Article Text

Abstract
Background: There is no universally accepted way of labelling or defining upper-extremity musculoskeletal disorders. A variety of names are used and many different classification systems have been introduced.
Objective: To agree on an “unambiguous language” concerning the terminology and classification that can be used by all relevant medical and paramedical disciplines in the Netherlands.
Methods: A Delphi consensus strategy was initiated. The outcomes of a multidisciplinary conference were used as a starting point. In total, 47 experts in the field of upper-extremity musculoskeletal disorders were delegated by 11 medical and paramedical professional associations to form the expert panel for the Delphi consensus strategy. Each Delphi round consisted of a questionnaire, an analysis and a feedback report.
Results: After three Delphi rounds, consensus was achieved. The experts reported the consensus in a model. This so-called CANS model describes the term, definition and classification of complaints of arm, neck and/or shoulder (CANS) and helps professionals to classify patients unambiguously. CANS is defined as “musculoskeletal complaints of arm, neck and/or shoulder not caused by acute trauma or by any systemic disease”. The experts classified 23 disorders as specific CANS, because they were judged as diagnosable disorders. All other complaints were called non-specific CANS. In addition, the experts defined “alert symptoms” on the top of the model.
Conclusions: The use of the CANS model can increase accurate and meaningful communication among healthcare workers, and may also have a positive influence on the quality of scientific research, by enabling comparison of data of different studies.
- CANS, complaints of arm, neck and/or shoulder
- RSI, repetitive strain injury
- UECTD, upper-extremity cumulative trauma disorder
Statistics from Altmetric.com
- CANS, complaints of arm, neck and/or shoulder
- RSI, repetitive strain injury
- UECTD, upper-extremity cumulative trauma disorder
Multidisciplinary consensus on terminology and classification of upper-extremity musculoskeletal disorders is a first requirement for accurate and meaningful communication among clinicians. Universal classification of these conditions of the upper limb and neck is necessary to assess prognosis and options for treatment,1,2 to study the natural course of the conditions, and to compare research findings across geographic regions and time periods within different (working) populations.
In a systematic appraisal of worldwide prevalence rates,3 substantial differences in the reported prevalence rates of upper-extremity disorders were found. Point prevalence estimates ranged from 1.6–53% and the 12-month prevalence estimates ranged from 2.3–41%. It was concluded that one of the main reasons for the differences found in this latter study is the absence of a universally accepted taxonomy for upper-extremity musculoskeletal disorders.
A variety of terms for upper-extremity musculoskeletal disorders are used in different countries all over the world, including repetitive strain injury (RSI), upper-extremity cumulative trauma disorder (UECTD) and work-related upper-limb disorder (WRULD). Many different classification systems have been introduced. Van Eerd et al4 found 27 different classification systems for the working population. The systems differed in the disorders they included, in the labels used to identify the disorders and in the criteria used to describe the disorders.
Two sets of consensus criteria for upper-extremity disorders were recently proposed in the UK5 and in Europe.6 Both Harrington et al5 and Sluiter et al6 gave criteria for a limited number of upper-extremity disorders only. Despite their efforts, implementation of these criteria would have been easier if the experts, chosen by the researchers in both studies, would have been key persons chosen by representatives of the persons who have to work with the criteria in practice.
Until now, none of the proposed classification systems have resulted in a complete overview in which (in principal) all musculoskeletal upper-extremity disorders are evaluated and discussed for inclusion. Moreover, they did not produce a workable classification tool that can be used in daily practice in an easy way (ie, no special training and/or no substantial time needed to perform) by both researchers and health professionals.
Therefore, we concluded that there is a need for a classification system on musculoskeletal upper-extremity disorders that (1) could be generally accepted and used by all disciplines, (2) can support the diagnosis and classification of (in principal) all upper-extremity conditions and (3) is reported as a practical tool.
Our first aim is to achieve consensus in the Netherlands, with a further intention to use the results of this study to eventually achieve international consensus. The decisions made regarding classification were based on the international literature. To make implementation of the results of the project more feasible, we invited 11 medical and paramedical associations to assign delegates to participate in this consensus project (box 1).
Box 1 Participating disciplines
On behalf of the professional associations:
General practitioners
Physical and rehabilitation medicine specialists
Occupational physicians
Orthopaedic surgeons
Rheumatologists
Neurologists
Physical therapists
Exercise therapists Cesar
Exercise therapists Mensendieck
Occupational therapists
An unambiguous classification system that is accepted by all professionals involved may increase multidisciplinary cooperation and have a positive influence on the performance of studies and also allow data to be compared. This paper presents the results of the Delphi consensus strategy used to achieve consensus and the resulting model.
