Article Text

Abstract
Objectives: To develop a concise screening instrument for early identification of employees at risk for sickness absence due to psychosocial health complaints.
Methods: Data from the Maastricht Cohort Study on “Fatigue at Work” were used to identify items to be associated with an increased risk of sickness absence. The analytical procedures univariate logistic regression, backward stepwise linear regression, and multiple logistic regression were successively applied. For both men and women, sum scores were calculated, and sensitivity and specificity rates of different cut-off points on the screening instrument were defined.
Results: In women, results suggested that feeling depressed, having a burnout, being tired, being less interested in work, experiencing obligatory change in working days, and living alone, were strong predictors of sickness absence due to psychosocial health complaints. In men, statistically significant predictors were having a history of sickness absence, compulsive thinking, being mentally fatigued, finding it hard to relax, lack of supervisor support, and having no hobbies. A potential cut-off point of 10 on the screening instrument resulted in a sensitivity score of 41.7% for women and 38.9% for men, and a specificity score of 91.3% for women and 90.6% for men.
Conclusions: This study shows that it is possible to identify predictive factors for sickness absence and to develop an instrument for early identification of employees at risk for sickness absence. The results of this study increase the possibility for both employers and policymakers to implement interventions directed at the prevention of sickness absence.
- screening instrument
- prediction
- sickness absence
Statistics from Altmetric.com
In many countries throughout the Western world, psychosocial health complaints, such as depression, fatigue, stress, and work family conflicts, represent important causes of sickness absence and disability.1,2 Once at home on sick leave due to these complaints, employees encounter difficulties in returning back into the workplace.3 A better and more effective strategy would be early identification of employees at risk for sickness absence. For this reason, it is imperative to recognise predictive factors in order to screen employees, and subsequently to prevent sickness absence as much as possible through early intervention.4
Numerous epidemiological studies have investigated factors such as sociodemographic factors, health and mental health, psychosocial work factors, personal factors, and organisational factors, to be predictive of sickness absence.5 The most consistent results within sociodemographic factors have been reported for age, which tends to be negatively related to sickness absence, and for gender—women have a higher rate of absence and more days of absenteeism than men. With regard to health and mental health factors, increased risks have been found for psychosomatic complaints, medication use, burnout, and psychological problems for sickness absence. Studies examining the relation between psychosocial work factors and sickness absence have found that sickness absence is related to low job control and low decision latitude, and that there is evidence relating to aspects such as psychological job demands, job strain, job satisfaction, and need for recovery. Studies that address the effect of personal factors on sickness absence suggest that stressful events in one’s private life may relate to ill health, and thus to sickness absence. With regard to organisational factors, epidemiological studies predominantly report the consequences of prior absence on future sickness absence.5
Taking these predictive factors into consideration, there are a number of options for looking at the management and prevention of sickness absence, which can be termed as primary, secondary, and tertiary levels of intervention.6 Primary interventions focus on prevention among people who are not immediately at risk for sickness absence; secondary interventions focus on people who are suspected to be at risk for sickness absence or who are already frequently on sick leave; and tertiary interventions focus on those who are on sick leave, to prevent further deterioration of their wellbeing.7 From a public and preventive medicine perspective, primary prevention is generally regarded as the ideal point of intervention,8 with the exception of circumstances in which primary prevention is not possible or individual factors create health concerns for only some people.9 When clearly identifiable predictive factors are present, preference may be given to individual interventions with a secondary preventive emphasis.10 However, to bring secondary preventive measures within the occupational health field into practice, the combination of these identified predictive factors in a screening instrument would be usable. Regardless of the numerous studies into particular predictive factors of sickness absence, only a few studies investigated the association between a range of predictive factors and sickness absence, but no study combined them in a screening instrument for early identification.
The objectives of this study were to identify a set of predictive factors, using data from the Maastricht Cohort Study on “Fatigue at Work”, to develop a concise screening instrument for early identification of employees at risk for sickness absence due to psychosocial health complaints, and to test its basic measures.
