Article Text

Abstract
Aims: To investigate the acute systemic inflammatory response to welding fume exposure.
Methods: Twenty four welders (42% smokers) and 13 non-exposed controls (23% smokers) were monitored at a welding school. Exposure to fine particulate matter (PM2.5) was assessed using cyclone samplers. Markers of systemic inflammation, including C-reactive protein (CRP), fibrinogen, and white blood cell (WBC) levels, were determined in peripheral blood samples collected at baseline and after 5.3 (SD 1.0) hours of exposure.
Results: The median PM2.5 concentration for welders was 1.66 mg/m3, which was significantly greater than that for controls (0.04 mg/m3). Compared to non-smokers, smokers had a significantly higher baseline WBC count, but comparable levels of CRP and fibrinogen. In non-smokers, welding fume exposure was associated with a significant increase in WBC and neutrophil counts immediately following exposure (+0.8×103/μl, 95% CI 0.1 to 1.6, and +1.0×103/μl, 95% CI 0.4 to 1.7, respectively). A significant decrease in fibrinogen levels was observed in non-smokers (−32 mg/dl, 95% CI −63 to −1). No significant changes in WBC, neutrophil, and fibrinogen levels were found in smokers. Sixteen hours after welding exposure, CRP levels were found to be significantly increased in both non-smokers and smokers (0.90 mg/l, 95% CI 0.17 to 1.64). PM2.5 concentrations were found to be significantly associated with absolute neutrophil counts in non-smokers, and CRP levels in both non-smokers and smokers.
Conclusions: High levels of welding fume exposure induce acute systemic inflammation in a relatively young, healthy working population. These results also suggest that smoking may modify the effect of welding fume exposure on specific inflammatory markers.
- 95% CI, 95% confidence interval
- ATS, American Thoracic Society
- CRP, C-reactive protein
- PM2.5, particulate matter with an aerodynamic mass median diameter ⩽2.5 μm
- PM10, particulate matter with an aerodynamic mass median diameter ⩽10 μm
- RBC, red blood cell
- SD, standard deviation
- SEM, standard error of the mean
- WBC, white blood cell
- C-reactive protein
- inflammation
- systemic
- occupational health
- particulate matter
- welding fume
Statistics from Altmetric.com
- 95% CI, 95% confidence interval
- ATS, American Thoracic Society
- CRP, C-reactive protein
- PM2.5, particulate matter with an aerodynamic mass median diameter ⩽2.5 μm
- PM10, particulate matter with an aerodynamic mass median diameter ⩽10 μm
- RBC, red blood cell
- SD, standard deviation
- SEM, standard error of the mean
- WBC, white blood cell
The process of welding involves joining metal parts by heating the pieces to melting temperatures.1 Welding generates high levels of metal fume, which is comprised primarily of fine and ultrafine particles.2 Epidemiological studies have shown that exposure to welding fumes is associated with metal fume fever3,4 and increased respiratory symptoms.3,5 In addition, welders experience an increased prevalence of inflammatory lung diseases such as asthma and chronic bronchitis.6–9 Chronic exposure to welding fumes also is associated with a significant reduction in lung function;8,10 however, this association often is observed only in smoking welders, suggesting a possible interaction between welding fume and tobacco smoke on pulmonary responses.
In addition to causing adverse pulmonary effects, there is growing evidence that welding fume exposure also may be associated with increased cardiovascular events. Several studies have found that welders experience increased mortality from ischaemic heart disease.11–13 The observed increase in cardiovascular mortality most likely is not attributable solely to smoking. In a recent Swedish census, Sjögren and colleagues found that welders had a 10% excess risk in mortality from ischaemic heart disease compared to the general population, even after adjusting for smoking.13 Although the exact mechanisms are unknown, systemic inflammation resulting from occupational exposure to welding fume may be partially responsible for the increased cardiovascular risk in welders.
