Article Text

Abstract
Objectives: To identify risk factors for new episodes of sick leave due to neck or back pain.
Methods: This prospective study comprised an industrial population of 2187 employees who were followed up at 18 months and 3 years after a comprehensive baseline measurement. The potential risk factors comprised physical and psychosocial work factors, health-related and pain-related characteristics and lifestyle and demographic factors. The response rate at both follow-ups was close to 73%.
Results: At the 18-month follow-up, 151 participants reported at least one episode of sick-listing due to neck or back pain during the previous year. Risk factors assessed at baseline for sick leave due to neck or back pain at the follow-up were blue-collar work, back pain one or several times during the previous year, 1–99 days of cumulative sickness absence during the previous year (all causes except neck or back pain), uncertainty of one’s own working ability in 2 years’ time and the experience of few positive challenges at work. After 3 years, 127 participants reported at least one episode of sick leave due to back or neck pain during the year previous to follow-up. The risk factors for this pain-related sick leave were blue-collar work, several earlier episodes of neck pain, no everyday physical activities during leisure time (cleaning, gardening and so on), lower physical functioning and, for blue-collar workers separately, repetitive work procedures.
Conclusion: The most consistent risk factors for new episodes of sick leave due to neck or back pain found during both the follow-ups were blue-collar work and several earlier episodes of neck or back pain assessed at baseline. Preventive efforts to decrease sick leave due to neck or back pain may include measures to increase the occurrence of positive challenges at work and to minimise repetitive work procedures. An evidence-based secondary prevention of neck and back pain including advice to stay active is also warranted.
- SF-36, short form-36
Statistics from Altmetric.com
Lower back and neck pain have a high prevalence and incidence in adult populations,1 and social expenditure due to these ailments is huge.2 Indirect costs such as sickness absenteeism and disability pensions constitute approximately 90% of this expenditure.3 Well-designed longitudinal studies have been called for to assess factors related to sick leave, including risk factors for being sick-listed.4
A large body of research has been aimed at discerning risk factors for developing neck or back pain and/or chronic disability and several reviews have summarised these findings. On the whole, it seems that the physical load at work—for example, manual material handling, bending and twisting and whole-body vibrations—increases the risk for back pain.5,6 With regard to psychosocial factors in the workplace, some authors have concluded that, among other things, low job satisfaction and low social support7,8 are related to the onset of back pain; whereas other researchers have found moderate evidence for no relation between back pain and psychosocial factors at work.9 Furthermore, psychological factors such as distress and depressed mood have been related to new episodes of neck or back pain10 and subsequent chronicity or disability.11 Regarding life-style factors, some evidence indicates that smoking may be related to back pain12,13 even though this has not been confirmed in all studies.14 Physical activity, or inactivity, during leisure time has not been consistently related to the occurrence of back pain.5,15
Most people will experience one or more episode(s) of neck or back pain during their lives,1 but only a small proportion will seek help and/or become sick-listed because of these complaints.16,17 Therefore, it seems reasonable to assume that sick leave due to neck or back pain is predicted by different factors other than those predicting the onset of neck or back pain.14,18
A number of studies have examined factors related to future sick leave due to neck or back pain; however, in a recent systematic review it was concluded that there is only limited evidence that certain work-related characteristics, together with a few medical/functional factors and some demographic factors, are risk factors for future sick-listing due to back or neck pain.19 Physical and/or ergonomic factors such as troublesome working postures and/or heavy lifting have been reported in some studies to increase the risk of future sick leave due to neck or back pain,14,20–23 but they were not related to sick-listing in other studies.24–26 Psychosocial factors in the work environment have also emerged as predictors of sick listing. These include low job satisfaction,23,24,26 low control over work and a low work pace among men27; low decision-making authority and medium skill discretion20 and low coworker support.14,26 However, in a study by Elders et al,21 psychosocial work characteristics were not related to sickness absence due to back pain.