METHODS
Maastricht Cohort Study
The Maastricht Cohort Study on “Fatigue at Work” is a prospective study on a sample of 12 140 workers, employed by 45 different organisations, mostly located in the southern part of the Netherlands.11,12 The heterogeneous group of employees represented a variety of jobs and educational levels, and a range of economic sectors and trades. Included were employees between the ages of 18 and 65 years (mean age 41.0 years). At baseline, 73.1% of the study population were men, 17.6% were government employees, 15.0% were employees from healthcare institutes, 50.4% of the employees worked in industry, and 17.0% were in services. The cohort study started in May 1998 and covers a period of three years, in which the participants received several self-administered questionnaires.13 The primary goal of the Maastricht Cohort Study was to identify risk factors involved in the aetiology and natural course of prolonged fatigue in the working population and to develop preventive measures and treatments, that can be used in occupational health settings.14
Study population
For development of the screening instrument, we have used data from the Maastricht Cohort Study on employees who have completed and returned both the self-administered baseline questionnaire in May 1998 and the extensive one year follow up questionnaire in May 1999. This resulted in data on 9655 workers. Employees were excluded from participation if they were fully or partially on sick leave (n = 592), because of the potentially biased perception of the work situation of sick listed employees15,16 and because of the secondary preventive emphasis of this study. Secondly, employees who reported suffering from chronic psychosocial health complaints at baseline (n = 279) were excluded. Including these employees would subvert the underlying principle of focusing on healthy employees who are “at risk” for future sickness absence due to psychosocial health complaints. Thirdly, employees with more than one contract (n = 385) were excluded. The need or the motivation to report sick in one job may lead to the systematic actual initiation of sickness absence in the other job.17 Finally, women who were pregnant or on maternity leave (n = 188) were excluded from participation. After application of these exclusion criteria, 8211 cohort participants were available for analysis.
For validation of the screening instrument, we used data from employees who completed and returned both the one year follow up questionnaire in May 1999 and the extensive two year follow up questionnaire in May 2000 (n = 7975). After applying the above exclusion criteria, data on 6780 employees were found to be suitable for analysis. The employees who responded to the questionnaires used for development of the screening instrument did not differ in gender, age distribution, and educational level from the employees who responded to the questionnaires used for validation of the screening instrument.
Measures
Sociodemographic and health related factors
Sociodemographic factors include age, sex, educational level, and variables concerning the private and financial situation, such as living conditions, care for children, leisure activities, and home help. The several questionnaires of the Maastricht Cohort Study also included questions about the presence of long term diseases, such as heart problems, stroke, cancer, diabetes, musculoskeletal problems, and chronic psychosocial problems. Self-rated health was assessed with one item from the Short Form Health Survey (SF-36),18 which is a widely used measure of general health status.19 The general health status item was scored on a five point scale (1 = excellent health, 2 = very good health, 3 = good health, 4 = moderate health, 5 = bad health).
Mental health factors
Fatigue was assessed with the 20 item self-reported Checklist Individual Strength (CIS).20,21 The CIS covers several aspects of fatigue, such as severity (eight items), concentration (five items), motivation (four items), and physical activity (three items). The response on each item is scored on a seven point Likert scale (1 = yes, that is true to 7 = no, that is not true). Higher scores on these subscales indicate a higher degree of fatigue, more concentration problems, reduced motivation, or a lower level of physical activity. Burnout was assessed with the three subscales of the Dutch version of the Maslach Burnout Inventory–General Survey (MBI-GS):22,23 exhaustion (five items), cynicism (five items), and professional efficacy (six items). All items are scored on a seven point frequency scale, ranging from 0 (never) to 6 (daily). High scores of exhaustion and cynicism and low scores on professional efficacy are indicative for burnout. Need for recovery was measured with a scale, derived from the Dutch Questionnaire on the Perception and Judgment of Work (VBBA).24,25 The scale contains 11 dichotomous items, concerning the recuperation period after one day of work, for example “it is difficult for me to relax at the end of a work day”. Higher scores on this scale indicate more complaints, i.e. a higher need for recovery. Furthermore, participants were asked to indicate if they had suffered from fatigue complaints in the preceding four months (yes or no), and if so, whether they felt that the cause of these complaints was psychological (yes or no), somatic (yes or no), or of an unknown nature (yes or no). Psychological distress was assessed with a Dutch version of the 12 item General Health Questionnaire (GHQ-12).26,27 The GHQ-12 was developed as a screening instrument for detecting minor psychiatric disorders and contains items such as “unhappy and depressed” and “losing confidence in self”. A higher score on this four point scale indicates a higher level of psychological distress. Anxious mood was assessed with three items on anxiety: excessive worrying, compulsive behaviour, and compulsive thinking. A higher score indicates a higher level of anxious mood.28
Psychosocial work factors and organisational factors