METHODS
The staff team
The staff team initiated and executed the Delphi consensus strategy. All three staff team members have an epidemiological as well as a clinical background. The epidemiologist/physician, the occupational health physician/psychologist and the health scientist/physiotherapist were responsible for the construction of the questionnaires, the analysis of the responses and the formulation of feedback. The staff team first initiated an invitational conference; the outcomes of this conference were used for the design of the first questionnaire of the Delphi consensus strategy.
Invitational conference
A multidisciplinary invitational conference (December 2002) was the starting point of the project. A total of 19 representatives of 10 of the 11 different medical and paramedical professional associations concerned with treatment of patients with upper-extremity disorders were present. Only one psychologist representing one national association was lacking. Structured group communication techniques were used at the conference to exchange ideas and expertise on the subject. The outcomes of the conference were used for further research to achieve the consensus.
Terminology
In the Netherlands, the term “RSI” is often used for symptoms of the arm or neck without a clear diagnosis. However, more than 90% of the participants of the conference were of the opinion that “RSI” is an unclear and confusing name for these ailments. During the conference, the staff team offered the participants a list of 14 Dutch and English terms used for upper-extremity musculoskeletal disorders that are frequently used in scientific literature and medical textbooks. The participants selected seven terms from this list and added one other term to it. The resulting eight terms were proposed in the Delphi-I questionnaire.
Definition
During the invitational conference, it became clear that the participants gave priority to a general and broad definition of upper-extremity disorders rather than to a narrowly described definition. It should include “complaints of pain”, “localised in the arm, neck and/or shoulder” and “no trauma involved”. Possibly “no systemic disease involved” could be included; “related to the musculoskeletal system” could be added to indicate that only musculoskeletal disorders should be considered. The participants chose not to mention the suspected aetiology of complaints in the definition.
Classification and model
Complaints meeting the general definition should be divided into diagnosable and non-diagnosable disorders. A diagnosable disorder should be defined as one with discernible characteristics, which can be diagnosed in a reproducible way. The diagnosis can be made through case history, physical examination, imaging and laboratory testing. It is important to realise that when a disorder is diagnosable, it does not necessarily mean that treatment is available.
During the conference, two models were initially discussed for the classification of patients (fig 1A,B). In model 1A the diagnosable and non-diagnosable disorders are two defined groups. Model 1B is largely similar to model 1A; however, the group “diagnosable disorders” was subdivided into separate disorders, which have to be mentioned and approached individually. The staff team decided to present both models in the Delphi-I questionnaire.
