Article Text

Abstract
Aims: To describe the course of low back pain (LBP) among nurses across eight years.
Methods: A longitudinal study was performed with a follow up at 1 and 8 years among nurses employed by a large university hospital in Switzerland. A modified version of the Nordic Questionnaire was distributed to obtain information about demographic data, occupational activities, and various aspects of LBP. A clinical examination and several functional tests were used to overcome the problems associated with subjective pain reporting. Nurses having answered the questionnaire on all three occasions (n = 269) were classified into subgroups according to their pain intensity. For each subgroup the course of LBP was recorded.
Results: LBP was highly prevalent with an annual prevalence varying from 73% to 76%. A large percentage (38%) indicated the same intensity of LBP on all three occasions. The proportion of nurses reporting repeated increase of LBP (19%) was approximately as large as the proportion who complained about repeated decrease of LBP (17%).
Conclusion: It became evident that LBP poses a persistent problem among nurses. Over an eight year period almost half of the nurses indicated the same intensity of LBP, thus supporting a recurrent rather than a progressive nature of LBP.
- longitudinal study
- nurses
- low back pain
- LBP, low back pain
- LMD, localised musculoskeletal disorders
Statistics from Altmetric.com
Work related musculoskeletal disorders, and in particular low back pain (LBP), pose a major health and socioeconomic problem in modern society. It has been shown that 60–80% of the general population suffer from LBP at some time during their lives.1 Among nurses the lifetime prevalence was found to be slightly higher, varying between 56% and 90%.2,3
Despite these high prevalences the aetiology and the nature of LBP are not yet well understood. Many studies have been performed in various occupational settings, indicating a strong association between musculoskeletal disorders and work related factors.4 This was also found among nurses.5 The contribution of psychosocial factors6,7 and work pressure8 was also evident, but not as clear as has been shown for the physical factors.
Few longitudinal studies have been carried out focusing on the course of LBP. In the clinical context, chronic LBP is defined as LBP lasting more than three months. However, it is not known whether LBP takes a progressive aggravating course, or whether a recurrent or persistent nature may be assumed. As it is supposed to be a rather slow process, the follow up should cover a long period to detect changes across time. Longitudinal studies found previous LBP to be a predictor of subsequent complaints.1,7 This is confirmed by results of a five year follow up study indicating that previous back injury was a significant predictor of subsequent low back injury among nurses.9 Conversely other authors reported no association between previous and subsequent LBP.10 However, Abenhaim and colleagues11 found that 67% of the total number of episodes reported by nurses within a three year follow up were recurrences. The authors suggest the presence of a link between subsequent episodes, which could be partly due to an increased sensitivity of a previously injured spine. One three-year follow up study revealed that about half the nurses indicated stable complaints on all occasions.12 The proportion who developed new symptoms was as large as the proportion who recovered.
Main messages
-
The course of low back pain was almost stable over many years. This suggests a recurrent nature of LBP.
-
The annual prevalence of low back pain among nurses was high (73–76%).
-
The annual prevalence of LBP was reliably indicated by the subjects.
Policy implications
-
Patients with low back pain should be informed about the probable course of their symptoms.
-
Health surveys and in particular longitudinal studies are an important instrument for identification of the course of musculoskeletal disorders. In this context, work related information, for example, the reason for job leaving, is required.
It is evident that there is still a considerable lack of knowledge about the long term course of LBP. Hence the aim of the current study was to describe the short and long term course of LBP among nurses over several years.
METHODS
Study group
Baseline in 1991
In 1991 a self administered questionnaire was sent to the home addresses of all nurses employed by a large university hospital (n = 1963).13 Two reminders were posted to the non-respondents, the second being a shortened version of the original questionnaire. Responses of 1460 nurses (74%) were available. Exclusion of pregnant women and responses to the second reminder reduced the number to 1307 nurses providing complete data.
