Article Text

Abstract
Objectives: To examine the influence of an airway diagnosis in adolescence on future health and occupation in Swedish men.
Methods: Data were collected from the linkage of four Swedish national registers: the Military Service Conscription Register, the Population and Housing Censuses, the Inpatient Care Register and the National Cause of Death Register. A job-exposure matrix for airway-irritating substances was developed for application on the conscription cohort. The cohort included 49 321 Swedish men born 1949–51. Three groups—(1) healthy, (2) asthmatics (mild and severe asthma) and (3) subjects with allergic rhinitis without concurrent asthma—were identified at conscription and analysed for mortality, in-patient care and strategies for choice of occupation with emphasis on airway-irritating job exposure. Analyses were adjusted for smoking and childhood socioeconomic position.
Results: The prevalence of total asthma was 1.8%, severe asthma 0.45% and allergic rhinitis 2.7%. Mortality for all causes was significantly higher in total asthma, hazard ratio (HR) 1.49 (95% CI 1.00 to 2.23), and lower in allergic rhinitis, HR 0.52 (95% CI 0.30 to 0.91). Asthma was a risk factor for inpatient care while allergic rhinitis was associated with less in-patient care (odds ratio (OR) for total asthma 1.16 (95% CI 1.00 to 1.34), severe asthma 1.38 (95% CI 1.04 to 1.85), allergic rhinitis 0.92 (95% CI 0.82 to 1.03)). Those with asthma tended to avoid jobs with a high probability for airway-irritating exposure (OR 0.88, 95% CI 0.71 to 1.09), but not to the same extent as subjects with allergic rhinitis (OR 0.58, 95% CI 0.47 to 0.70) (ORs from 1990).
Conclusion: Subjects with asthma did not change their exposure situation to the same extent as subjects with allergic rhinitis. Further, asthmatics had an increased risk for morbidity and mortality compared to healthy subjects and subjects with allergic rhinitis.
Statistics from Altmetric.com
Main messages
By applying ajob exposure matrix (JEM) for airway-irritating agents to a population cohort, we found associations between sensitive groups and exposure.
This study shows that subjects with asthma have jobs with airway-irritating exposure almost as often as healthy subjects, while subjects with allergic rhinitis avoid such exposure.
Further, asthmatics have an increased risk for morbidity and mortality compared with healthy subjects and subjects with allergic rhinitis.
Asthma and allergies are common chronic diseases affecting all age groups.1 About one child in four2 and one adult in three3 suffer from atopic diseases. Subjects with allergy and other hypersensitivity react at lower levels of irritating substances than healthy subjects do. Further, repeated exposure can lead to an unspecified reactivity, aggravated symptoms and even chronic conditions. In occupational life many workers have daily contact with dust, solvents or gases that might irritate airways and skin, and many report respiratory symptoms or skin disorders as a result of such exposure.4 Work disability from respiratory disease, especially asthma, is common and costly in the working population and people with asthma have also been found to change job more often than those without.5 Even upper respiratory tract complaints that are generally considered to be non-disabling, such as allergic rhinitis, have been associated with prominent decrements in work productivity.6 Although it is known that people with allergy and other hypersensitivity are more affected by irritating exposures, the long-term consequences of allergy in working life are not well known.
Nationwide registers in combination with the unique personal identification code in Sweden give an important opportunity for record linkages to be used in large epidemiological studies. We used the 1969/70 Conscription cohort7 linked to the Population and Housing Censuses, the Inpatient Care Register and the National Cause of Death Register. Furthermore, a job-exposure matrix (JEM) for airway-irritating substances was developed for application on the conscription cohort.
The aim of the present study was to elucidate the consequences of an airway diagnosis at enrolment on the adult life of Swedish men. What coping strategies are used by men with an airway diagnosis—do they avoid occupations with high risk of being exposed to airway-irritating substances? Is an airway diagnosis a risk factor for overall mortality? Are airway diagnoses associated with in-patient care in general and for respiratory diseases in particular?
METHODS
The conscription cohort
The study was based on data from a nationwide survey of 49 321 Swedish males, born in the years 1949–51, who were conscripted in 1969/70. They accounted for 97.7% of all conscripts in 1969/70, the remaining 2.3% having been born before 1949. Only 2–3% of all Swedish men were exempted from conscription at the time, in most cases due to severe handicaps or congenital disorders. Chosen variables from the conscription cohort are described below, and demographic characteristics are reported in table 1.