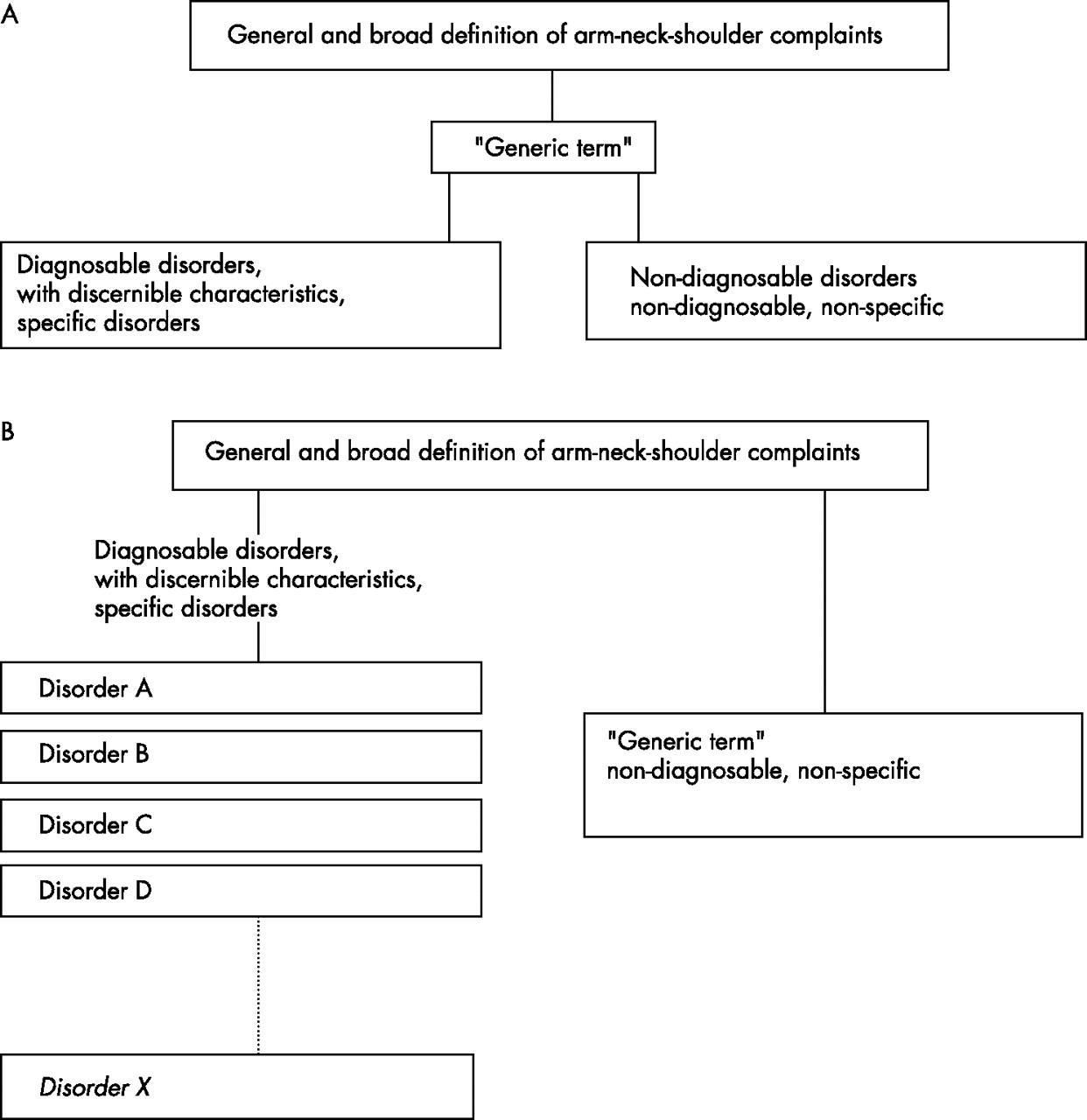
Two models for the classification of patients: model A and model B.
Delphi consensus strategy
Of all consensus techniques available, we chose the Delphi consensus strategy as our preferred method. In this method an expert panel is asked to answer questions concerning the subject. Then, through repeated feedback of the answers in several rounds involving all participants, the researchers try to develop consensus on opinions.7 The advantage of this method is that it is a written, anonymous method8 in which the opinions of the experts are combined whilst bias through institutional role, status or dominant personality is avoided.9
Selection of participants
The boards of the 11 relevant medical and paramedical associations in the Netherlands were asked to delegate a maximum of six experts each in the field of upper-extremity disorders, who were willing to participate in the expert panel.
Procedure
In the questionnaires of each Delphi round, we asked questions about term, definition and classification of complaints of the arm, neck and/or shoulder. We used structured questions with the answer formats “agree/don’t agree/don’t know” or “yes/no/don’t know”. For classification of the different complaints, the possible answers were diagnosable/non-diagnosable/no opinion. We invited the expert panel to give an explanation for their choices. After each round a feedback report was made to inform the expert panel about the answers and argumentations of the other experts. On the basis of the answers and arguments of the experts, the staff team decided which questions would appear in the next questionnaire. Staff team decisions were presented and justified in the feedback report.
Delphi-I questionnaire
The Delphi-I questionnaire was constructed using the outcomes of the invitational conference. The questionnaire of Delphi-I consisted of two parts. Part A contained questions concerning items for which 70% or more participants of the conference agreed on, and part B concentrated on the conflicting items. Items that were only discussed in small groups and not plenary were also included in part B. Separately, one question was included about the cut-off point for consensus concerning the whole Delphi survey.
Delphi-II and Delphi III questionnaires
The questionnaires of Delphi-II and Delphi-III were constructed using the results of Delphi-I and Delphi-II, respectively. The remarks of the expert panel were incorporated in the questionnaire of the next round. In this way, we collected and reported the opinions of the expert panel in each round in order to achieve consensus.
Analysis
The analysis of the responses from the Delphi rounds was both qualitative and quantitative. Qualitatively, two staff members independently analysed the answers of the expert panel; they compared the results of their analysis. Quantitatively, we reported for each question on how many participants gave which answers. Also, percentages were given of the positive and negative answers.