Follow up in 1992
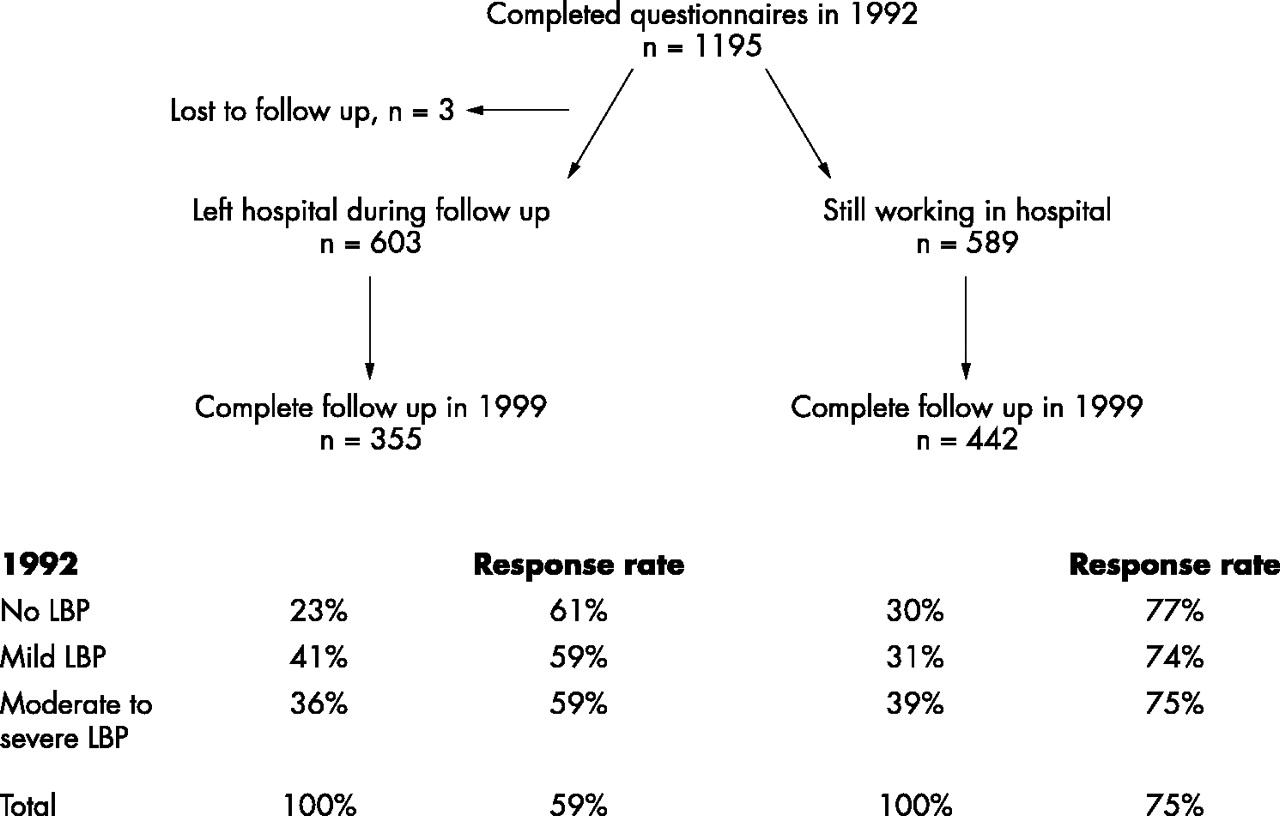
In 1992 the same self administered questionnaire was sent to all nurses employed at the hospital (n = 2185). As in 1991 there was no association between back complaints and a delayed response, in 1992 only one reminder was posted to promote participation among those who had not responded. The participation rate was 55% (1195/2185). Exclusion of pregnant women reduced the number of responders suitable for subsequent analysis to 1159 (53%). Of 1307 subjects who had participated at baseline, 630 (48%) filled in the questionnaire at follow up, representing the sample with complete data for further analysis of the short term course (18 months) of LBP.
Follow up in 1999
In 1999 all nurses employed at the hospital at that time as well as those already having participated in 1992 again received the same questionnaire. One reminder was posted, resulting in a response rate of 58% (1584/2744). Of all nurses having answered in 1992 (n = 1195), 603 had left the hospital. They were intensively followed up by two reminders. The participation rate of the latter was 59% (355/603), and was 75% (442/589) among those still working at the hospital.
