Article Text

Abstract
Objectives: Major depression is a leading cause of psychiatric morbidity and may be influenced by psychosocial factors in the workplace, although evidence so far remains circumstantial. This paper reviews follow-up studies addressing the risk of major depression and depressive symptoms relative to psychosocial stressors in the working environment and evaluates the evidence for causality.
Method: Follow-up studies were identified by a systematic Medline search combining search terms for the outcome and measures of job-related psychosocial factors. The quality of the studies was evaluated using 22 criteria related to their potential for bias and confounding.
Results: Sixteen company or population-based studies including some 63 000 employees were identified. Validated multi-item scales were used to measure perceived psychosocial stressors in most of the studies. Major depression was defined by clinical criteria in seven studies and by symptom scales in another seven. The follow-up period ranged from 1 to 13 years. The prevalence of depressive disorder varied substantially, suggesting a high degree of study heterogeneity. The adjusted relative risk for onset of a major depressive episode according to job stressors ranged from 0.5 to 1.5 in 44 of 61 reported associations with various psychosocial factor dimensions. Associations were strongest and most consistent for job strain defined as high demand and low decision latitude among men. Most studies shared common limitations such as lack of independent measures of exposure and outcome and potential confounding. Although a meta-analysis would technically be possible, heterogeneity across studies evidenced by variation in the prevalence of depression made this unfeasible.
Conclusion: This review provides consistent findings that perception of adverse psychosocial factors in the workplace is related to an elevated risk of subsequent depressive symptoms or major depressive episode; however, methodological limitations preclude causal inference. Studies implementing objective measures of job stressors or independent outcome ascertainment are warranted.
Statistics from Altmetric.com
Major depression is a recurrent mental disease characterised by episodes of reduced mood and interest that persist for at least 14 days.1 The reported prevalence of major depression varies between and within countries; however, data are strongly influenced by the diagnostic tools that are applied.2 In a random sample of US workers, 6.4% met the criteria of a major depressive episode during a 12-month period according to the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI).3 The use of the Major Depression Inventory (MDI), a validated self-rating scale which assesses depressive episode according to the symptomatic criteria in the DSM-IV and the ICD-10, revealed a 3.3% point prevalence of major depression in a random sample of Danish citizens.4 Major depression is more prevalent in women than in men. The peak age of a first-onset major depressive episode is between 25 and 45 years of age.3 Some 75% of patients recover within a year, but about 60% experience a new major depressive episode later in life.5
According to a 1997 literature review, it has been consistently documented that exposure to stressful life events is associated with subsequent onset of depressive episodes and that the risk increases with the severity and contextual importance of the event.6 Moreover, life events seem more important forerunners of first than subsequent depressive episodes.7 The evidence that serious life events greatly increase the risk of major depression is strong, however methodological limitations should not be ignored.6
Assuming that severe life events can, indeed, elicit a major depressive episode, it seems likely that chronic difficulties may also be of importance through similarly mechanistic pathways.6 8 Psychosocial stressors related to the work environment are of particular interest because they may be more easily prevented than the strain that results from life events, which are often unavoidable. Moreover, long-term stressors lasting several months or years may cause more severe disease and contribute to a greater relapse or recurrence rate.9
In reviewing the scientific literature, several authors have consistently found evidence that psychosocial factors in the workplace may play a role in well-being and psychological distress.9–12 However, the impact of psychosocial workplace factors on clinically significant psychiatric disorders has not been reviewed. This is regrettable because such disorders have a major impact on long-term disability, dependency, sick leave, lost productivity and mortality.13 During the past few years, several follow-up studies have addressed the risk of onset of major depressive disorders, which now involves critical assessment of work-related risks. The objective of this review is to identify follow-up studies that explicitly address the risk of major depression or depressive symptoms relative to psychosocial factors in the working environment and to discuss the evidence of causal association.