Variables
At conscription all conscripts were seen by a physician, who diagnosed formal disorders according to the Swedish version of the ICD, 8th revision (ICD-8). Diagnoses were based on written criteria and asthma was rated for severity from a military medicine perspective. In the present study we translated the grades “insignificant” to “fairly significant” (including four grades) as being a mild affliction, and “significant” to “very significant” (including four grades) as a severe affliction.
We studied the airway diagnoses asthma (ICD-8 = 493) and allergic rhinitis (ICD-8 = 507). Four subjects (0.45%) in the asthma group had no rating for severity.
Subjects without asthma or allergic rhinitis but with a diagnosis for bronchitis (ICD-8 = 490–491), atopic eczema (ICD-8 = 691), non-atopic eczema (ICD-8 = 692) and/or urticaria (ICD-8 = 708)—in total 1.5% of the conscripts—were excluded from the analyses.
Prevalence of airway diagnoses at conscription is listed in table 1. Allergic rhinitis and asthma accounted for less than 5%. Among asthmatics, about one quarter had a severe asthma. In this group the majority were exempted from compulsory military service due to asthma.
The following groups were studied: (1) total asthma (n = 871) and the subgroups severe asthma (n = 224) and mild asthma (n = 643); (2) allergic rhinitis (n = 1330) including subjects with allergic rhinitis without concurrent asthma; (3) healthy (n = 45 470), without any of the diagnoses mentioned above.
By means of personal identification number, the database was linked to the Inpatient Care Register and the National Cause of Death Register, held at Sweden’s National Board of Health and Welfare and the Population and Housing Censuses held by Statistics Sweden. The Inpatient Care Register records all hospital episodes with a diagnosis (ICD-8) for patients treated in any hospital in Sweden. Diagnoses were recorded at discharge of the patient. In the present study we used the primary diagnosis for in-patient care. We studied in-patient care during the years 1971–2003 for asthma (ICD-8 = 493) and for any in-patient care with a diagnosis.
Mortality in the cohort was followed up during 1969–2002 using data from the National Cause of Death Register. In the present study we used: (1) all causes of mortality and (2) date of death.
Information on occupation for each conscript was obtained by record linkage with the National Population and Housing Censuses which were carried out every fifth year between 1960 and 1990 in Sweden. The occupations reported in the censuses were coded according to the Nordic modification of the three-digit International Standard Classification of Occupations, NYK (1974).
Job-exposure matrix
A job-exposure matrix was developed for application on the conscription cohort. The exposure axis of the matrix includes 18 agents known to have an irritating effect on the respiratory system, such as organic solvents, irritating gases, cold air, and organic and inorganic dusts. Some of the irritating agents are also allergens (for example, flour, furred animals and isocyanates).
The job axis comprises all occupations on the Swedish labour market, classified in 281 job families according to NYK (1974). The sources of information were Swedish national workplace surveys and international literature8–11 as well as discussions with experienced occupational hygienists. When available, hygienic control measurements from 1970/80 were consulted.
As a first step in the construction of the matrix, a selection was made of all job families for which at least 10% of the individuals were estimated to be exposed to any of the chosen substances for more than one h/week in 1970/80. Assessment of exposure required an air concentration in the work environment significantly higher than the public exposure.
In each job family selected in the first step, all individual jobs involved were studied to get a picture of the included tasks and, based on this, the exposure for each of the agents in the matrix was assessed. Some job families were not assigned any exposure, while others were assigned many different ones. In some cases no exposure assessment was feasible, mainly because of a too inhomogeneous exposure situation within the job family including both unexposed and exposed tasks. As not all jobs in a job family are exposed, the probability of being exposed was classified as high (>2/3 exposed), moderate (1/3–2/3 exposed) or low (1/10–1/3 exposed).12
Fifteen per cent of the occupations in the JEM were estimated to have a high probability for exposure, 14% a moderate probability for exposure, 18% a low probability for exposure and 43% were assessed as unexposed (probability less than 1/10 to be exposed). No exposure assessment was feasible in 11% of the job families.
In 1970 the men were 19–21 years old and only 60% reported an occupation. Employment increased to 86% in 1975 and reached 92% in 1980–90. Unemployed subjects were not considered as being unexposed because they could have one or several jobs during the following five-year period until next report of occupation. Occupational exposure during the follow-up period for the whole cohort and for healthy individuals, asthmatics and subjects with allergic rhinitis was studied by analysing (1) the distribution of employment in exposed and unexposed occupations, and (2) the number of years in an exposed occupation.