Factors such as pain intensity,21,22 reports of earlier episodes of back pain,22,27 results from the straight-leg-raising test and medical history,24 sick-listing in general,28 demographics/background such as age,29 employment grade,27 working night shifts22 and a few others such as emotional distress or low mood,24,30 disability26 and heavy smoking14 have also predicted sick-listing attributed to back pain. However, divergent results have been found in other studies—for example, age, earlier back pain and smoking were not found to predict sick leave due to back pain in a study by Burdorf et al.31
A better knowledge of factors related to future sick leave attributable to neck or back pain could be instrumental in decision-making regarding preventive measures aimed at reducing sickness absence due to these conditions. The aim of this prospective study was to identify factors that predict new episodes of sick leave attributed to neck or back pain in an occupational population.
METHODS
This prospective study is based on material gathered during a larger study, “Work and Health in the Processing and Engineering Industries, the AHA Study”.32 Four workplaces in Sweden participated in the study. Two of those were paper mills including occupations such as operators, technicians, laboratory workers and repairmen; one was a truck manufacturer comprising job titles such as assemblers, mechanics, painters and truck drivers and one was a steelworks including occupations such as material handlers, tube workers, repairmen and material preparers. Data were gathered from the year 2000 to 2003. The baseline measurement was carried out in 2000, and the follow-up measurements were performed 18 months and 3 years thereafter.
Study population
All individuals employed at the time of the baseline measurement constituted the source population in this study. The baseline questionnaire was sent to 4160 employees (3679 men; 481 women) and 2894 (69.6%; 2523 men and 371 women) responded. Because register data were available for the entire source population, a comparison of a few variables between responders and non-responders at baseline was possible. The responders were, on average, older than non-responders (41.9 (SD 10.9) years vs 37.2 (10.9) years), the proportion of women was somewhat larger among responders than among non-responders (12.8% vs 8.7%), the proportion of white-collar workers was larger among responders than among non-responders (21.6% vs 6.3%) and the proportion of daytime workers was larger among responders than among non-responders (60.7% vs 54.5%).
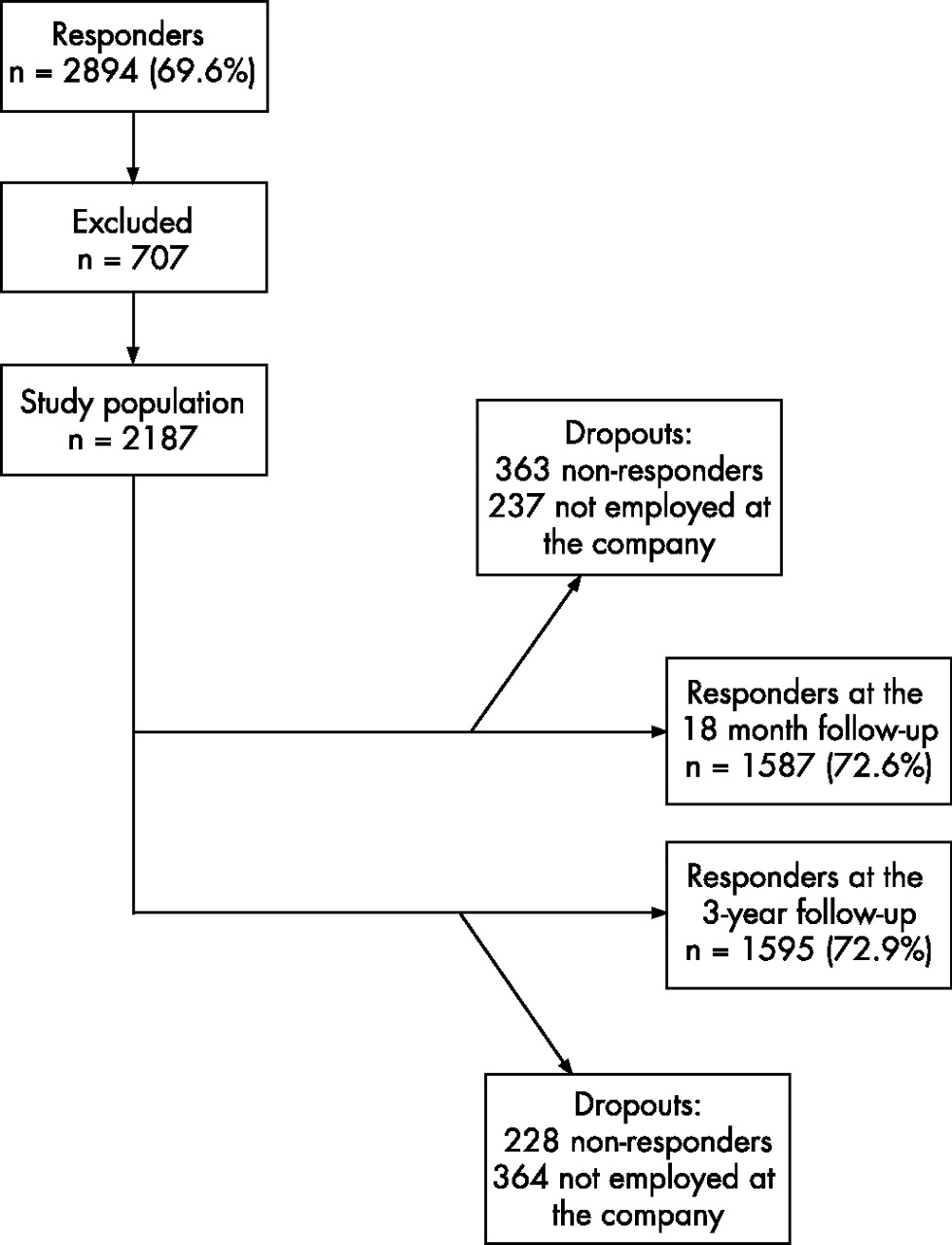
