Article Text

Abstract
Aims: To determine the prevalence of proteinuira and enzymuria among a cohort of subjects exposed to hexachlorobutadiene (HCBD) in their homes and to determine whether there was a change in observed effects when exposure ceased.
Methods: Residents underwent a health check, which included a panel of urinary markers of both glomerular and tubular origin, within two months of cessation of long term exposure to HCBD and again at least 10 months after exposure ceased. Analysis of the results was performed to determine if there was any early evidence of renal effects, and to ascertain whether changes in these parameters occurred after exposure to HCBD ceased.
Results: Tubular proteinuria and enzymuria were increased in the initial health check and significantly decreased after the residents had left their homes for about 10 months. As the early renal tubular markers improved when exposure ceased it is anticipated that the long term nephrotoxic risk will be minimal, but the carcinogenic risk remains unknown.
Conclusions: Results show there was a renal effect which improved when subjects left their homes. This suggests there was a local environmental factor responsible for the observations. This is consistent with the predicted toxicological effects of HCBD from animal studies.
- contaminated land
- hexachlorobutadiene
- CPB, cysteine-S-pentachlorobutadiene
- GPB, glutathione-S-pentachlorobutadiene
- GST, glutathione-S-transferase
- HCBD, hexachlorobutadiene
- IAM, indoor air quality monitoring
- TCCT, trichlorovinyl-chlorothioketene
Statistics from Altmetric.com
- CPB, cysteine-S-pentachlorobutadiene
- GPB, glutathione-S-pentachlorobutadiene
- GST, glutathione-S-transferase
- HCBD, hexachlorobutadiene
- IAM, indoor air quality monitoring
- TCCT, trichlorovinyl-chlorothioketene
The United Kingdom has a legacy of contaminated land as a result of past industrial, mining, and waste disposal activities. It has been estimated that there are between 50 000 and 100 000 potentially contaminated sites across the nation. Local authorities have longstanding duties in relation to environmental issues. New legislation with effect from 1 April 2000 brought into force a new regime for the identification and remediation of contaminated land. Its main objective is to investigate contaminated land that may pose unacceptable risks to human health.1
Halton Borough is located in the English County of Cheshire and spans the river Mersey. Major chemical industries have operated in the area for over a century, resulting in a legacy of contaminated land. Two former sandstone quarries within the village of Weston, used for the disposal of industrial waste until the early 1970s, were of particular public health concern.
Main messages
-
A cohort of subjects residing on an area of contaminated land, through which they were exposed to the known animal nephrotoxin and carcinogen, HCBD, were investigated.
-
The cohort showed evidence of subclinical tubular proteinuria and enzymuria.
-
These parameters improved when the subjects were reinvestigated, having left their homes for approximately 10 months.
-
A number of possible confounding factors are discussed; however, the results suggest that the effects observed are likely to be caused by local environmental factors.
Policy implications
-
It is likely that similar areas of contaminated land will be identified in the UK. Local authorities should obtain public health advice when investigating the potential health risks.
-
This study re-emphasises the need to consider potential health implications of developing “brownfield” sites for residential housing.
Ground investigations revealed that vapour transport of volatile chemicals was occurring in the vicinity of these quarries. A hazard assessment indicated that the chemical hexachlorobutadiene (HCBD) posed a risk to health. Subsequently, indoor air quality monitoring (IAM) commenced in January 2000 and revealed the presence of this chemical in 20 homes at levels up to 6.8 parts per billion (ppb). In one additional property, the chemical was detected at levels up to 1000 ppb. All these buildings were located immediately to the west of the North Quarry.
HCBD is toxic.2 Investigations have shown that its effects in animals are mainly restricted to the kidneys, including carcinogenicity. The effects on human populations, at low levels of exposure via inhalation, are unknown. The American National Occupational Safety and Health Administration (NIOSHA) recommends that exposure to HCBD should not exceed 20 ppb for a eight hour workday within a 40 hour working week.3
There were no guidelines on safe levels for residential exposure to HCBD. Therefore, the UK Committee on Toxicity, supported by the Committee on Mutagenicity, reviewed HCBD. Their guidance stated that, for non-carcinogenic effects, levels of exposure to HCBD below 0.6 ppb should not represent a significant risk to health.4 Furthermore, the committee believed the carcinogenic risk to be minimal below this level.
A second phase of IAM was conducted in June 2000 and confirmed the original results. However, HCBD was also detected, at levels above 0.6 ppb, in six additional adjacent properties.
To safeguard the health of the residents, the local health authority advised that exposure to HCBD should be kept below the reference value produced by the Department of Health. Unfortunately, environmental experts concluded that remediation of the houses was impossible and so most subjects elected to leave their homes.5
This paper describes the results of the health authority’s health investigations.
HCBD—PHYSICAL PROPERTIES AND TOXICOLOGY
HCBD (C4Cl6) is a by-product of the manufacture of chlorinated hydrocarbons and does not occur naturally. The metabolism and toxicology of HCBD has been studied in experimental animals. Following oral administration, HCBD is conjugated in the liver with glutathione to glutathione-S-pentachlorobutadiene (GPB), which is excreted in bile (fig 1). After secretion into bile GPB is partially degraded to cysteine-S-pentachlorobutadiene (CPB) in the bile duct epithelium.6 Following enterohepatic recirculation, GPB and CPB are delivered to the kidney where CPB is metabolised in the proximal tubule by the enzyme β-lyase to the reactive electrophile trichlorovinyl-chlorothioketene (TCCT).7 Covalent binding of this final compound to adjacent tissues is responsible for the site specific toxicity of HCBD.8

Schematic and simplified diagram of the metabolism and toxicology of HCBD.