Confounders
Smoking was controlled for in the analyses because asthma is known to be affected by smoking.13 Several studies have also shown that smoking is a risk factor for mortality, an association also seen in the conscription cohort.14 15 Data on self-reported smoking habits were given by 98.4% of the men at the time of conscription, indicated as 0, 1–5, 6–10, 11–20 or >20 cigarettes/day.
The father’s socioeconomic position was identified and controlled for, as previous studies on Swedish conscripts have revealed associations between socioeconomic position and allergy diagnoses16 and also mortality.17 The conscripts and their parents, and other head of household when different from the parents, were linked to each other between censuses through their personal identification numbers by Statistics Sweden. Information on childhood socioeconomic position was obtained from the National Population and Housing Census of 1960 (response rate 99%)—that is, when the subjects were 9–11 years old. Four different childhood socioeconomic groups were employed in the present study: children of (1) farmers, (2) manual workers, (3) low and intermediate non-manual employees and (4) higher non-manual employees. In the cohort 97.7% were classified on childhood socioeconomic position. The remaining 2.3% had no data on socioeconomic position and were excluded from the analyses.
Statistics
All statistical analyses were performed with SPSS version 14.0 (Chicago, IL, USA). All results were controlled for smoking and childhood socioeconomic position unless otherwise stated. Differences in mortality between healthy individuals, those with asthma and subjects with allergic rhinitis were tested using Cox regression analysis, giving a hazard ratio. Differences in proportions of subjects with an airway diagnosis and healthy subjects in exposed and unexposed jobs were tested with logistic regression analysis, resulting in an odds ratio. Differences between groups regarding the years spent in an exposed occupation were analysed with linear regression.
The study was approved by the Regional Ethical Review Board in Stockholm.
RESULTS
Confounders
More than half of the men, 28 424 (57.6%), were smokers at the time of conscription. The prevalence of smoking in healthy subjects (59.0%) and those with mild asthma (58.4%) did not differ significantly, while there were significantly fewer smokers in those with severe asthma (50.0%), OR 0.72 (95% CI 0.55 to 0.94) and allergic rhinitis (50.2%), OR 0.724 (95% CI 0.64 to 0.80). Odds ratios were controlled for childhood socioeconomic position. Smoking was also correlated to exposure. Among subjects with a high probability for exposure in 1980, 65.7% were smokers, compared to 50.3% among unexposed subjects.
The total asthma prevalence was 1.7% in all childhood socioeconomic groups except for farmers, who had a higher asthma prevalence, 2.5% (n = 138). Allergic rhinitis was more common in the offspring of higher non-manual employees 4.3% (n = 110), than in low and intermediate non-manual employees, 3.9% (n = 515), and in manual workers, 2.1% (n = 564). Farmers’ children had the lowest prevalence of allergic rhinitis, 2.0% (n = 106).
Childhood socioeconomic position reflects educational level. In 1990, 40.4% of subjects with allergic rhinitis had a higher education than upper secondary school compared to 29.4% in total asthma and 26.2% in healthy subjects.
Mortality
There were 55 (6.3%) deaths among men with an asthma diagnosis at enrolment, 16 deaths (7.1%) in the subgroup severe asthma and 2152 (4.7%) among healthy subjects during 1969–2002. Men with allergic rhinitis had the lowest mortality of all groups—34 deaths (1.5%). Mortality was significantly higher in total asthma, HR 1.49 (95% CI 1.00 to 2.23), and lower in allergic rhinitis, HR 0.52 (95% CI 0.30 to 0.91) (fig 1). The analyses were controlled for smoking and childhood socioeconomic position, although the confounders only had a marginal influence on the results.

In-patient care
During 1971–2003, the follow-up period for in-patient care, 30 290 (61.4%) subjects had at least one in-patient care occasion with any diagnosis. In-patient care for asthma occurred on 178 (0.36%) occasions (table 2). The prevalence of in-patient care with any diagnosis was in healthy subjects 61.5%, in total asthma 65.0%, in severe asthma 68.3% and in allergic rhinitis 58.3%. Odds ratios for in-patient care are presented in table 2. In-patient care for asthma was, as expected, most frequent in the asthma groups; 9.4% in severe asthma and 5.3% in total asthma. Furthermore, the group with allergic rhinitis had more asthma care than healthy subjects—0.5% and 0.3% respectively.