LITERATURE SEARCH METHODS
A systematic search for scientific literature for this review was undertaken in Medline (start date: 1966) on 28 August 2007. The criterion for inclusion was original research estimating the risk of major depressive disorder or depressive symptoms according to indicators of adverse psychosocial factors at work. Less specific outcomes such as well-being, mental health, anxiety, burnout, psychological distress or perception of general health were not included. Criteria for measures of job-related psychosocial factors were not rigorous and included validated scales of perceived strain such as job demand-control-social support scales and the effort–reward imbalance scale. Other models were also used, for example single-item measures and lists of work events. However, job titles or occupations with no particular exposure assessment were not included. Only follow-up studies were considered useful for the purposes of this review and a large number of cross-sectional studies were not included. Strict criteria with respect to a number of specific design features were not requested.
Two searches were carried out, one based upon medical subject headings (MeSH terms) and the other on free text strings. Lists of terms relating to mental disorders and to psychosocial factors were compiled using titles and key words from a number of recent core papers in the field. The complete search strings are given in appendix A. The searches were subsequently combined using the Boolean operator “AND” and were restricted to English journal articles with abstracts. The MeSH search identified 749 papers, the free text search 3042 papers and the combined yield was 3507 papers. Screening of titles reduced the number of eligible papers to 158, which was further reduced to 55 by abstract reading. The final sample of 13 papers fulfilling the eligibility criteria was identified by full paper reading.14–26 Bibliographies of the most recent reviews and original studies identified another three papers that had not been retrieved by the systematic literature search.27–29 Only one paper presenting findings from an individual cohort was included in the review. For example, findings from the French GAZEL study are based upon the paper by Niedhammer et al,18 while several other reports based upon the same data were not included.30–32
Included papers were characterised with respect to a number of design features considered relevant for judging the appropriateness of the evidence presented relative to the objectives of this review. In total, 22 features of design and methods were checked systematically to decide whether a characteristic was present or not (table 1).
For descriptive purposes, odds ratios and confidence intervals were averaged across studies for identical predictors (job demands, decision latitude and social support) by use of a comprehensive meta-analysis programme.33 The more conservative random effects models are reported.
RESULTS
Descriptive characteristics of the 16 eligible follow-up studies included in the review are listed in tables 1 and 2 and risk estimates by type of psychosocial factor are given in figs 1–4.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
All studies except three have been published within the past 5 years (table 2). Most involved employees in large companies or public service institutions such as hospitals, although several studies were population based (table 2). In addition to a nation-wide registry study covering more than 150 000 people,25 the other studies included a total of 62 606 employees and the average sample size was approximately 3400 participants. Follow-up from baseline recordings to outcome measurements ranged from 1 to 13 years; attrition during follow-up was limited and did not exceed 20% except in four studies (table 1). The applied measures of psychosocial job characteristics were heterogeneous: nine used the Job Contents Questionnaire albeit in different versions, two implemented the effort–reward imbalance model, two focused on organisational injustice and the remaining studies used other single or multi-item scales (tables 1 and 2). Independent measures of exposures were not obtained except in one study which used supervisor reports23 and a job exposure matrix that averaged perceived stressors across employees in specific jobs.25
Clinical psychiatric criteria (DSM-III, DSM-IV or ICD-8) were used to define major depression in seven studies (tables 1 and 2). This includes one study based upon clinical cases of depressive disorders diagnosed in the health care system25 but not a study that relied upon doctor-diagnosed depression as reported by the employee28 or a study that used prescription of antidepressant medication as the outcome.24 In the remaining seven studies, the outcome was depressive symptoms measured by questionnaire or interview depression scales (tables 1 and 2). The tools used to collect the information and the algorithms employed to arrive at the diagnosis varied, which may be an important reason for the wide variation in the baseline prevalence of depression across studies (table 2).