Subjects having participated in 1991, 1992, and 1999 (n = 269) represent a well described cohort permitting a thorough analysis of the long term course of LBP.
Questionnaire
The questionnaire used in the current study was a slightly modified version of the “Standardised Nordic Questionnaire” on LBP.14 An illustrated part was added to collect information on LBP and other localised musculoskeletal disorders (LMD).15 The following information was provided:
-
Sociodemographic data: age, nationality, marital status.
-
General information on occupation and work load: hospital department, ward, seniority, degree, part time work, shift work, night work, frequent lifting, awkward working posture, repetitive movements, permanent standing or permanent sitting during work.
-
Leisure time activities: physical activity, regular fitness, or strength training.
-
Prevalence and duration of low back complaints: ever LBP, first occurrence of LBP, hospitalisation or job change due to LBP, duration of LBP within the preceding 12 months (0/1–7/8–30/>30 days/every day), effects on work and leisure time activities, sick leave, medical history, current LBP, lifetime duration of LBP, problems due to LBP, and number of episodes.
-
Prevalence and duration of LMD according to assignment to the illustrated questionnaire: in the last part of the questionnaire a figure was displayed. Disorders could be assigned to different parts of the body. Contrary to the binominal answer (yes/no) suggested by the “Nordic Questionnaire” the scale was modified using different categories (never/1–7/8–30/31–90/>90 days musculoskeletal disorders within preceding 12 months).
Classification of LBP
Assuming that the initial pain status plays a major role in the subsequent course of LBP, three subgroups of different pain intensities were formed: no, mild, and moderate to severe LBP. Subjects were assigned to the subgroups according to their specification of the total length of time they had experienced LBP in the preceding 12 months. Answer “0 days” was classified “no pain”, “1–7 days” as “mild pain”, and “⩾8 days” as “moderate to severe pain”.
Clinical examination and functional tests
A subgroup of subjects having returned the questionnaire in 1991 was randomly selected for a clinical examination. Cases were defined to be subjects either reporting more than 30 days LBP in the preceding 12 months or 8–30 days and at the same time disability in their daily activities at work or at home (n = 148). Controls were a random sample of subjects who had never suffered from LBP (n = 91).
The clinical examination addressed the shape of the spine in the frontal and sagittal plane, and the presence of radiating pain and/or neurological signs.16 The test protocol was based on the recommendations of the “Quebec Task Force”.17 The mobility of the spine was measured using the Cybex Electronic Digital Inclinometer. Th12/L1 and L5/S1 were the reference points. After warming up subjects were measured in a standing position and performed flexion movements after standard instructions. The distance in cm between the reference points was registered.
Further functional tests were conducted comprising isometric endurance of the back extensors, isometric and isokinetic strength measurements, and a progressive isoinertial lifting evaluation.
The isometric endurance of the back extensors was measured in a modified version of the procedure described by Biering-Sørensen.18 The subject lay prone with the legs fixed and the arms at the side attached to the head. A pillow was used to support the pelvis. Time until the subject could no longer maintain the horizontal position was measured, with a maximum time of 120 seconds.
For isometric strength measurements of the trunk flexors the subjects had to lie supine, placing the lower legs on a step, thus forming an orthogonal angle with the upper legs, and then curl up, again not exceeding 120 seconds.
Isometric strength during knee extension was measured with the hips orthogonal to the knees. Again time was recorded until a maximum of 120 seconds was reached.
Isokinetic strength was determined using the Cybex Liftask (Lumex, Ronkonkoma, NY).19 A pretest was performed the day before the examination in order to familiarise the subjects with the equipment. The subject was fixed to the device and measurements were carried out in flexion and extension at a speed of 60, 120, and 150 degrees per second respectively. For further analysis results were averaged for each subject.
Finally isoinertial lifting capacity was evaluated according to the procedure described by Mayer and colleagues.20
Results of all functional tests were related to reference values obtained from a group of pain free subjects (n = 121).16
Results of both the clinical examination and the functional tests were used to determine the problems associated with subjective pain reporting and to describe cases and controls within a clinical context.