C-reactive protein (CRP), and to a lesser extent, fibrinogen and white blood cells (WBC) have been shown to be highly predictive of coronary heart disease.14–18 WBC, in particular neutrophils, are the primary acute inflammatory cells. The acute phase proteins CRP and fibrinogen also are sensitive, non-specific markers of inflammation.19,20 WBC, CRP, and fibrinogen levels have been utilised in numerous clinical and toxicological studies of inflammation, as well as in epidemiological studies investigating the association between particulate air pollution and acute systemic inflammation.21–23
In this study, we investigated the systemic inflammatory response to welding fume exposure. Blood samples were collected from welders and non-welding controls before and after their workshift. The inflammatory response attributable to welding exposure was determined by comparing CRP, fibrinogen, and WBC levels across the workshift. Data were further stratified by smoking status to determine whether smoking modified the effect of welding fume on the systemic inflammatory markers. Previous epidemiological studies have shown that cigarette smoking significantly affects CRP, fibrinogen, and WBC levels.24–26 We hypothesised that welding fume exposure would be associated with systemic inflammation, indicated by increased CRP, fibrinogen, and WBC levels. We further hypothesised that smoking status would significantly modify the association between welding fume and the various systemic inflammatory markers.
MATERIALS AND METHODS
Study population
The study was approved by the Institutional Review Board of the Harvard School of Public Health (Boston, MA, USA). Written informed consent was obtained from each subject. The study population consisted of 37 active and inactive boilermakers. Subjects were recruited and monitored at an apprentice welding school (Quincy, MA, USA) over three sampling periods, January/February 2003, June 2003, and January/February 2004. Sixteen of the 37 subjects were monitored more than once during the three sampling periods. A modified American Thoracic Society (ATS) questionnaire was used to collect information on medical history, current cardiopulmonary symptoms, smoking history, and occupational history of the subjects.
Twenty four subjects were exposed to metal fume and airborne fine particulate matter from shielded metal arc welding, gas tungsten arc welding (TIG welding), plasma arc cutting, and grinding. The most commonly used base metal was carbon steel. These 24 subjects with high levels of exposure to metal fume and fine particles were categorised as welders. Thirteen additional subjects served as controls, exposed primarily to background levels of particulate matter while performing bookwork and office tasks at the welding school.
Exposure assessment
Personal particle samplers were placed on the lapels of the subjects during their workday to monitor exposure to particles with an aerodynamic mass median diameter ⩽2.5 μm (PM2.5). The KTL cyclone (GK2.05SH, BGI Incorporated, Waltham, MA, USA) with a 50% aerodynamic diameter cutpoint of 2.5 μm was used in line with a Vortex Timer 2 personal sampling pump (Casella USA, Amherst, NH, USA) calibrated at a flow rate of 3.5 l/min. The air sample was collected on a 37 mm polytetrafluoroethylene membrane filter (Gelman Laboratories, Ann Arbor, MI, USA) encased in a cassette and placed downstream of the cyclone. The filters were weighed before and after sampling on a MT5 microbalance from Mettler-Toledo Incorporated (Columbus, OH, USA) after equilibrating for a minimum of 24 hours in a temperature and humidity controlled room. The mass collected on the filter was divided by the air volume sampled to calculate the gravimetric PM2.5 concentration.
Systemic inflammatory marker measurements
Venous blood samples were collected before work (baseline) and immediately after the end of the workday (six hours post-baseline). On a subset of subjects (n = 13), blood samples were also collected 24 hours after the baseline measurement. Blood samples were sent to Path Lab Incorporated (Portsmouth, NH, USA) for analysis. The Path Lab testing facility is in accordance with the Clinical Laboratory Improvement Amendments of 1988. Blood samples were analysed for CRP, fibrinogen, and total WBC count with differential. Quantitative determination of CRP in serum was performed with a Boehringer Mannheim/Hitachi 911 analyser (Roche Diagnostics Corporation, Indianapolis, IN, USA) using the latex particle enhanced immunoturbidimetric assay. The fibrinogen concentration in plasma was determined quantitatively with the Sysmex CA5000 coagulation analyser (Sysmex America, Incorporated, Mundelein, IL, USA) using the Clauss clotting method.27 The total WBC count was performed with an ADVIA 120 automatic cell counter (Bayer Diagnostics, Tarrytown, NY, USA) after haemolysing the red blood cells (RBC). The differential WBC count was performed with the ADVIA 120 analyser after differential cellular staining using the peroxidase method.