Job exposure
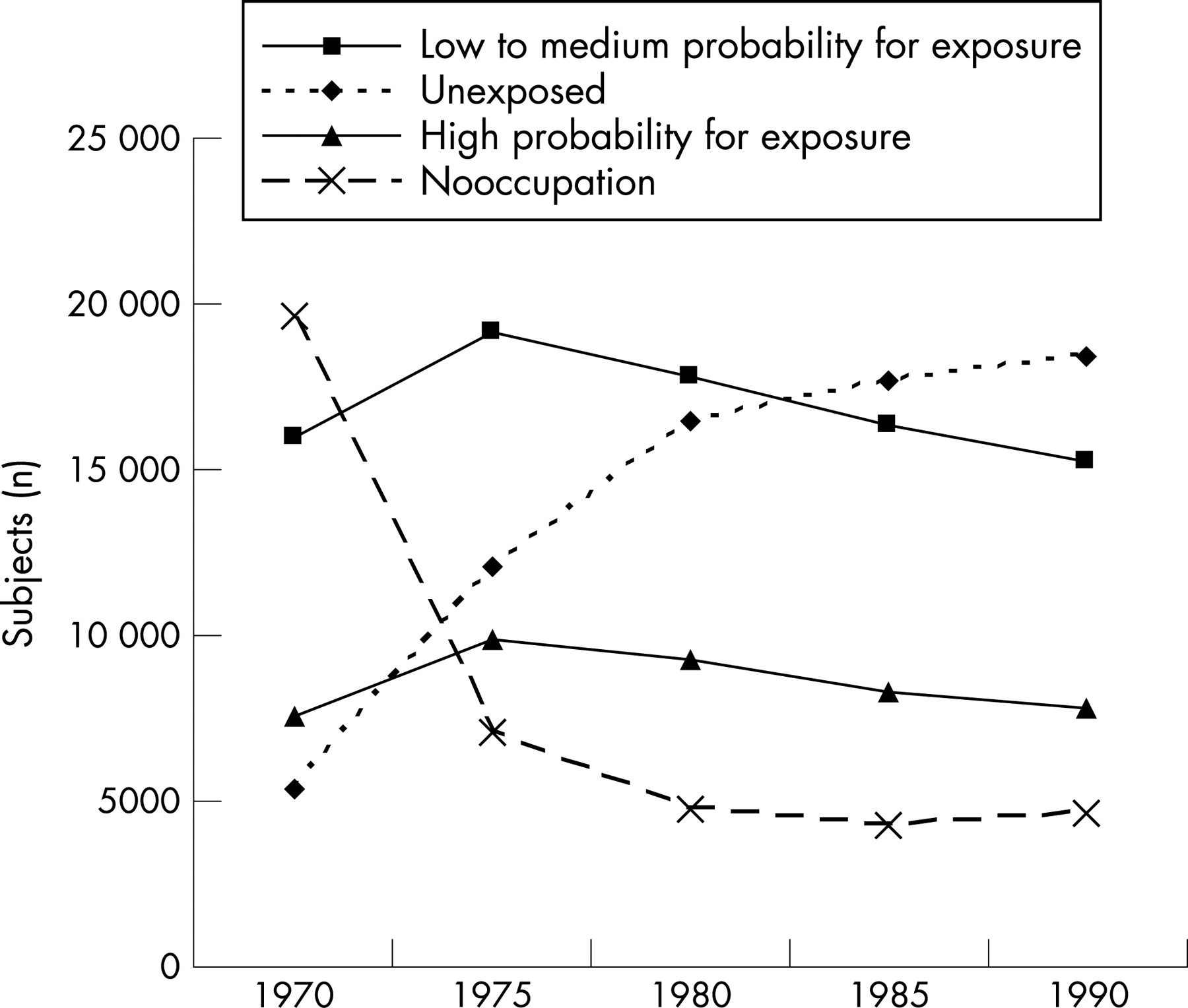
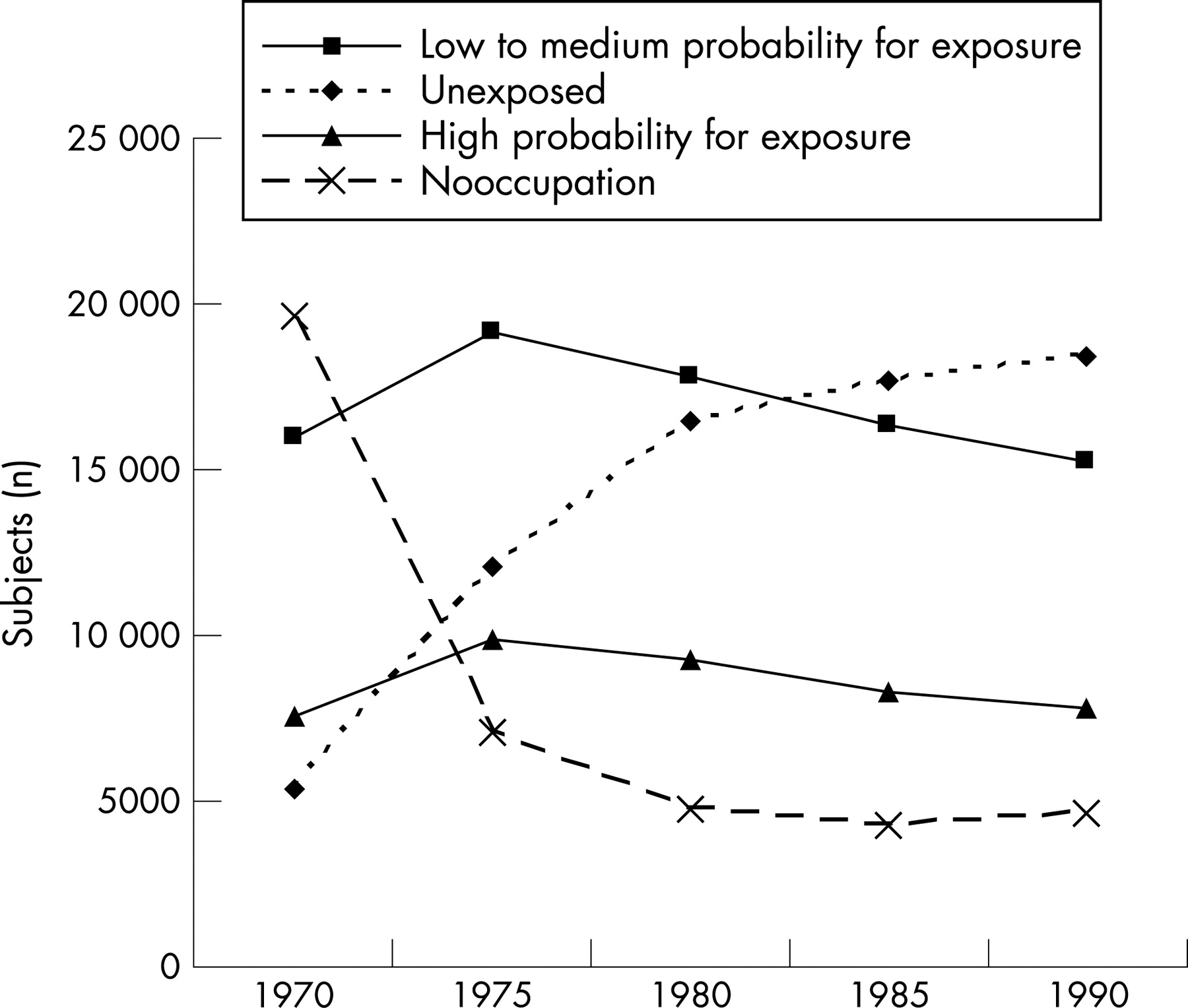
By applying the JEM on the conscription cohort, occupations during the follow-up period 1970–90 were graded for exposure. Figure 2 shows that exposed jobs dominated in the beginning and were fairly stable during the whole period, whereas unexposed jobs were few in the beginning and increased steadily during the period. Jobs not feasible to assess for exposure, due to an inhomogeneous exposure situation within the job family, were proportionally infrequent in the cohort—1.8% in 1970 and 6.5% in 1990 (not shown in the figure). These jobs included both exposed and unexposed tasks.
The likelihood for subjects with an asthma diagnosis, in relation to healthy subjects, to have an exposed job (with low and high probability for exposure) is presented as OR in figure 3A. In figure 3B the corresponding OR for subjects with allergic rhinitis is shown. Odds ratios were controlled for smoking and childhood socioeconomic position. Asthmatics tended to avoid jobs with a low to medium probability for airway irritating exposure and they avoided jobs with high probability for exposure to the same degree (fig 3A). Asthma severity had no influence on the results.