The inclusion criteria in this study were: (1) complete data on prevalence of, and sick leave due to, neck or back pain during the year previous to baseline; (2) no sick leave due to back or neck pain during the year previous to baseline; (3) working at least 20 h per week and (4) having been in the current work position for at least 1 year. Figure 1 shows the flow chart of the study. After excluding 707 subjects, the eligible study population was 2187. Nearly 90% of the participants were men and approximately a third reported no neck or back pain during the year previous to the baseline (table 1).
Descriptive information on the study population (n = 2187)
{kind=link}
Flow chart of the study. Reasons for exclusion: sick leave due to neck or back pain the year previous to baseline (n = 422); missing information on prevalence of, or sick leave due to, neck or back pain the year previous to baseline (n = 92); working less than 20 h/week or having been in the current work position less than 1 year (n = 193).
Measurement at baseline of potential risk factors
The companies’ registers were used for information on the participants’ sex, age and employment grade. All other data were self-reported. Primarily, questionnaires that have shown acceptable reliability and validity in Swedish populations were chosen.
Data regarding demographic/background information included age, sex, education, immigration status, marital status, number of children living at home, employment grade (white-collar/blue-collar) and work schedule (daytime/shift work).
Health-related variables and pain characteristics were assessed using eight scales from the short form-36 (SF-36),34,35 the Hospital Anxiety and Depression Scale,36,37 exhaustion from the Maslach Burnout Inventory–General Survey,38 body mass index39 and four items from the Work Ability Index.40 Disability due to back or neck pain was assessed using the three 0–10 interference ratings included in the Graded Chronic Pain Scale41 and the prevalence of neck and back pain during the previous year was measured by two items (one for neck pain and one for back pain) formulated as follows: “Have you been troubled by back (neck) pain during the past year?” The response alternatives were: “no”, “yes, one time” and “yes, several times”.
Lifestyle factors comprised smoking,42 hazardous alcohol consumption33 and four items on exercise habits.43 Three of the items on exercise habits considered deliberate exercise at three different levels of exertion: “How often do you exercise at a high (medium, low) level of exertion?” The response alternatives were “never”, “irregularly”, “1 time per week”, “2 times per week” and “3 times per week or more”. The fourth item considered everyday physical activities formulated as: “How physically active are you except regarding paid work and exercise (eg, cleaning, gardening, cycling to work etc.)?” The response alternatives were “almost no physical activities”, “less than 30 minutes per day”, “1–2 hours per day” and “3 hours or more per day”.