Psychosocial work characteristics were measured with five subscales of a validated Dutch version of the Job Content Questionnaire (JCQ):29,30 psychological job demands (five items), skill discretion (six items), decision authority (three items), co-worker social support (four items), and supervisor social support (four items). The response options for each item varied on a four point scale from “strongly disagree” to “strongly agree”. Participants were also asked to indicate whether they experienced conflicts with colleagues (yes or no) or conflicts with supervisors (yes or no). Additional data on organisational characteristics, such as “working hours”, and perception of work, such as “commitment”, “job satisfaction”, “job security”, “physical and emotional demands”, “effort–reward imbalance”, and “role ambiguity”, were gathered with the Dutch Questionnaire on the Perception and Judgment of Work (VBBA).24,25
Sickness absence
Data on sickness absence due to psychosocial health complaints were inventoried in the two extensive follow up questionnaires (May 1999 and May 2000). In both questionnaires, participants were asked to report the frequency of sickness absence in the previous four months, given the six possibilities: (1) never, (2) one time, (3) two times, (4) three times, (5) four times, (6) five times or more. In case of at least one ill report, they were asked to give information about the reason for their latest sick leave. A code has been allotted, in accordance with the International Classification of Primary Care (ICPC), to the reasons employees have given for their latest sickness absence. The following ICPC codes were used to identify employees who reported sick as a result of psychosocial health complaints: A04, P01–P26, P76, P78, Z01–Z29. Both short term and long term absence spells were included. Frequency and duration of self-reported sickness absence data were compared with available objective sickness absence data from company records to preclude self-report bias.31 Within these objective sickness absence data, no reasons or diagnoses for sick leave were present.
Statistical analysis
All analyses were performed separately for men and women, since females are more susceptible to sickness absence than men.32–36 Employees who reported sickness absence due to psychosocial health complaints were compared with employees who did not report this form of sickness absence. Firstly, logistic regression analysis was used to examine the effect of each particular item at baseline on sickness absence after one year. All significant items in these univariate analyses (χ2 test; p < 0.05), complemented by a set of substantive variables as listed in literature, were selected. Secondly, backward stepwise linear regression analysis (p < 0.10) was used to further reduce items to be associated with a higher risk of sickness absence. Thirdly, multiple logistic regression analysis was conducted to determine unstandardised regression coefficients and their standard errors. Fourthly, sum scores of individual employees were computed by multiplying and adding up the unstandardised regression coefficients with the scores on the significant items. Finally, a receiver operator characteristic (ROC) analysis was performed to define both sensitivity and specificity, and to determine the screening instruments’ most adequate cut-off point for sickness absence. The last two steps of the development of the screening instrument were repeated in order to achieve internal validation of the instrument. All statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS), version 11.0.37
RESULTS
Selection step 1
Univariate logistic regression analyses were used for the first selection of baseline items, with an effect on sickness absence due to psychosocial health complaints after one year. The analyses resulted in an extensive list for both men and women. The most important statistically significant factors were related to “health”, “mental health”, and “psychosocial work characteristics”. For both men and women, the list was complemented by a set of substantive items, such as factors concerning the “private situation” (data not shown).
Selection step 2
Backward stepwise linear regression analysis was used as second selection step for the reduction of items to be associated with a higher risk of sickness absence. The statistical analysis resulted in a final enumeration of items, for both men and women, associated with sickness absence due to psychosocial health complaints. Table 1 shows the relation between these specific predictive factors and the incidence proportion of sickness absence, as well as a presentation of corresponding odds ratios. In women, the following were strong predictors of sickness absence due to psychosocial health complaints: general health factors, such as feeling unhappy and depressed (GHQ-12); mental health factors, such as having a burnout; being tired when facing another day and being less interested in work (MBI-GS); work related factors, such as going through an obligatory change in working days and experiencing conflicts with colleagues (VBBA); and factors concerning their private situation, such as living alone. In men, the following were significant predictors: general health factors, such as having a history of sickness absence; mental health factors, such as compulsive thinking, being mentally fatigued, and finding it hard to relax at the end of a working day (VBBA); work related factors, such as lack of supervisor support (JCQ); and factors concerning their private situation, such as having no hobbies (table 1).
Odds ratios (OR) and incidence proportion (I) of identified predictive factors and sickness absence due to psychosocial health complaints
Selection steps 3 and 4
Multiple logistic regression analysis was used as third selection step to determine the unstandardised regression coefficients (B) and their corresponding standard errors (SE B) of the identified items. Subsequently, sum scores were computed for both men (range −7.69 to 0.40) and women (range −6.11 to 0.01) by multiplying and adding up the unstandardised regression coefficients with the scores on the significant items.