{kind=link}
{kind=link}
{kind=link}
Subjects with allergic rhinitis less often had exposed jobs compared to healthy and asthmatic subjects, and the likelihood for subjects with allergic rhinitis to have a job with a high probability for exposure was even lower. This finding, that exposed jobs are less usual among subjects with allergic rhinitis than among those with asthma, was seen in all childhood socioeconomic groups except for in farmers. Among farmers’ children the likelihood for asthmatics to have a job with a high probability for exposure was as low as for subjects with allergic rhinitis.
There were no differences in unemployment between healthy subjects and subjects with asthma or allergic rhinitis, but proportionally fewer subjects with allergic rhinitis had a job in 1970 and 1975, which is in agreement with their higher educational level.
During the follow-up period 1970–90 the healthy group spent on average 13.2 years in exposed occupations, all those with asthma 12.6 years (p = 0.010), the subgroup severe asthma 12.4 years (p = 0.10) and subjects with allergic rhinitis 11.7 years (p<0.01). The group that received in-patient care for asthma spent the longest time in exposed jobs, 14.1 years (p = 0.11). The presented figures are controlled for smoking and childhood socioeconomic position.
DISCUSSION
Our most interesting finding in the present study from enrolment 1969/70 was that an asthma diagnosis in adolescence only marginally influenced the choice of job and airway irritating exposure. However, subjects with allergic rhinitis less often had exposed jobs and particularly jobs with a high probability for exposure. Whether this depends on differences in experienced symptoms is still to be revealed. Further, the study presents evidence that asthmatics have a higher mortality and consume more in-patient care for respiratory causes as well as for all causes, also after controlling for smoking and childhood socioeconomic position.
Our study has several strengths: the cohort includes 97.7% of the Swedish men that were conscripted during one year—that is, the whole male population is represented in the cohort. Further, the conscripts were followed for 30 years and the follow-up information was collected from national registers linked to the conscript’s unique identification code. The fact that asthma and allergic rhinitis are based on a doctor’s diagnosis, at a defined age and graded for severity, provides our study with a distinct advantage through greater diagnostic homogeneity as compared with case definitions by either self-reported or questionnaire-based symptoms (that is, the methods often used in population-based studies). In a validation of diagnoses at the conscript examination the sensitivity was 80% for asthma and allergic rhinitis18 (the specificity was not reported). Thus, a test-based diagnosis would have increased the sensitivity and could provide important information about bronchial reactivity and allergy (immunology), especially if the same test method is used consistently. The diagnosis was however graded for severity in order to assess the capacity of the conscripts, which may be relevant also for assessment of the capacity in work life. We can also assume that the diagnoses in the cohort contain early-onset conditions only, as the subjects hardly had developed occupational related asthma or rhinitis at the age of 18–20 years, when the diagnoses were set.
We also had information on childhood socioeconomic status and smoking at conscription—two important confounders when studying the consequences of asthma and allergy. The prevalence of smoking was high (58%) in the conscription cohort in 1969/70 when smoking was reported and was, as expected, less frequent in subjects with an airway diagnosis. Smoking has decreased in all age groups since then and today 10% of Swedish 18–20 year old men are smokers, according to the Swedish survey of living conditions 2002.19 However, in the present study, smoking had no significant influence on mortality in asthma and allergic rhinitis.
We chose to control for the conscript’s childhood socioeconomic position because circumstances early in life might influence the development of asthma and allergy. Farmers’ children were distinguished as having proportionally less allergic rhinitis than subjects from other socioeconomic groups, which is consistent with findings that farming prevents the development of allergic disorders in children.20 Farmers are however exposed to many agents which are risk factors for respiratory diseases,21 22 supporting the higher prevalence of asthma in farmers’ children in the conscription cohort.
The increased mortality risk from all causes for those with asthma in the present study is comparable to those reported in previous studies: Markowe et al23 found increased mortality from all causes RR 1.6 (95% CI 1.3 to 2.0); Huovinen et al24 found an age-adjusted RR of 1.5 (95% CI 1.1 to 2.1); and Vandentorren et al25 found (after adjustment for age, sex, educational level, smoking habits, occupational exposure and forced expiratory volume in one second) an increased RR of death by 1.2 (95% CI 1.0 to 1.4). The agreement of mortality risks for asthma support the assumption that the asthma diagnoses in the present study are relevant.