Psychosocial factors in the workplace were assessed using the General Nordic Questionnaire for Psychological and Social Factors at Work (QPSNordic).44 The following indexes (range 1–5) were used: support from superior; support from coworkers; quantitative work demands; decision demands; learning demands; role conflicts; role clarity; control of decisions; control of work pace; positive challenges at work; fair leadership; empowering leadership; mastery of work; social climate; predictability of work (in the next 2 years) and commitment to the organisation. Single items were used to measure repetitive work (“Do you have to repeat the same work procedure at intervals of a few minutes?”), bullying and harassment at work (“Have you been subjected to bullying or harassment at the workplace during the last six months?”) and work centrality (“How important and significant is working in your life as a whole?”).
The physical load at work was assessed by single items pertaining to the frequency of heavy lifting, working with hands above the shoulders, proportion of the day exposed to whole-body vibrations, proportion of the days working with hand-held vibrating tools45 and perceived exertion at work.46
Measurement of the outcome (dependent) variable
Sick leave attributed to neck or back pain was assessed at the two follow-ups using the following items: (1) “Have you been sick-listed due to neck or back pain during the past year?” and (2) “Are you sick-listed right now because of neck or back pain?” These two items were merged into one dichotomous variable indicating sick-listing (ongoing or sick-listed during the previous year) or no sick-listing, which constituted the dependent variable in the following analyses. No distinction was made between neck and back pain, as medical factors seem to have limited explanatory power for variation in sick leave due to neck or back pain.19
Ethics
All ethical considerations regarding the study were approved by the Committee on Ethics of the Karolinska Institute, Stockholm, Sweden.
Statistical analyses
Logistic regression47 was used to analyse the data using SPSS V.13.0 for Windows. Indexes were divided into quartiles before entry in the logistic regression. The independent variables were divided into five different variable sets: demographic/background factors; lifestyle factors; health-related and pain-related variables; physical factors at work; and psychosocial work factors. The analyses were carried out in three steps: (1) each independent variable was analysed using a univariate logistic regression; during this procedure the odds ratios (ORs) were scrutinised and, in cases where the ORs from ⩾2 adjacent categories lay within ±10% of the mean OR for the categories in question, they were merged. Thereafter, all variables with a p value ⩽0.10 were analysed by (2) stepwise multiple logistic regressions for each of the five variable sets. Before these multivariate analyses, collinearity was checked for by calculating correlation coefficients (Spearman’s ρ) for the independent variables, and variables with a pairwise correlation >0.5 were examined and the one with the weakest univariate OR (see step 1) was removed. In the multiple logistic regressions, the p value for entry in the model (PIN) was p = 0.15 and the p level for removal from the model (POUT) was p = 0.20. Eventually, (3) a final multiple logistic regression was used in which all variables from the analyses in step 2 with p<0.10 were entered. In these analyses PIN = 0.05 and POUT = 0.10 were applied to reach a more restrictive final model. Age, sex and neck or back pain at baseline were regarded as a priori predictors and were entered in all multivariate analyses. To be defined as a risk factor in this study (and presented in the forthcoming tables), a variable should have a significance level of <0.05 in the multivariate analyses.
Dropouts
As depicted in fig 1, 72.6% (n = 1587) of the study population answered the 18-month follow-up questionnaire and 72.9% (n = 1595) responded at the 3-year follow-up. Based on baseline data, the dropouts were slightly younger than the responders both at the 18-months follow-up (mean (SD) age 40.4 (11.6) years vs 43.5 (10.3) years) and at the 3-year follow-up (41.8 (12.1) years vs 43.0 (10.2) years), the sex distribution was relatively similar between dropouts and responders both at the 18-month follow-up (dropouts 13.3% women vs responders 11.6% women) and the 3-year follow-up (13.7% vs 11.5%) and the proportion among dropouts and responders reporting neck or back pain at baseline was approximately the same (18-month follow-up, 60% among dropouts vs 63.3% among responders; 3-year follow-up, 60.5% vs 63.1%).
RESULTS
Among the 1587 responders at the 18-month follow-up, 151 participants (9.5%) reported at least one episode of sick-listing due to back or neck pain during the previous year. In this group, 21 (13.9%) individuals did not report any previous or present neck or back pain at the baseline measurement, 63 (41.7%) reported neck or back pain during the year previous to baseline and 67 (44.4%) reported both previous and present neck or back pain at baseline.