Selection step 5
The ability of the screening instrument to identify employees with or without self-reported sickness absence due to psychosocial health complaints was assessed by calculating sensitivity and specificity rates, and their corresponding confidence intervals, of different cut-off points (table 2).
Cut-off points (CP), and sensitivity and specificity rates (%) for development and validation of the screening instrument
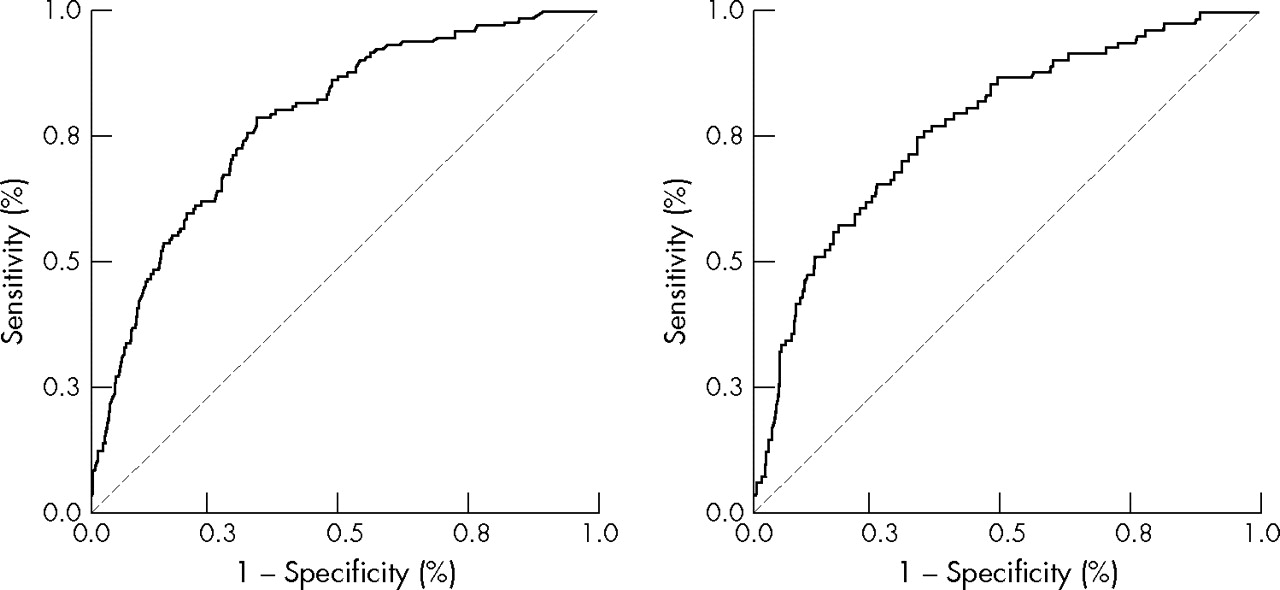
Receiver operator characteristic (ROC) analyses were performed, for both men and women, to define the screening instruments’ most adequate cut-off point for sickness absence. For example, a cut-off point of 10 on the screening instrument resulted in a sensitivity score of 41.7% for women and 38.9% for men, and a specificity score of 91.3% for women and 90.6% for men. The area under the curve was 0.775 for women (p < 0.001) and 0.780 for men (p < 0.001) (fig 1).
{kind=link}
Receiver operator characteristic curves for men (left) and women (right) of the developed screening instrument.
Validation of steps 1 and 2
The developed screening instrument was used to predict which employees, in May 1999, were “at risk” for sickness absence in May 2000. Sum scores were calculated and, by means of the determined cut-off points on the developed screening instrument, sensitivity and specificity scores were estimated. For example, a cut-off point of 10 resulted in a sensitivity score of 10.8% for women and 17.6% for men, and a specificity score of 92.8% for women and 92.4% for men (table 2).