Urine analysis for cotinine
Urine samples were collected in sterile 120 ml containers before and after the workday, then aliquoted into 15 ml polypropylene tubes. Samples were sent to Path Lab Incorporated (Portsmouth, NH, USA) for urinary cotinine analysis. The presence of cotinine in urine was detected using an immunoassay procedure on an Olympus AU800 chemical analyser.
Statistical analysis
Statistical analyses were performed using SAS version 6.12 (SAS Institute Incorporated, Cary, NC, USA). Exposure status was dichotomised as non-exposed controls and welders. Study population characteristics between controls and welders were compared using two-sample t tests, Wilcoxon rank sum tests with exact p values, and Fisher’s exact test. The mean (standard deviation, SD) and median (25th–75th centile) values of the PM2.5 concentrations were determined for controls and welders. Two-sample t tests and Wilcoxon rank sum tests with exact p values were performed to compare the PM2.5 concentrations in controls and welders, and also in smokers and non-smokers. Dichotomised smoking status (yes/no) was confirmed by the presence of cotinine in the urine samples.
A total of 127 blood samples were collected from 37 subjects. Subjects provided two to three blood samples each time they participated, all at baseline and six hours post-baseline, and a subset at 24 hours post-baseline. In addition, 12 of the 37 subjects participated during two sampling periods and four participated in all three sampling periods. Baseline mean (standard error of the mean, SEM) levels of CRP, fibrinogen, WBC, and neutrophils were determined by exposure status and smoking status. To account for the repeated measurements, linear mixed models were used to investigate the effect of welding fume exposure on the systemic inflammatory markers. A generalised autoregressive covariance structure was used to account for the exponential decay of the correlation function as the interval between the measurements increased.28 Restricted maximum likelihood was used to estimate the covariance parameters. The effect of age on the baseline levels of the systemic inflammatory markers also was investigated. The distribution of residuals was examined using the Shapiro-Wilks test for normality and normal probability plots. Although the Shapiro-Wilks tests indicated that the residuals from some of the models might not be normally distributed (p < 0.05), the lack of significant curvature in the normal probability plots for all the models suggested that it was reasonable to assume that the random errors were approximately normally distributed. Therefore, for ease of interpretation of the results, the outcome variables were not transformed.
The following mixed effect model was constructed to examine the main effect of welding fume exposure on the measured change in inflammatory markers, adjusting for potential confounding by age, smoking, and time effects:
-
Model 1: (Δ systemic inflammatory marker)ij = β0 + β1(age – 37 y)i + β2(smoking status)i + β3(sampling time)ij + β4(exposure status)i + β5[(exposure status)i × (sampling time)ij] + eij
where β4 indicates the effect of welding fume exposure at 6 hours and β4+β5 represents the welding fume exposure at 24 hours, after adjusting for the effects of age (β1) and smoking (β2).
To further examine whether the effect of welding fume exposure depends on smoking status, the following mixed effect model with interaction terms between the main effect and smoking status was constructed:
-
Model 2: (Δ systemic inflammatory marker)ij = β0 + β1(age – 37 y)i + β2(smoking status)i + β3(sampling time)ij + β4(exposure status)i+ β5[(exposure status)i × (sampling time)ij] + β6[(exposure status)i×(smoking status)i] + β7[(exposure status)i × (smoking status)i × (sampling time)ij] + eij
where β4 and β4+β5 now indicate the effect of welding fume exposure at 6 hours and 24 hours among non-smokers, after adjusting for the effects of age (β1) and smoking (β2). β4+β6 and β4+β5+β6+β7 represent the effect of welding fume exposure at 6 hours and 24 hours among smokers. These two models were compared using the likelihood ratio test.