All but four studies excluded persons fulfilling the outcome criteria at baseline, but only a few restricted the analyses to first-onset cases. Most studies adjusted risk estimates for the effects of gender, age, educational level, income, employment status and marital status, some adjusted for personality, domestic stressors and life events, and few took account of other known or likely risk factors for depression such as history of affective disorder in the family, earlier mental disorder and serious chronic disease. All studies used multivariate techniques to adjust for possible confounders, but none adjusted for variables from all six following domains: demography, life events or domestic strain, personality, earlier mental disorder, chronic disease and family history of depressive disorder (tables 1 and 2). Apart from five studies, none provided exposure–response or exposure–effect data and the risk according to the time lag between the stressor and the onset of depressive disorders was not detailed in any of the studies.
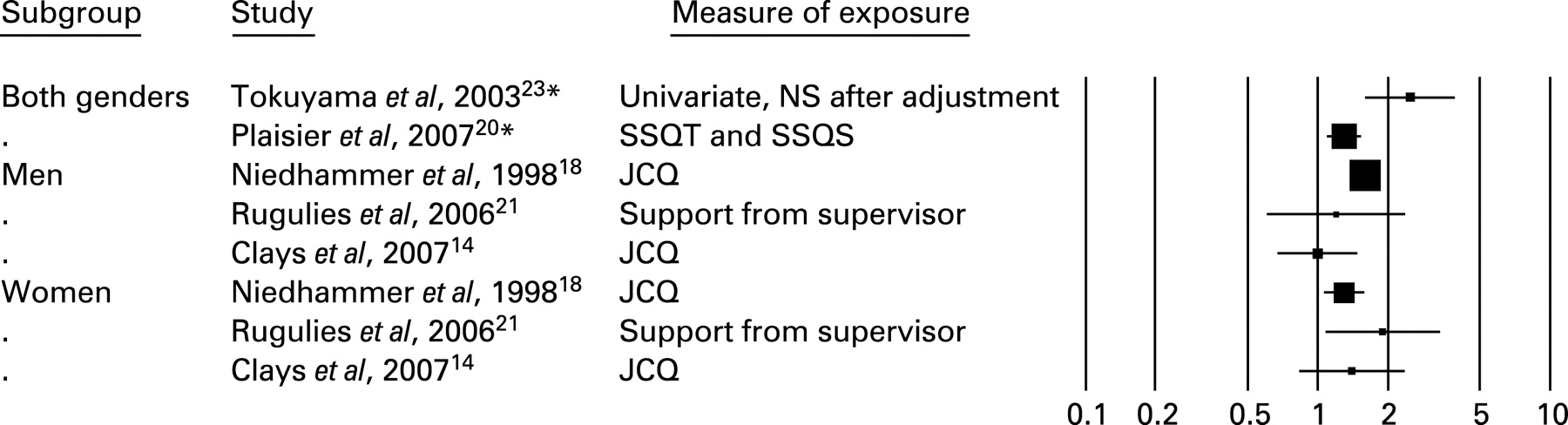
The relative risk of depressive disorder according to the separate dimensions of the job demand-control-social support model is displayed in figure 1, which includes seven studies based upon the widely used Job Contents Questionnaire (JCQ) and three studies using other items and scales to measure similar concepts. Most risk estimates showed elevated risk for employees holding perceived high-demand jobs with no noticeable differences between men and women. Very similar results were found for decision latitude and social support (figs 2 and 3). The average risk across all studies weighted by the number of participants was 1.31 (95% CI 1.08 to 1.59) for demands, 1.20 (95% CI 1.08 to 1.39) for control and 1.44 (95% CI 1.24 to 1.68) for social support. These figures only changed marginally in a sensitivity analysis that included the six studies where the Job Contents Questionnaire was employed. Furthermore, the risk was not dependent on outcome criteria (clinical versus symptom scales).