RESULTS
Expert panel
From January till March 2003, the 11 medical and paramedical professional associations selected 47 experts to form the expert panel for the Delphi consensus strategy. Experts from all 11 disciplines participated in the survey as delegates for their respective professional associations. Three experts, all Mensendieck exercise therapists, ended their participation during the process. Two of them only returned the Delphi-I questionnaire, the third did not return any of the questionnaires. Of the 46 experts, 44 (96%) returned the Delphi-I questionnaire; 40 (87%) and 43 (93%) returned the Delphi-II and Delphi-III questionnaires, respectively. The most common reason for non-response was ‘lack of time’. The final results of the Delphi consensus strategy—that is, the consensus model—were presented in October 2004.
Cut-off point for consensus
In the Delphi-I questionnaire a cut-off point of 70% agreement was accepted: Consensus was reached when ⩾70% of the experts gave the same answer to a question.
Term
In Delphi-I, it became clear that almost all experts (93%) gave priority to dispose of the term RSI. Although the term RSI has played an important role in recognising the extent of the problem, the term has led to negative associations concerning patients dealing with these problems. It was considered to be an umbrella term. Furthermore, the term was judged unclear and confusing: an injury is not always involved, and, besides “repetitive strain”, “static burden” also may generate the complaints.
In the Delphi-I questionnaire the expert panel was asked to rank the eight terms on the list composed of the outcomes of the invitational conference and to place their preferred name on the top. In this round they could also bring up other (new) terms. The staff team decided that the five terms which scored 70% of the votes in Delphi-I, complemented with another term given by one of the experts, would be used for the Delphi-II questionnaire. This list involved three English and three Dutch terms. In Delphi-II the expert-panel was asked to divide six points among both the English and the Dutch terms, separately. Elsewhere in Delphi-II, the experts were asked whether an English or a Dutch term should be used. In Delphi-II, consensus was reached about bringing into use an English term: CANS—complaints of arm, neck and/or shoulder.
Definition
In Delphi-I, the experts agreed to bring into use a general and broad definition. During Delphi-I and Delphi-II, all of the items mentioned in the conference were adopted, with a few minor changes. The expert panel decided to change “complaints of pain” into “complaints” because pain and also other sensations, such as tingling, can be involved.
Traumas such as fractures and ruptures needed to be excluded from the definition. However, micro-traumas can be involved in CANS. Therefore, the word “acute” was added to the element concerning the presence of traumata and became “no acute trauma involved”.
In conclusion, “complaints”, “localised in the arm, neck and/or shoulder”, “no acute trauma involved”, “no systematic disease involved” and “related to the musculoskeletal system” were included in the definition. In Delphi-III, consensus was achieved on the following definition of CANS: “Musculoskeletal complaints of arm, neck and/or shoulder not caused by acute trauma or by any systemic disease”.
Classification and model
Number of disorders classified
The staff team constructed a list of 29 disorders of the upper-extremity based on textbooks and the scientific literature. The experts added eight other disorders during Delphi-I. In total, the expert panel discussed 37 diagnoses that met the definition of CANS and classified these as diagnosable or non-diagnosable. During this process, six disorders were excluded from this list for various reasons (table 1). Finally, 23 disorders were classified as diagnosable and four as non-diagnosable.
Classification of complaints
Diagnoses excluded from classification
In Delphi-III, the experts decided to exclude the diagnosis “tendonitis of the wrist/forearm” from the list; this term was considered too general and specific disorders, such as De Quervain’s disease were already part of the list. The experts also decided to exclude the diagnoses “lung tumour” and “cardiac diseases”. Although these diseases can cause problems in the upper extremity, they are not related to the musculoskeletal system. Because the experts achieved consensus on excluding systemic diseases from CANS, they decided to delete rheumatic diseases from the list after Delphi-II. Although osteoarthritis is not a systemic disease, it was included within rheumatic diseases.
Shoulder complaints
In Delphi-I, a well-known clinical problem concerning musculoskeletal disorders of the shoulder, such as tendonitis and bursitis, emerged; they are difficult to differentiate but can be identified as a group. Therefore, some of the experts pleaded for the introduction of a generic term for these disorders, so that they can be classified as diagnosable. This idea was presented and adopted in Delphi-II. In Delphi-III, consensus was achieved to use the term “subacromial impingement syndrome” for the disorder that includes the rotator cuff syndrome, tendonitis of the m infraspinatus, m supraspinatus and m subscapularis, and bursitis in the shoulder area.
Non-diagnosable disorders
In Delphi-II consensus was achieved on the classification of the “tension neck syndrome” and “radiating neck complaints” (or “radiculopathy without a herniated disc”) as non-diagnosable.