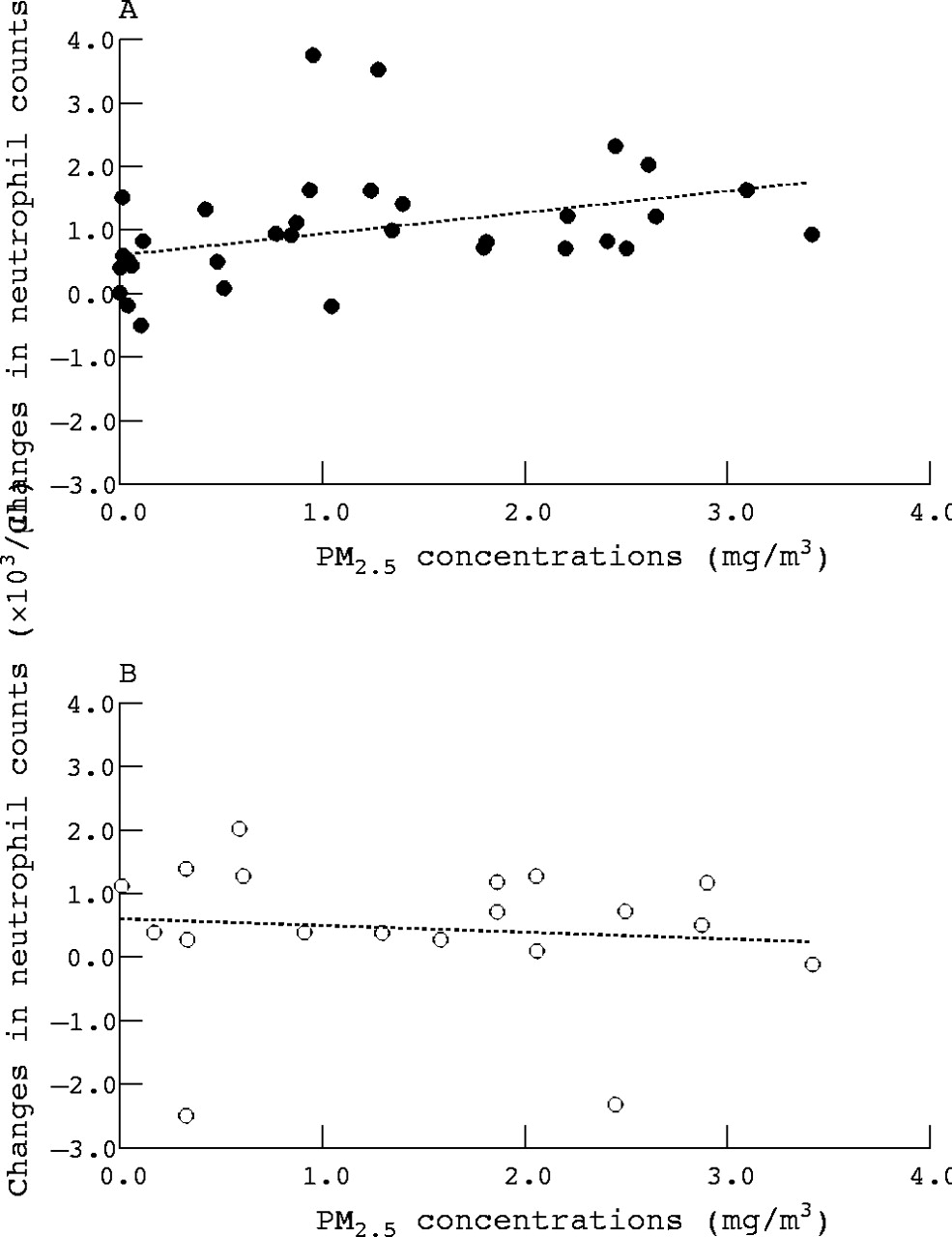
Similar models were used to investigate the linear exposure-response association between PM2.5 concentrations, indicated as a continuous variable, and levels of systemic inflammatory markers. The linear exposure-response association was examined based on scatterplots of data stratified by smoking status indicating an approximately linear relation between PM2.5 concentrations and changes in systemic inflammatory markers. Figure 1, for example, depicts the relation between PM2.5 concentrations and changes in neutrophil counts 6 hours post-baseline in non-smokers and smokers. The level of significance for all analyses was set at 0.05.