DISCUSSION
General findings
This study represents the development of a screening instrument for the prediction of sickness absence due to psychosocial health complaints. The selection of a range of predictive factors to screen employees, in order to prevent sickness absence due to psychosocial health complaints, has not been done before. For both men and women, 17 predictive items were extracted from several questionnaires used in the Maastricht Cohort Study, all known for their reliability and unidimensionality. In women, the main results suggest that feeling depressed, having a burnout, being tired, being less interested in work, experiencing an obligatory change in working days, and living alone, were strong predictors of sickness absence due to psychosocial health complaints. In men, statistically significant predictors were having a history of sickness absence, compulsive thinking, being mentally fatigued, finding it hard to relax, missing supervisory attention, and having no hobbies. Sensitivity and specificity assessment, on both the development and the validation of the screening instrument, resulted in rather low sensitivity rates, but high specificity rates for both men and women. We will present methodological features and limitations, and give recommendations for clinicians and policymakers.
Methodological features and limitations
With respect to the present study, several issues have to be acknowledged. First, information on predictive factors as well as on sickness absence due to psychosocial health complaints is obtained by self-reported measures. Even though the use of objective data is regarded as an ideal starting point, in case of psychosocial health complaints, both self-reported complaints and diagnoses given by medical specialists are rather subjective. A review by Johns states that both subjective and objective absenteeism data are moderately correlated.31 The review reports 11 correlations ranging from 0.30 to 0.92. The conclusion of the review is that self-reports can be considered a moderately valid measure of actual absenteeism. A second point of interest concerns the changeability to which self-reported reasons for sick leave are susceptible. Only those employees who explicitly stated that their latest sick leave was due to psychosocial health complaints were included as cases in this study. Since this self-report is not accompanied by a medical diagnosis or objective sickness absence data, the extent of sickness absence due to psychosocial health complaints is not comparable with prevalence measurements on a national level. A third issue concerns the time span between the assessment of predictive factors and the follow up of sickness absence after one year. The aim of this study was to predict sickness absence in healthy employees, i.e. employees who are not on sick leave and have not diagnosed themselves as suffering from chronic psychosocial health complaints, such as recurring depression. Including these employees creates a heterogeneous study population, which could lead to a misrepresentation of indicators for sickness absence. Therefore, a certain time span is necessary to develop psychosocial health complaints of such a level that an employee is unable to work. A fourth issue concerns the determination of a cut-off point with preferably both high sensitivity and high specificity rates. Unfortunately, no such cut-off point could be found on the developed screening instrument. Nevertheless, the value of an instrument will be determined by its practical usability and efficiency. Specifically, when an expensive preventive intervention is to be implemented after screening of a large group of individuals, a screening instrument with a high specificity rate is preferred, to ensure that the intervention will be directed at the individuals who will particularly benefit from it. For example, a cut-off point of 10 on the developed screening instrument, i.e. specificity scores of 91.3% for women and 90.6% for men, restricts the number of false positively classified healthy working employees. Nevertheless, the low sensitivity scores are undeniable and are responsible for the weakness of the instrument, i.e. an amount of false negatively classified employees. However, since the screening instrument is directed at healthy employees, the consequences of not identifying these employees are not very significant. If necessary, they can use the available health care, inside or outside their company, such as consultation with a social worker, general practitioner, or occupational physician. Combination of the developed screening instrument with a more sensitive instrument is a functional possibility for implementation. Finally, to put this instrument into practice, calculation of the sum score on the screening instrument should be easily manageable. Therefore, an electronic version in which a sum score will automatically be calculated is the most obvious solution.
Main message
-
It is possible to identify predictive factors for sickness absence and to develop an instrument for early identification of employees at risk for sickness absence.
Policy implications
-
Employers could use screening to determine which employees are eligible for early intervention, to identify and deal with specific psychosocial health complaints, and hence influence absentee rates and modify public health consequences on a larger scale.
Recommendations and conclusion
This study shows that it is possible to identify predictive factors for sickness absence and to develop an instrument for early identification of employees at risk for sickness absence. From a public and preventive medicine perspective, the presence of this screening instrument increases the possibility of implementing interventions directed at the prevention of sickness absence. For instance, employers could use screening to identify and deal with specific psychosocial health complaints, such as fatigue, and consequently influence the absentee rates. Moreover, the same in-company screening could be used to determine which employees are eligible for early treatment or social medical counselling. This is imperative for clinicians and policymakers in order to modify public health consequences on a larger scale. To investigate the effectiveness of the developed screening instrument more adequately, validation of this screening instrument in an additional population is necessitated. Also, implementation possibilities and consequences of falsely classified employees should be examined more thoroughly.
REFERENCES
Footnotes
-
Published Online First 12 May 2006
-
Competing interests: none declared