Statistical analysis
Reliability of the subjects’ specification of the duration of LBP within the preceding 12 months was assessed by comparing answers given to both the illustrated and the non-illustrated part of the questionnaire. Spearman correlation coefficients were used to assess the reliability between both items.
The reliability of the subjects’ indication of the lifetime duration of LBP was analysed by regression equations. The reliability between answers given in 1991 and 1992, as well as between answers given in 1992 and 1999, was analysed.
ANOVA was used to investigate whether an increase in intensity of LBP (expressed as number of days with LBP in the preceding 12 months) is associated with an increase in the lifetime prevalence of LBP (expressed as years with persistent or recurrent LBP) or vice versa.
Data obtained from the clinical and functional evaluation of cases and controls were compared by univariate analysis. Odds ratios were adjusted for three age groups (⩽33/34–43/⩾44 years) and sex. Correspondent 95% confidence intervals (95% CI) were calculated on the basis of the standard errors assuming asymptotic distribution.
To reveal a potential healthy worker effect, subjects who had left the hospital in 1992 and subjects who stayed were compared for frequency and intensity of LBP as indicated in 1992 (Mann-Whitney test). Furthermore, the association between the intensity of complaints and response rate was analysed.
All statistical analyses were performed with the SAS program 6.12 software package. Pregnancy was an exclusion criterion since a relation between pregnancy, delivery, and the occurrence of LBP has been reported.21 Answers to the second reminder posted in 1991 and 1999 were disregarded since it was just a shortened questionnaire.
RESULTS
Population
The total study population with complete short term follow up data (cohort 91–92) consisted of 630 subjects. For the long term follow up the number of subjects with complete data was 729 (cohort 92–99), and 269 (cohort 91–92–99) respectively. A late responder analysis revealed no significant association between the prevalence of LBP and a delayed response. Thus it may be assumed that subjects who returned the questionnaire pose a representative sample. Table 1 shows the basic characteristics of the nurses with complete follow up data for each of the cohorts. Comparison of nurses having left the hospital during follow up and those still working there revealed that there was no significant difference in intensity and frequency of low back pain (p > 0.1). For details see fig 1. As expected, the response rate was higher among nurses still working at the hospital. However, there was no significant association with the intensity of complaints.
Individual characteristics of the different cohorts at baseline
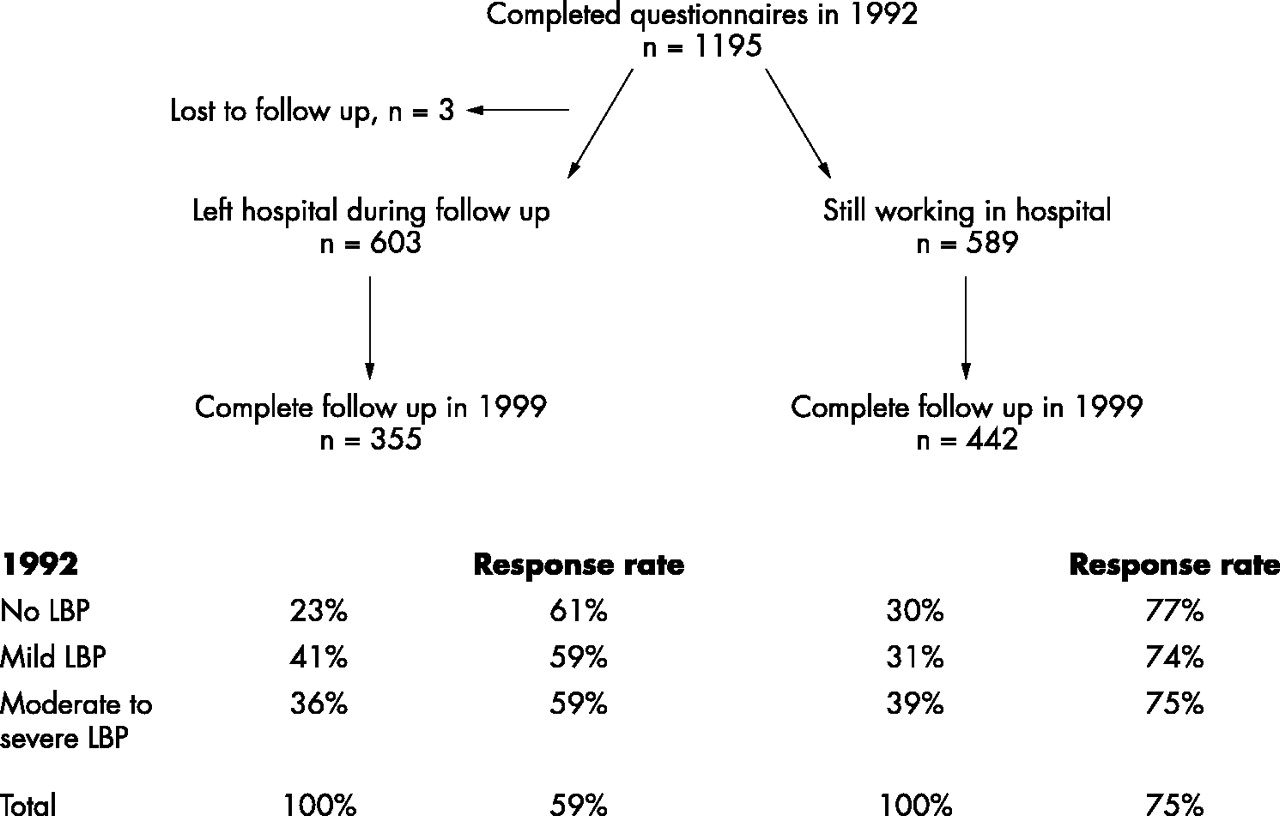