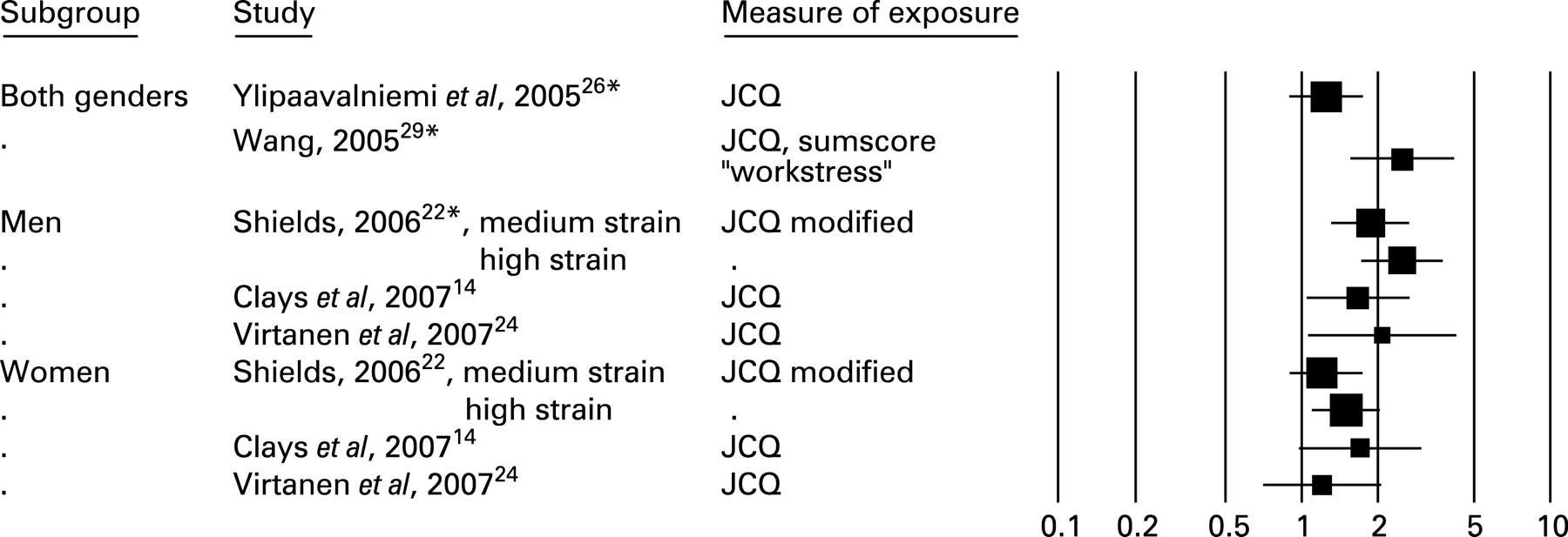
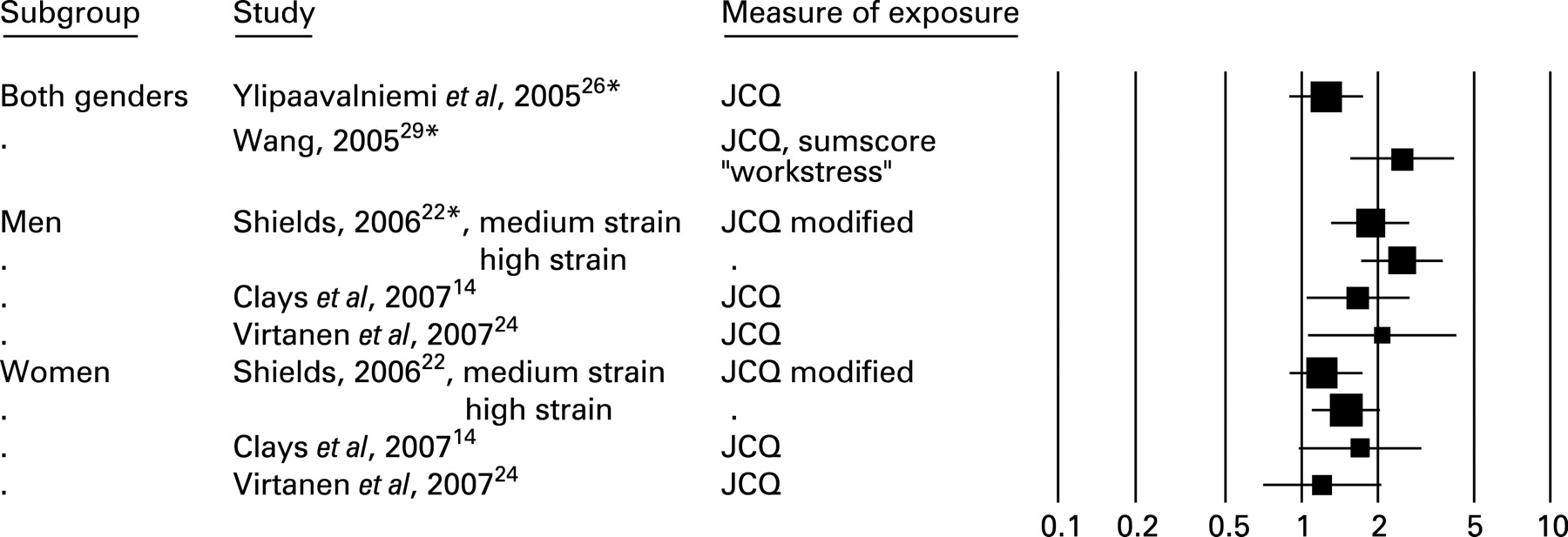
According to the three studies that provided relevant data, job strain defined as a combination of high demands and low decision latitude was related to an increased risk of subsequent depression among men but less so among women (fig 4). One study provided indications of an exposure–response relationship with respect to the intensity of exposure.22 The risk attributable to strain was not adjusted for the effects of job demands and decision latitude and in all analyses the reference group was a low-demand, high-control group.
Few studies have focused upon other aspects of the psychosocial work environment such as effort–reward imbalance, organisational injustice, undesirable work events and bullying, but findings suggest that all these factors are associated with an increased risk of depression23 25 or depressive symptoms.15 26 28 31 Significantly elevated risk estimates ranged between an OR of 1.4 (95% CI 1.0 to 2.4) in relation to organisational injustice26 and 2.3 (95% CI 1.5 to 3.4) in relation to bullying.28
DISCUSSION
The systematic search of the scientific literature identified 16 follow-up studies that explored the risk of depressive disorder or symptoms in relation to psychosocial factors in the workplace. With few exceptions, these studies suggested an elevated risk in both men and women and the risk seemed not to be particularly dependent on the type of stressor, diagnostic criteria or the duration of the follow-up period. Is it likely that the observed associations are causal and that an improvement in psychosocial health in the workplace could reduce psychiatric morbidity?
Many cross-sectional studies of job-related depressive disorders were not included in this review because they were not expected to provide information on causal relationships, firstly because self-reported data on perceived stressors and health outcome are not independent, and secondly because they introduce the risk of circular reasoning.34 However, 15 of the 16 longitudinal studies included in this review were based upon perceived stressors in the