In Delphi-III the experts decided that disorders for which no consensus about classification was achieved during the three Delphi rounds would be classified as non-diagnosable, until more information becomes available about the diagnostic criteria for the disorder. This was the case for the “thoracic outlet syndrome” and the “hand–arm vibration syndrome”.
Alert symptoms
It is generally known that a physician has to be aware of so-called “alert symptoms” while making a diagnosis. For example, symptoms may appear to be a result of complaints in the upper extremity, but are in fact caused by serious conditions such as angina pectoris. Diseases such as rheumatoid arthritis and osteoarthritis also need to be identified. To make sure that the symptoms of these disorders get the attention they need, the expert panel decided in Delphi-II to add “alert symptoms” at the top of the final model.
The CANS model and the flow chart
In Delphi-I, consensus was achieved to use model 1B (fig 1B) for the classification of patients. In Delphi-III the experts achieved consensus to use the terms “specific CANS” and “non-specific CANS” instead of “diagnosable-CANS” and “non-diagnosable CANS”. The whole model will be called the CANS model. A flow chart has been developed to help the doctor or paramedical therapist to classify the patient using the CANS model (fig 2). When complaints meet the definition of CANS, the clinician has to investigate whether or not one of the 23 disorders mentioned as specific CANS is present. If present, the diagnosis will be mentioned by its specific label, such as “carpal tunnel syndrome” or “lateral epicondylitis”. If not present, the complaints will be diagnosed as ‘non-specific CANS’.

{kind=link}
{kind=link}
The CANS model and flow chart.
DISCUSSION
The aim of the Delphi consensus strategy was to decide on an “unambiguous language” concerning the terminology and classification of complaints of the arm, neck and/or shoulder for all relevant medical and paramedical disciplines in the Netherlands involved in the treatment of patients with these complaints. After three Delphi rounds, multidisciplinary consensus was achieved and reported in the CANS model. As far as we know, this is the first time a multidisciplinary classification system on a national level has been developed in which all relevant medical and paramedical professions dealing with the treatment of patients with CANS were involved and in which (in principal) all musculoskeletal upper-extremity disorders were evaluated and discussed for inclusion.
Williams and Webb10 observed weaknesses in the Delphi consensus strategies, including (1) limited descriptions of experts’ characteristics, (2) imprecise definitions for consensus and (3) low response rates.
In a consensus procedure, there is a risk of bias in the selection of participants. In the present Delphi consensus strategy, 11 medical and paramedical associations selected the expert panel. In this way, the expert panel consisted of professionals with various medical and paramedical backgrounds, all seen as experts on upper-extremity disorders within their own discipline. In a decision-making group heterogeneity can lead to a better performance than homogeneity in terms of considering all relevant aspects of the topic.11 Furthermore, it has been shown that doctors willing to participate in an expert panel are representative for their colleagues.12
To avoid an imprecise definition for consensus, the experts discussed the cut-off point for consensus and decided in Delphi-I that consensus would be defined as ⩾70% agreement. To maintain rigour when using the Delphi method, a 70% minimum response rate should be achieved.13 We were privileged with high response rates in all three Delphi rounds; an average of 92% (range 87–96%) of the participants returned the questionnaires.
The experts achieved consensus about excluding systemic diseases, such as rheumatic diseases, from CANS and decided to add them as “alert symptoms” on the top of the model. Although osteoarthritis is not a systemic disease, it was included within the group of rheumatic diseases.
Local arthritis (not rheumatoid arthritis) in a joint of the upper extremity is classified as one of the 23 specific disorders. An inflammation of the AC joint is an example of such a local arthritis. In the Delphi consensus strategy, the experts did not discuss “local osteoarthritis in a joint of the upper extremity”. A joint can degenerate as a result of overuse, such as osteoarthritis of the AC joint, as a result of sports such as tennis or swimming. We cannot change the results of the consensus, but we see the absence of this specific disorder as a limitation of our model.
One of the oldest classification systems used is the ICD. The ICD is used in many countries for general epidemiological and many health-management purposes. It is used to classify diseases and other health problems recorded on many types of health and vital records, including death certificates and hospital records. Buchbinder et al14 studied the ICD-9 for soft-tissue disorders of the neck and upper limb; they examined the overall accuracy of identifying soft-tissue disorders of these conditions and studied whether the codes themselves, on an individual basis, accurately reflected the underlying problems as documented in the medical records. They found poor agreement between the diagnostic labels recorded in the medical records and the ICD codes, suggesting that many of the terms are being used interchangeably.