Prevalence and intensity of pain in the low back in 1992 for nurses still working or having left hospital during follow up.
Reliability of various aspects concerning LBP
Since further analysis of the course of LBP refers to the variable “duration of low back pain within the preceding 12 months”, it is essential to investigate the reliability of answers given to this question and its association with other aspects of LBP.
The reliability of the subjects’ specification concerning the 12 month prevalence of LBP was analysed by comparing answers to both questions on duration of LBP within the preceding 12 months in the illustrated and the non-illustrated part of the questionnaire. Reliability between these items appeared to be R = 0.82 at baseline (p = 0.001, standard error (SE) = 0.021), R = 0.81 at first follow up (p = 0.001, SE = 0.024), and R = 0.79 at second follow up in 1999 (p = 0.001, SE = 0.027). Coefficients of R ⩾ 0.8 (p < 0.05) indicate good correlation.22 Hence for all further analysis a new variable was built (mean of both answers) indicating the LBP status in the preceding 12 months.
Provided that subjects reliably indicate the lifetime duration of LBP over the years, the following should result when comparing answers given at baseline and follow up: The acclivity of the evens should be 1 for both the short and long term follow up, whereas the axis intercepts should be located at 1.5 and 7 for the short and long term follow up, respectively. The following result for the short term follow up was obtained: y = 2.69 + 0.83x, R = 0.79 (x = lifetime duration of LBP recorded in 1991 (years), y = lifetime duration of LBP recorded in 1992 (years), R = Pearson correlation, n = 276). Consequently in 1992, subjects tended to underestimate the duration of LBP. For the long term follow up (cohort 92–99) the equation was y = 5.52 + 0.81x, R = 0.67 (x = lifetime duration of LBP recorded in 1992 (years), y = lifetime duration of LBP recorded in 1999 (years), n = 306). According to these results recall of the lifetime duration of LBP seems to be difficult with increasing follow up interval.
Analysis of variance revealed a slight but significant association (p = 0.04) between the lifetime duration of LBP, and the duration of LBP within the preceding 12 months when focusing on data of the cohort 92–99. Analysis of the other cohort (91–92) delivered non-significant results (p > 0.5) (table 2).
Association between severity of LBP (number of days with LBP in the preceding 12 months) and lifetime duration of recurrent LBP in years
Validity of self assessed intensity of LBP
The clinical examination and the functional tests served to establish validity of the classification into cases and controls. Cases and controls differed slightly but significantly regarding height and weight: cases were 168 ± 9 cm tall and their weight was 67 ± 12 kg, whereas controls were less tall (166 ± 9 cm) and had a lower weight (64 ± 13 kg).