{kind=link}
Scatterplot of PM2.5 concentrations and baseline to 6 hours post-baseline changes in neutrophil counts; (A) non-smokers, (B) smokers.
RESULTS
Study population characteristics
Table 1 presents the study population demographic data. The study population included 37 men, of which 24 were welders and 13 served as controls. Their ages ranged from 19 to 61 years, with a mean of 41.5 years (SD 15.9) for controls and 35.0 years (SD 8.0) for welders. The controls had 5.0 years (median) of boilermaking experience, while the welders had 3.0 years (median) of experience. The mean age and median years of boilermaking were not significantly different in controls and welders (p ⩾ 0.1). Three of the 13 controls (23%) and 10 of the 24 welders (42%) were current cigarette smokers. The percentage of smokers in each group was not significantly different (p = 0.3). In general, the study population consisted of relatively young, healthy workers, with few having underlying respiratory or cardiopulmonary diseases.
Demographic characteristics and exposure assessment of non-welding controls and welders
Particle exposure assessment
Table 1 also shows the personal PM2.5 exposure data. Particle samples were collected from all controls and welders during the workday. Four of the 13 controls and 12 of the 24 welders were monitored on additional sampling days. The subjects, on average, worked for six hours at the welding school. Personal particulate matter samples were collected for a mean sampling time of 5.1 hours (SD 1.1) in controls and 5.3 hours (SD 0.9) in welders. The median PM2.5 concentration in controls was 0.04 mg/m3, with 25th–75th centile values of 0.02–0.11 mg/m3. In welders, the median PM2.5 concentration was 1.69 mg/m3, with 25th–75th centile values of 0.89–2.44 mg/m3. The median PM2.5 concentrations were significantly different between controls and welders (p < 0.001).
Baseline measurements of systemic inflammatory markers
Table 2 shows the baseline mean (SEM) levels of the systemic inflammatory markers. Age was shown to be a significant positive predictor of CRP and fibrinogen (p ⩽ 0.02), therefore all analyses were adjusted for centred age. Controls and welders were not found to have significantly different age adjusted mean baseline levels of systemic inflammatory markers (p > 0.05). In addition, the mean baseline CRP and fibrinogen levels were not significantly different in non-smokers and smokers (p ⩾ 0.2).
Comparison of mean (SEM)* levels of systemic inflammatory markers at baseline, stratified by exposure and smoking status
Smoking status was shown to affect mean baseline WBC counts (p < 0.001). The mean baseline WBC count was 2.1×103/μl (95% CI 1.2 to 3.1) greater in smokers compared to non-smokers. Similarly, smokers were found to have significantly greater baseline neutrophil counts compared to non-smokers (p < 0.001). The mean baseline neutrophil count in smokers was higher by 1.7×103/μl (95% CI 0.9 to 2.4) than in non-smokers. The mean percent neutrophils were also significantly different in non-smokers and smokers (p = 0.05).
Prior to participating in this study, the amount of time that subjects had away from boilermaking work ranged from zero days to several years. Analyses indicated that there were no significant differences in the baseline levels of any of the systemic inflammatory markers between subjects who had worked the previous day and those that did not (p ⩾ 0.3).
Changes in systemic inflammatory marker levels following welding fume exposure
Table 3 shows the mean effects (95% CI) of welding fume exposure on levels of systemic inflammatory markers across the workday. The results for the crude models, and age and smoking status adjusted models were similar. In the adjusted models, welding fume exposure resulted in a significant increase in WBC and neutrophil counts (p ⩽ 0.05), in addition to a marginally significant increase in percent neutrophils (p = 0.06). In addition, welding fume exposure was associated with a marginally significant decrease in fibrinogen levels (p = 0.08).