Among the 1595 responders at the 3-year follow-up, 127 (8%) individuals reported at least one episode of sick-listing due to back or neck pain during the past year. In this group, 25 (19.7%) participants did not report any previous or present neck or back pain at baseline, 42 (33.1%) had experienced neck or back pain during the year before baseline and 60 (47.2%) reported both previous and present neck or back pain at baseline.
Predictors at the 18-month follow-up
Table 2 gives the adjusted ORs from the multiple logistic regressions per variable set. In the final multiple logistic regression (table 3), risk factors assessed at baseline for sick leave due to neck or back pain at the 18-month follow-up were blue-collar work, back pain once or several times during the previous year, cumulative sickness absence (all causes except neck or back pain) of 1–99 days during the previous year, being uncertain of one’s own working ability in 2 years’ time and the experience of few positive challenges at work. None of the variables concerning the physical work environment or lifestyle factors was significantly related to sick leave attributed to neck or back pain.
Factors assessed at baseline related to sick leave due to neck or back pain at the 18-month follow-up
Risk factors assessed at baseline predicting sick leave because of neck or back pain at the 18-month follow-up
The final multiple logistic regression (including all the variables described in table 3) was also carried out for blue-collar workers separately, and rendered the same risk factors as for the total group except for “perceived prognosis of own working ability in 2 years’ time”. Because of the small number of cases of sick leave due to neck or back pain among white-collar workers (n = 17) and the subsequent risk of large CIs and instability in the model, no further analyses were performed for this group.
Predictors at the 3-year follow-up
Table 4 gives the adjusted ORs from the multiple logistic regressions per variable set. In the final multiple logistic regression (table 5), risk factors assessed at baseline for sick leave attributed to neck or back pain at the 3-year follow-up were blue-collar work, no everyday physical activities during leisure time (cleaning, gardening, etc), having had neck pain at several times during the previous year and having ⩽90 points on the physical functioning scale of the SF-36. Decision demands at work were also included in the model, but when the categories reflecting higher demands were compared to the reference category with the lowest demands one by one, the CIs did not exclude unity. As can be seen, no clear dose–response gradient is visible for decision demands. Again, none of the variables concerning the physical work environment were independent risk factors.
Factors assessed at baseline related to sick leave due to neck or back pain at the 3-year follow-up
Risk factors assessed at baseline predicting sick leave because of neck or back pain at the 3-year follow-up
The final multiple logistic regression was also carried out for blue-collar workers only. This analysis rendered the same risk factors as for the total group except that decision demands were left out and repetitive work was included in the final model. Blue-collar workers reporting that they often or always had to repeat the same work procedure at intervals of a few minutes had an increased risk of sick leave due to neck or back pain, OR 1.78 (95% CI 1.13 to 2.81), compared with workers who seldom or never had to do so.
Ex post facto analyses were used for the variable “perceived prognosis of one’s own working ability in 2 years’ time”, because a low level of belief in future working ability may indicate an increased risk of being among the “not employed” (dropouts) at both the follow-ups. These analyses showed that employees reporting that they would “probably not” be able to work in 2 years’ time had a higher risk of being in the “not employed” group at the follow-ups compared with those marking the “almost certain” alternative (reference category) of the item. At the 18-month follow-up the OR for the “probably not” category was 4.38 (95% CI 2.02 to 9.49) and at the 3-year follow-up the OR was 4.20 (95% CI 2.02 to 8.75). Employees marking the category “not certain about it” at baseline also had a heightened risk of being among the not employed at the 3-year follow-up (OR 1.82; 95% CI 1.25 to 2.65) but not at the 18-month follow-up (OR 1.32; 95% CI 0.81 to 2.13).