The clinical examination revealed significant differences between cases and controls. Scoliosis and shifts of the spine as well as a hunchback and reduced lordosis and kyphosis were more frequent among cases (table 3).
Results of the clinical examination of controls and cases
Concerning the results of the functional tests, the largest difference between cases and controls was found for the progressive isoinertial lifting situation. In the lower lifting test, 27% of the cases achieved values below normal—that is, 75% of the mean of a reference group, whereas it was only 8% in the control group (OR 4.2, 95% CI 1.8 to 9.9). For the upper lifting test similar results were found (OR 3.5, 95% CI 1.3 to 9.5). Furthermore, static strength of the back extensor and the leg muscles was found to be significantly lower in cases than in controls (OR 1.8, 95% CI 1.0 to 3.1 and OR 2.0, 95% CI 1.1 to 3.5). Similarly, cases showed significantly lower outcome in measurements of dynamic strength (OR 2.7, 95% CI 1.0 to 7.1). Concerning the flexibility of the lumbar spine, no significant differences between cases and controls were found.
Short and long term course of LBP
Subjects participating on all three occasions—that is, at baseline, in 1992 and 1999 (n = 269), pose a well defined cohort to investigate the long term course of LBP. LBP was highly prevalent at baseline. Thirty five per cent of the nurses complained of mild LBP (1–7 days) and 33% of moderate to severe LBP (⩾8 days) within the preceding 12 months (table 1). The respective intensities of LBP at baseline and follow up were closely related. Thirty eight per cent of all nurses indicated the same intensity of LBP (no, mild, or moderate to severe pain) on all three occasions. Complaints decreased in 19%, increased in 17%, and varied in 27% of all nurses. Considerable changes (no pain to moderate–severe pain and vice versa) were less frequent (12%). Figure 2 displays the most frequent courses within eight years (cohort 91–92–99). It appeared that LBP took the same course across years irrespective of the original pain intensity. Similar results were obtained when analysing the course of LBP on the basis of the other cohorts (91–92, 92–99). Considering the original five point ordinal scale it becomes evident that major changes comprising more than two categories occurred even less frequently (4%) (for details see tables 4 and 5).
Number of subjects according to their specification of LBP within the preceding 12 months at baseline and follow up in 1992 (n=627)
Number of subjects according to their specification of LBP within the preceding 12 months in 1992 and follow up in 1999 (n=728)

{kind=link}
{kind=link}
Course of LBP among subjects claiming moderate to severe (A), mild (B), or no (C) LBP at baseline. The three most frequent courses are shown.
DISCUSSION
The main purpose of this study was to identify the long term course of LBP among nurses in relation to the original pain intensity. In this context it should be kept in mind that the term “pain intensity”, as it is used in the current study, solely refers to the duration of LBP within the preceding 12 months.
To avoid selection bias, it is essential to include not only pain free subjects but also subjects indicating different intensities of LBP at baseline. The former criterion is hard to meet since in most subjects the first onset of LBP occurs early in life. In the present study, pain free subjects have been defined as persons indicating no complaints within the preceding 12 months. Abenhaim and colleagues11 suggest that this period might be too short as they observed that 14.3% of their study population had a first recurrence not until the first year of follow up. Consequently a pain free time interval comprising one year appears rather short to eliminate recurrent cases. However, in the present study the short term course of LBP (18 months) showed no significant tendency towards decreasing or increasing symptoms. These findings suggest a longer recurrence period since most changes did not take place until the second year of follow up.
Both the clinical examination and the functional tests showed significant differences between cases and controls, thus supporting the information retrieved from the questionnaire. Nevertheless, it should be noted that only a subsample of subjects was clinically examined, which hampers generalisation of results. Another limitation concerns the point that data retrieved from questionnaires and those obtained from clinical examinations may not necessarily overlap. However, from the current study it may be concluded that the subjects’ specification of the duration of LBP within the preceding 12 months corresponds with the clinical and functional outcome.