Mean effects (95% CI)* of welding fume exposure on baseline to 6 hours post-baseline changes in levels of systemic inflammatory markers
The age and smoking status adjusted models were compared to the adjusted models with interaction terms for smoking status. The likelihood ratio test indicated that for fibrinogen, and absolute and relative neutrophils, the models with the smoking interaction terms were a better fit for the dataset (p < 0.02). For the WBC model, the likelihood ratio test was marginally significant (p = 0.08). The significant likelihood ratio test results suggested the presence of effect modification by smoking status.
In smokers, there were no significant changes in any of the systemic inflammatory marker levels immediately following welding fume exposure (p ⩾ 0.5). In contrast, significant changes in WBC counts, and absolute and relative neutrophils were found in non-smokers (p < 0.03). Welding fume exposure was associated with an increase of 0.8×103/μl (95% CI 0.1 to 1.6) in WBC counts and an increase of 1.0×103/μl (95% CI 0.4 to 1.7) in neutrophil counts. In addition, a significant decrease in fibrinogen levels was observed in non-smokers (−32 mg/dl, 95% CI −63 to −1). CRP levels did not change significantly across the workday in non-smokers (p = 0.4).
Blood samples also were collected 24 hours post-baseline, 16 hours after the welding exposure. Table 4 shows the mean effects (95% CI) of welding fume exposure on levels of systemic inflammatory markers 24 hours after baseline. In both the crude and adjusted models, only CRP levels were significantly associated with welding fume exposure on the previous day (p < 0.02). Exposure to welding fume was associated with an increase in CRP levels by 0.90 mg/l (95% CI 0.17 to 1.64), after adjusting for age and smoking status. The interaction term for smoking status was not found to be statistically significant for any of the systemic inflammatory markers, suggesting a lack of effect modification by smoking status 16 hours after exposure (p > 0.2).
Mean effects (95% CI)* of welding fume exposure on baseline to 24 hours post-baseline changes in levels of systemic inflammatory markers
Association between PM2.5 exposure and systemic inflammatory marker levels
Table 5 presents the mean effects (95% CI) of PM2.5 exposure on levels of systemic inflammatory markers immediately after six hours of exposure. No significant exposure-response relations were observed between PM2.5 concentrations and systemic inflammatory markers in the crude and adjusted models. However, the adjusted models with the smoking interaction terms indicated a statistically significant exposure-response association between PM2.5 concentrations and neutrophil counts in non-smokers (p = 0.04). With each 1 mg/m3 increase in PM2.5 exposure, absolute neutrophil counts increased by 0.3×103/μl (95% CI 0.02 to 0.6) in non-smokers. Similarly, a marginally significant exposure-response association was found between PM2.5 concentrations and WBC counts in non-smokers (p = 0.09). Among non-smokers, each 1 mg/m3 of PM2.5 exposure was associated with a 0.3×103/μl (95% CI −0.05 to 0.7) increase in WBC counts.
Mean effects (95% CI)* of PM2.5 exposure on baseline to 6 hours post-baseline changes in levels of systemic inflammatory markers
The association between systemic inflammatory markers and occupational PM2.5 exposure from the previous day was also investigated. Table 6 shows the mean effects (95% CI) of PM2.5 exposure on levels of systemic inflammatory markers 16 hours after exposure. In both the crude and adjusted models, only CRP was associated significantly with the PM2.5 exposure from the previous day. In the adjusted model, each 1 mg/m3 increase in PM2.5 exposure the previous day was associated with a 0.78 mg/l (95% CI 0.35 to 1.22) increase in CRP levels. Smoking status was not found to affect significantly the association between PM2.5 concentrations and CRP levels (p = 0.6).