DISCUSSION
This prospective study strengthens the evidence regarding factors related to new episodes of sick leave attributable to neck or back pain. The most consistent risk factors found at both the 18-month and 3-year follow-ups were blue-collar work and several earlier episodes of neck or back pain assessed at baseline. Furthermore, a cumulative sick leave of 1–99 days for reasons other than neck or back pain during the year previous to baseline, uncertainty about future working ability and the experience of few positive challenges at work emerged as risk factors at the 18-month follow-up. At the 3-year follow-up, no everyday physical activities in leisure-time (riding a bicycle to work, taking a short walk and so on) and figures ⩽90 points on the physical functioning scale of the SF-36 predicted sick leave due to neck or back pain and, for blue-collar workers, repetitive work also emerged as a predictor. Although a number of seemingly pertinent variables concerning the physical work environment were included in the analyses, they failed to predict future sick leave due to neck or back pain in the final multivariate model. The generalisability of the study applies primarily to male-dominated industrial settings and to similar types of insurance systems.48
In this study, pain disability did not independently emerge as a predictor, nor did pain severity according to the SF-36. This is at variance with some earlier studies regarding both pain disability26,49 and pain intensity21,22 and may depend on different characteristics of the study populations or the use of different measurement methods.
To the best of the authors’ knowledge, only one earlier study concerned with risk factors for sick leave due to neck or back pain has used the QPSNordic for measuring the psychosocial work environment.22 Therefore, a closer look at the risk factor “positive challenges at work” that emerged could be appropriate. According to the developers of the instrument,44 this variable reflects job control and is somewhat similar to job discretion in the demand–control model.50 The three items in the scale deal with the question of whether the work is perceived as being meaningful or challenging in a positive way and whether the employees’ skills and knowledge are useful at work. In Eriksen et al’s study,22 positive challenges in the workplace did not emerge as a predictor of sick leave due to back pain. More studies are needed on the predictive power of this variable as well as an the use of QPSNordic in general for such predictive purposes as in this report.
The employees with the highest decision demands reported a lower risk of sick leave due to neck or back pain compared with employees with the lowest demands in the univariate analysis, but this result became non-significant when other health, lifestyle and work characteristics were controlled for. Furthermore, no dose–response relation was seen for this variable. A similar result was found by Eriksen et al22 regarding quantitative work demands and may indicate the presence of a healthy-worker effect, which, among other things, implies that jobs with high demands may be avoided by workers perceiving poor health. Although high decision demands also, to some degree, may be related to positively challenging jobs, as discussed above, this may also partially explain the finding that a large degree of decision demands were protective against sick leave due to neck or back pain in the univariate analysis.
At the 18-month follow-up, a cumulative sickness absence (all causes except neck or back pain) 1–99 days the year before baseline was a risk factor for sick leave attributable to neck or back pain and the same variable also showed some predictive ability at the 3-year follow-up in the multivariate analysis of health characteristics. This finding may reflect the fact that different forms of employment are more or less demanding and/or flexible, and thereby also more or less taxing to carry out with impaired health regardless of the type of complaint. However, as several work-related variables were controlled for, the finding may also imply that certain employees are more inclined to use sick leave as a coping strategy irrespective of the type of symptoms. Among the health-related characteristics, uncertainty about one’s own working ability in 2 years’ time was also predictive of sick leave due to neck or back pain at the 18-month follow-up. This variable is, however, troublesome to interpret as the risk of being in the not-employed group was increased at both follow-ups for employees with a low level of belief in their working ability in 2 years’ time and, consequently, they could not be included in the analyses. This means that a potential increased risk of future sick leave due to neck or back pain for these employees may not be detected and it may also explain the lack of a dose–response gradient for this factor at the 18-month follow-up.