Concerning the reliability of recall of former pain episodes we found that subjects tended to underestimate the persistence of LBP, which means the lifetime duration of LBP since the first onset of complaints. Within 18 months recall was shown to be reliable. However, with increasing time interval between baseline and follow up, it became more and more difficult to remember episodes of LBP. Nevertheless the correlation coefficients indicated good reliability with respect to the lifetime duration of recurrent LBP.
The prevalence of LBP was found to be 73–76%. Several authors report lower annual prevalences of LBP in nurses varying between 45% and 58%.23–26 As stated by others,23,27 comparison between studies might be difficult as definitions of the term LBP vary considerably. Furthermore, the heterogeneity of different nursing populations should be considered. However, the current results emphasise that nurses run a high risk of suffering from LBP.
We found that LBP was stable for eight years in approximately half the nurses. It appeared that LBP took the same course over the years irrespective of its intensity at baseline. There was no significant trend, neither towards increase nor to decrease of complaints. One explanation might be that experienced nurses avoid harmful physical load and additionally have developed better coping strategies than less experienced younger nurses. This would partly compensate for a cumulative effect of putative risk factors. Another explanation would be a selection effect. However, there was no significant association between leaving the hospital during follow up and the intensity of complaints at baseline. Although a healthy worker effect cannot be completely excluded by a late responder analysis, it may be assumed that there is little evidence for its occurrence. Thus it may be assumed that the remaining nurses pose a representative sample for study of the course of LBP over several years.
When considering that changes might occur due to slightly different answers at follow up, it becomes even more evident that complaints were stable. Josephon and colleagues12 reported similar results in a three year follow up study of nurses. The size of the cohort was comparable to ours. They reported that about half the nurses indicated stable complaints on all occasions. The proportion who developed new symptoms was as large as the proportion who recovered. However, they used another definition of a case based on the indication of ongoing symptoms with a score >6 on a 10 point scale in at least one of the following body regions: neck, shoulders, or back. Moreover, they did not consider the subjects’ initial pain status. This makes comparison with our results difficult. Nuebling and colleagues28 followed the course of LBP in nursing students from the beginning of their working life. In contrast to our results they found that the lifetime prevalence as well as the annual prevalences of LBP steadily increased over five years. The different findings might be due to differences in age and hierarchical composition of the cohorts. In another study it was reported that a longer period of time since the last episode of LBP predicted a lesser risk of LBP occurrence in the follow up year.1 This means that the more recently and frequently a subject experienced LBP the more liable he or she will be to have further complaints. These findings suggest not only a recurrent nature of LBP but also a trend towards aggravation with increasing persistence of complaints. However, our results do not support this theory. We found no significant association between the lifetime duration of recurrent LBP and its intensity in terms of duration of LBP within the preceding 12 months. Because the long persistence of LBP is independent from the pain intensity we suggest that the nature of LBP is recurrent with only minor tendency towards improvement or aggravation.
The association between LBP and age is controversial. It has been reported that the mean age of nurses with current back pain was slightly but significantly greater than those without.29 Conversely it has been found that LBP decreased with age,2,11 whereas others suggested that it was not related to LBP.23,30 Similarly, our results revealed no significant association between age and LBP.
The strength of this study lies in the longitudinal study design with a long follow up interval providing data about the long term course of LBP. The questionnaire used in this study delivered reliable results and appeared to be valid with respect to the outcome of functional tests and clinical examination. In contrast to other studies we followed up not only healthy subjects, but also subjects indicating different intensities of LBP at baseline. The fact that the study population was a well defined group of subjects working in a single hospital eliminated employer to employer variability. This advantage carries a possible limitation of generalisability. However, there is no obvious reason for the university hospital being unique. Hence it may be assumed that results are transferable to other large hospitals with similar organisational structure.
Conclusions
This study showed that LBP still poses a major problem among nurses. Over several years, a large percentage of all nurses indicated the same intensity of complaints. Therefore it might be suggested that LBP takes a recurrent rather than an aggravating course, which should be considered in the future management of LBP in the healthcare sector. It is hypothesised that adapted coping strategies among experienced nurses contribute to a large extent to these findings. Further analysis will elucidate putative predictive factors.
Acknowledgments
This study was supported in part by the BBW (Project “SOS-LBD”, No. 97.0046).