Mean effects (95% CI)* of PM2.5 exposure on baseline to 24 hours post-baseline changes in levels of systemic inflammatory markers
DISCUSSION
Welding fume is comprised of various gases and metal containing fine and ultrafine particles, with 90% of the particles having an aerodynamic mass median diameter less than 1 μm.1,2 In the present study, the median PM2.5 concentration for welders was 1.69 mg/m3, which was significantly greater than that for controls, 0.04 mg/m3 (p < 0.001). We found that acute exposure to welding fume was associated with increased levels of systemic inflammatory markers. Additionally, smoking was found to modify the effect of welding fume on specific inflammatory markers. Immediately following welding fume exposure, non-smokers experienced a significant increase in circulating WBC counts, specifically absolute and relative neutrophil counts, and a significant decrease in fibrinogen levels. Sixteen hours after exposure, both non-smokers and smokers experienced significantly increased levels of CRP. Significant PM2.5 exposure-response relations confirmed the welding fume associated increase in absolute neutrophil counts in non-smokers and CRP levels in all subjects.
In non-smokers, welding fume exposure was associated with a mean increase in WBC count by 0.8×103/μl (95% CI 0.1 to 1.6), a 13% increase from baseline. Likewise, neutrophil counts in non-smokers increased by 1.0×103/μl (95% CI 0.4 to 1.7), indicating that the increase in WBC counts following exposure may be mostly attributable to increased neutrophil counts. A significant exposure-response association also was observed between PM2.5 exposure and neutrophil counts in non-smokers (p = 0.04). There was no significant change in WBC and neutrophil counts following welding fume exposure in smokers (p ⩾ 0.6). In smokers, the acute inflammatory response as assessed by change in peripheral WBC counts was not significant, probably due to the fact that smokers already had an increased mean baseline WBC count of 8.5×103/μl (SD 0.4), which was 1.7×103/μl (95% CI 0.9 to 2.4) higher compared to non-smokers. Similarly, smokers had significantly higher neutrophil counts compared to non-smokers (p < 0.001). In previous studies, current smokers have been found to have increased WBC counts compared to former or never-smokers.25,26 One concern regarding the lack of change seen in smokers is that some of the subjects performed boilermaking work the day before participating in the study. The residual inflammation from the previous day’s work, in addition to the inflammatory response from smoking, may have contributed to the inability to observe a significant change in WBC counts in response to welding fume exposure.
Other studies also have shown that exposure to ambient and occupational particulate matter is associated with increased WBC and neutrophil counts.22,29 A study by Schwartz examined the association between urban air exposure and various blood markers.22 Schwartz observed a significant positive relation between circulating WBC counts and particulate matter with an aerodynamic mass median diameter ⩽10 μm (PM10), after controlling for several variables including smoking.22 The mean PM10 exposure in the Schwartz study was 35.2 μg/m3, nearly 50-fold less than the mean PM2.5 exposure in the welders in our study. In another study, non-smoking subjects exposed to diesel exhaust for one hour at a PM10 concentration of 300 μg/m3, experienced increases in peripheral neutrophil counts six hours after exposure.29
In blood samples taken 16 hours after exposure to welding fume, WBC and neutrophil counts in non-smokers were not found to be significantly increased compared to baseline levels. However, the similar effect estimates obtained from both the 6 hours and 24 hours post-baseline models indicated that acute systemic inflammation caused by welding fume exposure persisted. Each 1 mg/m3 increase in PM2.5 concentration was associated with a 0.3×103/μl increase in absolute neutrophil counts immediately after exposure compared to a 0.2×103/μl increase 16 hours post-exposure in non-smokers.