workplace as well as self-reported depressive symptoms. Some studies excluded employees who fulfilled the outcome criteria at baseline and other studies only adjusted risk estimates for baseline case status. One study demonstrated how profoundly the risk estimate was changed when baseline cases were excluded.16 The longitudinal design and the exclusion of cases at baseline does not rule out that associations between perceived stressors and later reporting of depressive symptoms reflect the way that the individual perceives and interprets their surroundings.35 Moreover, unmeasured subclinical depression at baseline may influence individual reporting of psychosocial factors in the workplace. Few studies controlled for minor psychiatric morbidity or negative affect at baseline and it is uncertain if such procedures effectively control this type of potential confounding. Therefore, the belief that adjusting for locus of control, neuroticism and similar constructs solves the problem may be too optimistic. There is an obvious lack of studies that provide independent measures of stressors and outcome, for instance by relating disease occurrence to identifiable undesirable events in the workplace or by using aggregated measures of psychosocial factors wherever applicable.25 36 The lack of independence between measurements of exposure and outcome and uncertain timing of exposure relative to disease onset are considered a major limitation of current evidence. Studies of work events in analogy with life events may be one path to follow in future studies. Thus, a large number of studies consistently and strongly reveal how the death of a spouse is associated with subsequent depression with a relative risk of 24.3 during the first year, 9.0 during the first 2 years and 3.1 during the first 3 years (for original references see Bruce37). Two of the reviewed papers attempted to clarify the impact of undesirable events that took place in the workplace and observed a moderately increased risk of depression.18 23 However, the identification of life and work events is, by necessity, retrospective and thus subject to recall bias.