To date, the “RSI” report by the Health Council of the Netherlands15 and the so-called SALTSA report “Criteria document for evaluating the work-relatedness of upper-extremity musculoskeletal disorder”6 were considered the state-of-the-art in the Netherlands. Many professional organisations and researchers used these reports as a starting point to develop their own terminology and classification system. This way, over and over again, new terms and classification systems have been generated; this problem occurs not only in the Netherlands but also in other countries. Use of the CANS model can help solve this problem, but we realise that different implementation projects and strategies will be needed before all professionals accept the model. We have already launched projects to implement the CANS model in daily practice. A national conference on upper-extremity musculoskeletal disorders was organised for researchers, clinicians and paramedical health professionals in which the CANS model was revealed. The results of our study were also presented at other congresses and meetings. The Dutch media were very interested in our work; they published on CANS and reported that consensus was achieved. Nowadays, the CANS model is taught in the professional training and retraining of healthcare professionals. However, despite all our efforts to implement the CANS model, and the fact that the CANS model is already used in practice by many professionals, more time and more projects are needed before the model is fully accepted in the Netherlands.
The factor “work-relatedness” is not mentioned in the CANS model. Ergonomic workloads such as repetitive and forceful motion, work organisational factors and psychosocial work factors have definitely been implied as a cause of CANS. Currently, many experts are of the opinion that a single common pathway that links exposure in the workplace resulting in CANS cannot be identified.16 Work-relatedness is not a decision-making factor for including or excluding patients in the CANS model. The model does more justice to reality, as activities at work as well as activities in daily living, such as housekeeping, sports, hobbies and stress at home, can influence the complaints.
Although few data are available on the validity and repeatability of the diagnostic tests of upper-extremity disorders,5 the expert panel of the Delphi consensus strategy achieved consensus to label 23 diagnoses as specific CANS. We did not develop consensus on the diagnostic criteria for these disorders because the aim of this project was to agree on an “unambiguous language”. However, the results of this study are just a starting point for the use of consensus terminology. The CANS model should be re-evaluated after testing it in clinical practice. Moreover, further development of consensus regarding the diagnostic criteria of all the specific disorders is needed; this will make the CANS model even more practical.
Because the criteria specified for diagnoses of specific disorders vary among different classification systems,4 we recommend (inter)national multidisciplinary cooperation to describe these criteria in which key persons—researchers and paramedical and medical professionals—cooperate.
CONCLUSION
The participants in this Delphi survey achieved multidisciplinary consensus on the terminology and classification of complaints of the arm, neck and/or shoulder and reported their result in the CANS model. Adoption of this model can be the first step towards an unambiguous, multidisciplinary accepted classification system for these conditions. Studies on diagnostic criteria and validation studies for both the classification system and the diagnostic criteria are needed to further refine this work.
Acknowledgments
We thank the following organisations and people for their participation.
Selection participants, Delphi consensus strategy: Dutch College of General Practitioners, Dutch Orthopaedic Society, Royal Dutch Society for Physical Therapy, The Netherlands Society of Occupational Medicine, The Netherlands Society of Physical and Rehabilitation Medicine, The Netherlands Society of Neurology, Dutch Society of Exercise therapists Cesar and Mensendieck, Dutch Society for Rheumatology, Dutch Association of Occupational Therapy and the Dutch Professional Association of Psychologists.
Expert-panel, Delphi consensus strategy: T Appels, P Assendelft, I Bakker, P Barendregt, D van der Beek, S Bierma-Zeinstra, R Brenner, C Broekkamp, J Coene, R Diercks, M van Dijk, W Draijer, J Godtschalk, J van Groenendael, M van Heel, M Heemskerk, E Hendriks, P Houtman, M Jansen, I Janssen, B Kolnaar, S Koning, M de Krom, B Kruik, M van der List, W van der Meij, G Meijer, H Osamulia, J Patijn, V Pigmans, J Plasman, J Rasker, P Rietveld, A Romijnders, J Ruijgrok, R Te Slaa, J Starreveld, J Stenvers, J Tellekamp, A Verhoeven, C Visser, W Wertheim, D Wever, F de Wilde, W Willems.
Their participation in this project does not necessarily mean that they fully agree with the final achieved consensus. The CANS model is the result of a “communis opinio”.
REFERENCES
Footnotes
-
Published Online First 16 October 2006
-
Competing interests: None.