In addition to WBC counts, CRP and fibrinogen levels also were investigated in our study. Epidemiological studies have found that CRP and fibrinogen levels are increased in cigarette smokers.24,25 In our study, the baseline CRP and fibrinogen levels were not significantly different in non-smokers and smokers (p > 0.2). Unlike the other studies which had 4000+ subjects each, this study had a small number of subjects (n = 37) and most likely did not have adequate power to detect subtle differences in baseline levels. After exposure to welding fume, we observed a significant decrease in fibrinogen levels in non-smokers (p = 0.04); however, a significant exposure-response relation between fibrinogen levels and PM2.5 exposure was not found (p = 0.2). No significant change in fibrinogen levels was observed in smokers following welding exposure (p = 0.8). Epidemiological studies examining the relation between fibrinogen levels and particle exposure have observed conflicting results. Seaton and colleagues found that ambient PM10 measurements (range 16 μg/m3 to 24 μg/m3) were negatively associated with fibrinogen levels in non-smokers.23 However, Schwartz found that PM10 exposure was significantly associated with increased fibrinogen,22 while Sørensen and colleagues did not observe a significant association between ambient PM2.5 exposure (mean PM2.5 concentration of 16.1 μg/m3) and fibrinogen levels.30 Due to the circadian variation of fibrinogen, using this marker to detect changes associated with exposure may be difficult.31,32
Our study found that welding fume was not associated with significant changes in CRP levels immediately following exposure. However, 16 hours after exposure, a significant increase in CRP levels was observed in both non-smokers and smokers (p = 0.02). Smoking status was not found to significantly affect the association between PM2.5 exposure and CRP levels (p = 0.6). CRP levels increased by 0.90 mg/l (95% CI 0.17 to 1.64), resulting in a 39% increase from baseline. The exposure-response relation between the previous day’s PM2.5 concentrations and CRP levels was also statistically significant (p = 0.001). Each 1 mg/m3 increase in PM2.5 exposure on the previous day was associated with a 0.78 mg/l (95% CI 0.35 to 1.22) increase in CRP levels.
Studies investigating the effect of particulate air pollution on systemic inflammatory markers found that increased exposure to particulate matter was associated with significantly increased levels of CRP.21,23,33 Peters and colleagues observed that particle exposure (mean total suspended particle concentration of 54.0 μg/m3) was positively associated with CRP levels on the same day.21 However, the Peters study also indicated that particle exposure from the previous day was found to have a stronger effect on CRP levels, as shown in our study.21 A recent study by Pope and colleagues also found a significant exposure-response association between PM2.5 concentrations (mean 23.7 μg/m3) and CRP levels.33 In a study by Seaton and colleagues, a positive association was found between city centre PM10 measurements over a three day period and CRP levels.23
Many studies have shown that increased levels of systemic inflammatory markers are associated with increased risk of coronary heart disease and also predict adverse cardiovascular outcomes, although the exact mechanisms remain unclear.14,15,17,18 Chronic inflammation plays a major role in the pathogenesis of coronary heart disease.34,35 Increased levels of CRP may contribute directly to the atherogenic process or may reflect simply the extent of inflammation associated with atherosclerosis.18 Acute systemic inflammation also is associated with a series of adverse responses, including plaque rupture and platelet aggregation, that eventually lead to acute cardiac events.36,37 Even if these inflammatory markers are not involved directly in the aetiology of coronary heart disease, their usefulness as an early indicator of potential disease is of clinical value.
In conclusion, we observed acute systemic inflammatory responses following occupational exposures to high levels of fine particulate matter in a cohort of welders without overt cardiovascular diseases. An immediate increase was observed in peripheral WBC counts, mainly the neutrophils, but the acute effect on WBC was noted among non-smokers only. Sixteen hours after welding exposure, we began to observe a significant increase in CRP, among both smokers and non-smokers. The clinical significance of acute changes in WBC and CRP levels associated with welding fume exposure needs to be investigated further.
Acknowledgments
The authors are grateful to L Ngo, E Rodrigues, S Mukherjee, S Magari, J Cavallari, J Hart, L Su, Z Wei, and J Natkin for their assistance. Special thanks goes to the staff and members of the International Brotherhood of Boilermakers, Iron Ship Builders, Blacksmiths, Forgers and Helpers of Local No. 29, Quincy, Massachusetts.
REFERENCES
Footnotes
-
This study was supported by NIH grants ES09860, ES00002, and CA94715. Dr Kim was supported by Harvard-NIOSH Education and Research Center training grant T42110421 and a NIEHS post-doctoral fellowship T32 ES07069.