In a study by Radon et al adolescent vocational trainees were asked about the type of job they would like to have in the future.26 Only subjects that had not been occupationally exposed during training were included in the study. The authors found that subjects with allergic rhinitis tended to avoid highly exposed jobs. This association was not found in subjects with asthma. These results agree with the results of the present study.
The fact that those with asthma only marginally avoided jobs with a high probability for exposure may partly be a consequence of the lack of relevant occupational guidance before entering working life. Knowledge about work-life exposure and its impact on asthma was limited in 1970 and the occupational guidance had no information for people with asthma about which jobs posed risks. Although one would expect subjects with severe asthma to be more carefully guided, we found that they had exposed jobs as often as subjects with mild asthma. This indicates that subjects with severe asthma did not follow advice, even if it was provided.
Allergic rhinitis is frequently reported to be more prevalent in non-manual employees,16 28 and in the present study allergic rhinitis was most common in children of higher non-manual employees, and differences in mortality, in-patient care and avoidance of exposed jobs remained after controlling for childhood socioeconomic position. One may speculate that parents, regardless of socioeconomic position, who are attentive to the health of their children, are also more engaged in their education. This could lead to a misclassification of diagnoses, with a higher proportion of diagnoses reported in subjects with a higher education. If this is true, our interpretation that subjects with allergic rhinitis avoid exposure due to medical conditions may not be the whole explanation. However, controlling for educational level in 1990 did not affect the odds ratio for subjects with allergic rhinitis to be in an exposed job.
Estimates of the occupational impact of rhinitis are limited. The occupational form of rhinitis may however have a profound effect on the worker, resulting in performance deficits, reduced productivity and psychosocial problems.29 In a study by Blanc et al, on 125 subjects with asthma and 175 subjects with rhinitis, the subjects with asthma were less likely to be employed at all while among those remaining at the job, rhinitis was a more potent cause of decreased job effectiveness.6 The results were not controlled for exposure at work but the educational level was somewhat higher in subjects with rhinitis, which often is associated with less exposed jobs. A subject with rhinitis, with an already compromised health, will react at a lower exposure level and have a more severe reaction when exposed to airway irritating agents.
Asthma is a disease with different phenotypes and separating asthma into atopic and non-atopic conditions would probably give important information. In the present material only 15% (127/871) of the asthma cases had registered data on rhinitis or atopic dermatitis.
The present study is based on men because only men are included in the conscription cohort. It would be valuable to have the corresponding information on females. We are however not aware of any corresponding data source for females.
As previous research has showed that JEMs are optimised when specificity is favoured over sensitivity,30 a job was classified with a high probability for exposure only if more than two thirds were expected to be exposed in that job. It is important to consider that one job family may include different tasks with different exposure situations. This also means that subjects who experience problems due to job exposure may be transferred to a less exposed task within the job family. However this does not explain why those with asthma are less prone to choose an unexposed job compared to subjects with allergic rhinitis.
The fact that the JEM is constructed on job families that may contain several exposure situations also means that exposure differences detected when using the JEM is probably diluted. Therefore, the differences seen in the present study are probably even greater than we have shown.
The results from this study concern subjects born in 1950 with a confirmed diagnosis for asthma and allergic rhinitis in 1970 when these diagnoses were less prevalent than today. It should be pointed out that these days asthma and allergic rhinitis probably include a larger group of subjects with mild symptoms, resulting in less apparent effects of occupational exposure. The highly increased prevalence of asthma and allergic rhinitis today will however have significantly greater consequences for society than is apparent from the results of the present study.
It is evident from our results that subjects with asthma have deprived health, and we know from earlier studies that hazardous occupational exposure is correlated with an enhanced disability risk for those with asthma.4–6 31 32 Young subjects with asthma have been shown to have poor knowledge of the disease and many do not receive adequate treatment.33 Therefore, increased awareness in people with asthma of the asthma disease and how exposures in the environment affect them is necessary to improve their health.
CONCLUSION
Our conclusion is that subjects with asthma do not change their exposure situation to the same extent as subjects with allergic rhinitis. Further, those with asthma have an increased risk for morbidity and mortality compared with healthy subjects and subjects with allergic rhinitis.
Acknowledgments
We thank Helena Svensson at the Department of Occupational and Environmental Health, Stockholm County Council, for statistical help.
REFERENCES
Footnotes
Funding: The Swedish Asthma and Allergy Association.
Competing interests: None.