any differences in the risk of bladder cancer between men and women who worked in the textile industry. Despite a lack of statistical significance, we observed a consistent trend of higher risk point estimates among women than men for those occupations and in locations employing a higher proportion of women. Possible reasons that may explain differences in occupational risks between genders are differences in jobs and tasks within jobs, in metabolism and genetics, in the use of preventive measures and in occupational and non-occupational modifying factors.38 Differences in exposure are the most likely explanation for the observed pattern of higher risk among women. However, retrospective data on exposure levels were not available and such differences could not be documented. Smoking prevalence was much higher in men than in women in our study, but differences remained even after excluding smokers from the analysis. Findings from our study and other studies do not indicate major gender differences regarding the two main polymorphisms associated with bladder cancer, specifically NAT2 and GSTM1.39 In addition, metabolism of some of the potential exposures associated with an increased risk in our study is unlikely to be modulated by these two genes.
The textile industry is an old and diverse industry and is one of the largest employers worldwide, with more than 13 million workers, mainly in developing countries.6 37 The association between exposure to artificial dyes in the chemical industry and bladder cancer has been well known for decades.40 Several, but not all, studies have also found an increased risk for dyers in the textile industry.7 11 13 In our study, no increased risks were found for dyers/finishers, except a borderline increased risk for workers in the dye room between 1960 and 1974, a period where aromatic amine dyes could still have been used in Spain. This lack of a strong finding is not surprising since preventive measures were extensively applied in past decades throughout Europe to prevent exposure to dyes as these were singled out as one of the main causes of bladder cancer in several industries.20 Our results indicate that an increased risk of bladder cancer persists in this industry, which cannot be attributed only to exposure to dyes. These results are important especially in developing countries where textile industries are flourishing and exposures can be expected to be higher than those observed in industrialised countries.41
A small sample size in stratified analyses is the main limitation of the study. Some of the study areas were traditional textile industry areas and, as a consequence, the total number of textile workers was higher in this study compared to most previous studies. However, owing to the considerable length of the interview, only 48% of textile workers completed a textile module, although all completed the lifetime occupational history. As a consequence, for more detailed analyses, such as locations and materials, information was often lacking for those without a textile module. Responders to the module were similar to non-responders with respect to age, gender, region, background education, and smoking status and any bias from this non-response is unlikely. Detailed information is a major strength of this analysis, at least for those workers completing the module. The use of a specific module to assess occupational textile exposures allowed us to collect more detailed information on specific places of work and materials than previous studies. Furthermore, assessment by experts with an extensive knowledge of the textile industry in the study areas was a key element that is likely to have improved exposure assessment.
In conclusion, this is the most detailed analysis to date of risk of bladder cancer within the textile industry. It used, for the case-control design, a state-of-the-art exposure assessment procedure and illustrates the importance of collecting detailed information on industries and jobs when conducting research in a specific occupational setting. This analysis suggests that workers in the weaving process and those exposed to synthetic and cotton materials may be at increased risk of bladder cancer. In particular, we observed for the first time an association between weaving preparation activities (sizing, warping and winding) and bladder cancer that warrants further research. Our findings indicate that observed risks in previous studies may be better evaluated by a combination of materials used, section worked within the industry and occupation.
Main messages
-
Workers in the weaving process and those exposed to synthetic and cotton materials were at increased risk of bladder cancer.
-
We observed for the first time an increased risk among workers in weaving preparation activities including sizing, warping and winding.
-
A state-of-the-art exposure assessment for this type of study shows that cancer risk in the textile industry may be determined by a combination of materials used, location worked within the industry and occupation.
Policy implications
There is a need for case-control studies on bladder cancer to assess the exposure to specific sectors and materials within textiles manufacturing in areas with a high prevalence of this industry.
Acknowledgments
We thank Robert C Saal from Westat, Rockville, MD, USA; and Leslie Carroll, Jeremy Bendler and Eric Boyd from IMS, SilverSpring, MD, USA, for technical assistance, and Dr Francisco X Real, one of the principal investigators of the Spanish Bladder Cancer Study, for commenting on an earlier draft.
Appendix
Participating study centres in Spain
Institut Municipal d’Investigació Mèdica, Barcelona–Coordinating Centre (M Sala, M Torà, D Puente, C Villanueva, C Murta-Nascimento, J Fortuny, E López, S Hernández, R Jaramillo); Hospital del Mar, Universitat Autònoma de Barcelona, Barcelona (J Lloreta, S Serrano, L Ferrer, A Gelabert, J Carles, O Bielsa, K Villadiego), Hospital Germans Trias i Pujol, Badalona, Barcelona (L Cecchini, JM Saladié, L Ibarz); Hospital de Sant Boi, Sant Boi de Llobregat, Barcelona (M Céspedes); Consorci Hospitalari Parc Taulí, Sabadell (D García, J Pujadas, R Hernando, A Cabezuelo, C Abad, A Prera, J Prat); Centre Hospitalari i Cardiològic, Manresa, Barcelona (M Domènech, J Badal, J Malet); Hospital Universitario de Canarias, La Laguna, Tenerife (J Rodríguez de Vera, AI Martín); Hospital Universitario Nuestra Señora de la Candelaria, Tenerife (FJ Taño, F Cáceres); Hospital General Universitario de Elche, Universidad Miguel Hernández, Elche, Alicante (F García-López, M Ull, A Teruel, E Andrada, A Bustos, A Castillejo, JL Soto); Universidad de Oviedo, Oviedo, Asturias; Hospital San Agustín, Avilés, Asturias (JL Guate, JM Lanzas, J Velasco); Hospital Central Covadonga, Oviedo, Asturias (JM Fernández, JJ Rodríguez, A Herrero), Hospital Central General, Oviedo, Asturias (R Abascal, C Manzano, T Miralles); Hospital de Cabueñes, Gijón, Asturias (M Rivas, M Arguelles); Hospital de Jove, Gijón, Asturias (M Díaz, J Sánchez, O González); Hospital de Cruz Roja, Gijón, Asturias (A Mateos, V Frade); Hospital Alvarez-Buylla (Mieres, Asturias): P Muntañola, C Pravia; Hospital Jarrio, Coaña, Asturias (AM Huescar, F Huergo); Hospital Carmen y Severo Ochoa, Cangas, Asturias (J Mosquera).
REFERENCES
Footnotes
-
Funding: This work was partially supported by the Intramural Research Program of the Division of Cancer Epidemiology and Genetics, National Cancer Institute, USA, and by the Fondo de Investigación Sanitaria, Spain (grants 96/1998–01, 00/0745, G03/174, G03/160, C03/09, and C03/10).
-
Competing interests: None.