The reported risk estimates were rather consistent across studies but were generally only slightly or moderately elevated with a relative risk below 2, which suggests that residual confounding may an important issue. A number of well-known risk factors for depression including gender, age, income, educational level, unemployment and marital status were adequately dealt with in most studies, while several other known or likely strong risk factors such as life events (separation, premature death, crime, etc), personality traits, family history of depressive disorder, chronic disease and earlier psychiatric morbidity were not. Moreover, in elderly participants, vascular causes of depressive episodes were of importance.38 Such factors may produce biased risk estimates in longitudinal studies because of reversed causality. Thus, Kivimaki et al demonstrated that people who had depression at baseline were more likely later to report onset of bullying.28
The risk of depression is surprisingly uniform across a large number of different psychosocial dimensions and it is generally of similar magnitude in men and women. This apparent lack of specificity between exposure and effect points to confounding by some common correlated factor, which is most likely related to measurements of exposure and effect. On the other hand, findings may, of course, also indicate that psychosocial factors of different types contribute equally to the outcome. Current evidence does not provide clues as to which of the two alternative explanations is the more likely.
The demand-control-support model predicts that individuals with high-strain jobs characterised by high demands in combination with low control (decision authority and skills discretion) and possibly low social support in the workplace (isolated strain: iso-strain) are at high risk of disease. Six papers examined the effect of high strain or iso-strain, but only one study adjusted the risk estimates for the main effect variables and found no effect of the interaction terms.14 In a strict sense, none of the studies therefore lend support to Karasek’s and Theorell’s job strain and iso-strain hypothesis. Interestingly, the same applies to the two studies addressing the effort–reward imbalance model: none examine the effects of the interaction between effort and reward.15 An elevated risk of depression according to effort–reward imbalance therefore cannot be claimed to be, in fact, a true interactive effect or to be due to either high effort or low rewards or additive effects of both.
Main messages
Many recent large follow-up studies indicate that perceived psychosocial job strain is related to a moderately elevated risk of major depression.
More research is needed to determine whether observed associations are causal and to provide a solid basis for targeted preventive measures.
Policy implications
Managers and workplace officials should take into account that high job demands, low decision latitude, effort–reward imbalance and organisational injustice in the workplace may possibly trigger depressive episodes.
Current evidence that psychosocial factors in the workplace can contribute to depression is far from conclusive.
The included follow-up studies are not true incidence studies. Some did not exclude subjects fulfilling the outcome criteria at baseline, and the majority examined the prevalence of the outcome measure at the time of follow-up or after 12 months. The time relationships between exposure and outcome were thus heterogeneous across the studies. Contrary to expectations, the risk estimates were not attenuated in studies with long follow-up time and several years’ time lag between the measurement of exposure and outcome. With few exceptions, exposure intensity–response relationships were not examined and no studies included analyses of the duration of adverse psychosocial work factors.
This review was restricted to studies that explicitly addressed depressive disorders or symptoms of depression, so a large number of studies exploring mental health in broad terms were left out in order to achieve more specificity. It should be acknowledged, however, that the outcome criteria differed across the studies. Although the true prevalence of depression may vary from one population to another, the large variations in the prevalence of the outcome in this review (2.5–33%) clearly point to the heterogeneous nature of the outcome. Some studies reported a modest relationship between self-reported symptoms of depression and clinically diagnosed depression39 and others reported strong correlations.40 41 The majority of studies did not address the risk of major depressive episodes in a strict clinical sense, rather they reported less severe conditions without sharp boundaries between minor psychiatric disorders and well-being. Studies focusing on the risk of clinical depression are needed to better understand how psychiatric disorders can be prevented by improving the psychosocial environment in the workplace.