A result of⩽90 points at the 3-year follow-up on the physical functioning scale of the SF-36 and no everyday physical activities during leisure time seemed to be risk factors for sick leave due to neck or back pain. Physical functioning can be regarded as being inversely related to disability, although not necessarily pain-related disability, and, to the authors’ knowledge, this type of life-quality measurement has not been used earlier in prospective studies on sick leave due to neck and back pain. It should be noted that this category became very wide due to the distribution of the scale scores and that the risk of future sick leave probably varies considerably within this category. Considering the role of no everyday physical activities in leisure time (eg, cleaning and gardening), this may indicate that a prolonged sedentary lifestyle heightens the risk of sick leave due to neck or back pain. Physical leisure-time activities have been reported earlier to reduce the risk of long-term sick leave,51 and a sedentary lifestyle has been related to sick leave due to lower back pain52 even though the connection to back pain in itself is unclear.5,15
None of the physical work factors were predictive of future sick leave attributable to neck or back pain when variables from other areas (datasets) were taken into account. As described in the introduction, earlier research has not been consistent regarding whether physical work factors predict future sick leave due to neck or back pain. Nevertheless, because several studies have found a relationship between physical work factors and neck or back pain,53–55 the results of this study suggest that physical work factors may be more important in explaining the occurrence of neck or back pain than episodes of sick leave due to these conditions.
Some implications of this study are that measures at the workplace to reduce sick leave due to neck or back pain in similar populations may be directed primarily at blue-collar workers and include efforts to make the work more meaningful and positively challenging and to reduce repetitive work procedures. As earlier neck and back pain both seemed to be risk factors, evidence-based strategies, including advice to stay active,56 for the secondary prevention of neck and back pain may also be necessary to reduce sick leave due to these complaints.
This study used self-reported data as both independent variables (potential predictors) and the dependent variable (outcome), which could have led to the risks being overestimated due to correlation between the methods used for assessment. Self-reported data may also mean that the accuracy regarding the measurement of, for instance, the physical workload is limited.
Moreover, the choice of cut-off points when dividing a variable into one reference category and one or more exposure categories may be crucial. In this study, some variables were categorised, for instance, according to quartiles, and a different method of categorisation may have led to a different end result. A further consideration is that no distinction was made between neck and back pain in the study due to the limited ability of medical variables to predict sick leave due to neck or back pain.19 However, the scientific knowledge is considerably better for back pain than for neck pain, for example, regarding diagnosis and treatment,1 and there may be differences between these conditions concerning risk factors both for the occurrence of complaints and for any subsequent sick leave.
In summary, this prospective study suggests that risk factors for new episodes of sick leave due to neck or back pain in a male-dominated industrial setting were several earlier episodes of neck or back pain, few positive challenges at work, cumulative sick leave of 1–99 days the year before baseline (all causes except neck or back pain), uncertainty about one’s own working ability in 2 years’ time, no everyday physical activities during leisure time (eg, cleaning or gardening) and, for blue-collar workers, repetitive work procedures. Blue-collar workers had an increased risk for sick leave due to neck or back pain compared with white-collar workers. Some practical implications of the study are that, in similar populations, preventive efforts in the workplace may be focused primarily on blue-collar workers and include measures to increase the occurrence of positive challenges in the workplace and to design work so as to minimise the occurrence of repetitive work procedures. An evidence-based secondary prevention of neck and back pain including advice to stay active is also warranted. Furthermore, research is needed among white-collar workers and women for predictors of future sick leave due to neck or back pain because these groups are often under-represented in this type of research.
Main messages
-
In this prospective study, risk factors for new episodes of sick leave due to neck or back pain in a male-dominated industrial setting were several earlier episodes of neck or back pain, few positive challenges at work, cumulative sick leave of 1–99 days the year previous to baseline (all causes except neck or back pain), uncertainty about one’s own working ability in 2 years’ time, no everyday physical activities during leisure time (eg, cleaning or gardening) and, for blue-collar workers, repetitive work procedures. Blue-collar workers had an increased risk for sick leave due to neck or back pain compared with white-collar workers.
Policy implications
-
Preventive efforts in male-dominated industrial settings may be focused primarily on blue-collar workers, and include measures to increase the occurrences of positive challenges in the workplace and to design the work so as to minimise the occurrence of repetitive procedures.
-
Evidence–based secondary prevention of neck and back pain including advice to stay active is also warranted.
Acknowledgments
We are grateful to the research and project groups in the AHA study who have been indispensable in the completion of the study. We also thank Mr Isaac Austin for his revision of the English in the manuscript. We acknowledge the financial support of AFA-sjukförsäkring, Stockholm, Sweden.
REFERENCES
Footnotes
-
Published Online First 9 November 2006
-
Competing interests: None declared.