Depressive disorder is a recurrent disease. Following the first depressive episode, most patients experience another spell of depressive symptoms during their lifetime. Risk factors for the first depressive episode may differ from those of subsequent episodes.7 Thus, anxiety disorders are more strongly related to subsequent episodes of depressive disorder than to the first episode, which may be explained by selection: the more susceptible personalities are at greater risk of a subsequent episode than the average individual who experiences a first-onset episode. For this reason, analytical studies of risk factors for depression should be restricted to the first episode. Only one study examined first-onset major depressive episodes14and did not support the hypothesis that stressors at work other than work events increase the risk of depression.
Summarising the findings across studies by means of meta-analytical methods was considered, but this idea was abandoned because, although technically possible, the heterogeneity of the studies with respect to both exposure and outcomes in combination with the limitations discussed above would render such an approach unfeasible. After all, the main issue at present is not to obtain the best possible estimate of the strength of an association but to balance the weight of the evidence with respect to causality of relationships between job stressors and onset of major depression.
A recent meta-analytical review focusing on the psychosocial work environment and mental health concluded that there is robust, consistent evidence that high demands and low decision latitude and high efforts and low rewards are prospective risk factors for common mental disorders, suggesting that the psychosocial work environment is important for mental health.11 This is in keeping with another review that found good evidence of causal effects of work characteristics on well-being.10 The present review differs from the previous reviews in its more rigorous selection of outcome. There is little reason to doubt that the work environment may impact on well-being and self-reported mental health in broad terms, but according to the present review, it cannot be ruled out with confidence that observed associations between perceived psychosocial work environment and the onset of depressive disorder are biased or confounded.
CONCLUSION
This review provides rather consistent findings indicating that perception of psychosocial stressors in the workplace is related to an elevated risk of subsequent onset of depressive symptoms or a major depressive episode, but several methodological limitations preclude causal inference. With few exceptions, measurements of exposure and outcome based upon self-reporting cannot be considered independent and they are likely to inflate risk estimates. Studies that implement objective measures of stressors or independent outcome ascertainment are encouraged.
Acknowledgments
The study was supported by a grant from the Danish Working Environment Research Fund.
Appendix A
| PubMed search terms used for a systematic review of original papers on the risk of depressive disorders in relation to strenuous psychosocial work environment | |
| Search using medical subject heading (MeSH) | |
| Outcome | (“Mental Disorders/classification”[MeSH] OR “Mental Disorders/epidemiology”[MeSH] OR “Mental Disorders/etiology”[MeSH] OR “Mental Disorders/prevention and control”[MeSH] OR “Mental Disorders/psychology”[MeSH] OR “Mental Disorders/statistics and numerical data”[MeSH]) |
| AND | |
| Exposure | (Occupation[MeSH] OR Work[MeSH] OR Employment[MeSH]) |
| AND | |
| Risk | (Risk [MeSH]) |
| Search using free text strings in all fields | |
| Exposure | (Depression OR depressive symptoms OR mood disorder OR affective disorder AND (has abstract[text] AND (Humans[MeSH]) AND (English[lang]) AND (Journal Article[ptyp])) |
| AND | |
| Outcome | (“job demand*” OR “job control” OR “demand control model” OR “Karasek*” OR “effort reward imbalance” OR ERI OR “organisational injustice” OR “occupational stress” OR “work stress” OR “job stress” OR “psychosocial stress” OR “job strain” OR “psychosocial work environment” OR “psychosocial job characteristics” OR “psychosocial working conditions” OR occupation OR employment OR “psychosocial factors” OR bullying OR “long working hours” OR “work event*”) AND (has abstract[text] AND (Humans[MeSH]) AND (English[lang]) AND (Journal Article[ptyp])). |
REFERENCES
Footnotes
Competing interests: None.