Damage occurs principally in the kidney causing proximal tubular necrosis.9,10 Rats fed very high concentrations of HCBD, for prolonged periods, showed a significant increase in incidence of renal tubular neoplasms compared to controls.2 Toxic doses reduce conception rates and birth weights.11,12
HCBD is also genotoxic. Point mutations can be induced in Salmonella typhimurium by incubating the organism with HCBD in the presence of rat liver.13
In vitro human tissues studies have shown that hepatocytes metabolise HCBD to GPB using glutathione-S-transferase14 and that CPB causes β-lyase dependent cytotoxicity to proximal tubular cells.15 As human kidney β-lyase activity is lower in comparison to rats, humans may be less susceptible to HCBD toxicity.16
Residents living to the west of the North Quarry were exposed principally by inhalation, which avoids first pass hepatic metabolism of the compound, and so the health effects may differ from those observed in animal investigations. There are few studies of the effect of the compound in vivo in humans and none on the effects of long term inhalation exposure in the residential setting.17
The aim of the investigations was to determine whether there was any evidence of harm, or potential harm, in individuals exposed to levels of HCBD in excess of annual average concentrations of 0.6 ppb with special reference to renal disease. Furthermore, to determine whether there was an improvement in abnormalities detected when exposure to HCBD ceased.
METHODS
Study design
A longitudinal prevalence study of indicators of renal glomerular and tubular function observed within two months of cessation of long term exposure to HCBD and at least 10 months after exposure ceased.
Subjects in permanent residence at the time that HCBD was detected, at average concentrations in excess of 0.6 ppb, were invited to participate in the study. Eighty two subjects were eligible and 70 participated in the first phase of the investigation. Among the 70 who attended there were 15 children aged less than 16 years, 53 subjects aged 16–65, and two subjects aged over 65 years.
Everyone who underwent the first examination was offered a second round of tests. To avoid introducing participation bias, this was completed prior to participants being informed of the initial results. Forty seven subjects (67%) attended for the follow up examination. This sample comprised 10 children aged less than 16 years, 37 subjects aged 16–65 years, and none over 65 years.
Clinical investigations
A full medical history was taken from all subjects.18 The subjects underwent a physical examination and an ultrasound examination of the liver, biliary system, pancreas, and urinary tract. Blood was examined for routine biochemistry and liver function tests, α fetoprotein, and routine haematological parameters. A 24 hour urine collection was obtained and used to measure creatinine clearance and total urinary protein excretion. Urine was also examined cytologically. Those with microscopic haematuria or atypical urinary epithelial cells were offered cystoscopy. No cases of urinary tract neoplasia or overt renal dysfunction were identified by these methods.
Overt clinical renal disease, from prolonged exposure to chemicals, would only occur after a major part of renal function had been lost. Routine clinical tests are not sufficiently sensitive to be informative, except in the most extreme situations. Therefore a panel of site specific urinary markers of early tubular and glomerular effects were used (table 1).
Urinary markers representing different sites of effects in the nephron
The use of a panel of markers to detect early renal disease is well established in a variety of occupational settings,19 including investigations into exposure to industrial hydrocarbons20,21 and cadmium.22 While the application of these tests is relatively new in population settings, an almost identical approach has been recommended by the American Agency for Toxic Substances and Disease Registry for case studies of persons exposed to hazardous substances at waste sites.23 These measurements have the advantage of being easily made and have great sensitivity but, unfortunately, do not test specifically for nephrotoxic effects of HCBD.
Table 2 summarises the assays used to quantify the urinary markers. The tests were performed at the Health and Safety Laboratory, Sheffield, UK and were subject to internal quality assurance schemes. These procedures ensure that assay drift does not introduce measurement bias. To allow for variations in urinary flow rate and concentration, urine parameters were corrected per millimole creatinine excretion.24 The normal ranges for all tests, except α- and π-GST (glutathione-S-transferase), were calculated using 97.5% centiles from a cohort of 320 working subjects with no history of exposure to nephrotoxins. The ranges for α- and π-GST are mean ±2SD (taking log distribution into account) from 72 control subjects.25 To make the study group as comparable as possible to “healthy workers”, only participants aged 16–65 were included. Also, any participant who was found to have a pre-existing renal condition was excluded from the following analysis, as were those known to be taking non-steroidal anti-inflammatory drugs.
HSL assays used to quantify urinary proteins and enzymes
These investigations were undertaken to deal with the emergency clinical situation that had arisen subsequent to the discovery of the contaminated homes. All subjects gave informed consent to the clinical investigations, and also consented to the pooling of results to enable public health investigations. The residents gave verbal consent to the publication of the pooled results at a meeting with the investigators.
Statistical analysis
Subjects who completed both rounds of investigations were included in this analysis. The results were compared by two methods. Firstly, the results of first and second round tests were compared by the paired t test. Secondly, the number of abnormal results of proximal tubular tests, in subjects aged 16–65 years, was compared by simple frequency counts.
RESULTS
Table 3 shows the results of the urinary proteins and enzymes. It can be seen that four of the five proximal tubular markers had significantly decreased in the second round of tests. Similarly, the distal tubular marker, π-GST, showed a significant decrease. The markers of glomerular function did not show any significant change.
Comparison of urinary protein/enzyme levels shortly after (first round) and at least 10 months (second round) after subjects left their homes
Table 4 shows how many of the tests performed on subjects aged 16–65 years exceeded the HSE laboratory’s reference range. Comparison of tables 3 and 4 reveals that while there was a significant decrease in the mean N-acetyl-d-glucosaminidase level, only two participants initially had levels greater than the laboratory reference range.
Number of abnormal urinary test results shortly after (first round) and at least 10 months (second round) after subjects, aged 16–65, left their homes when compared to the HSL reference range
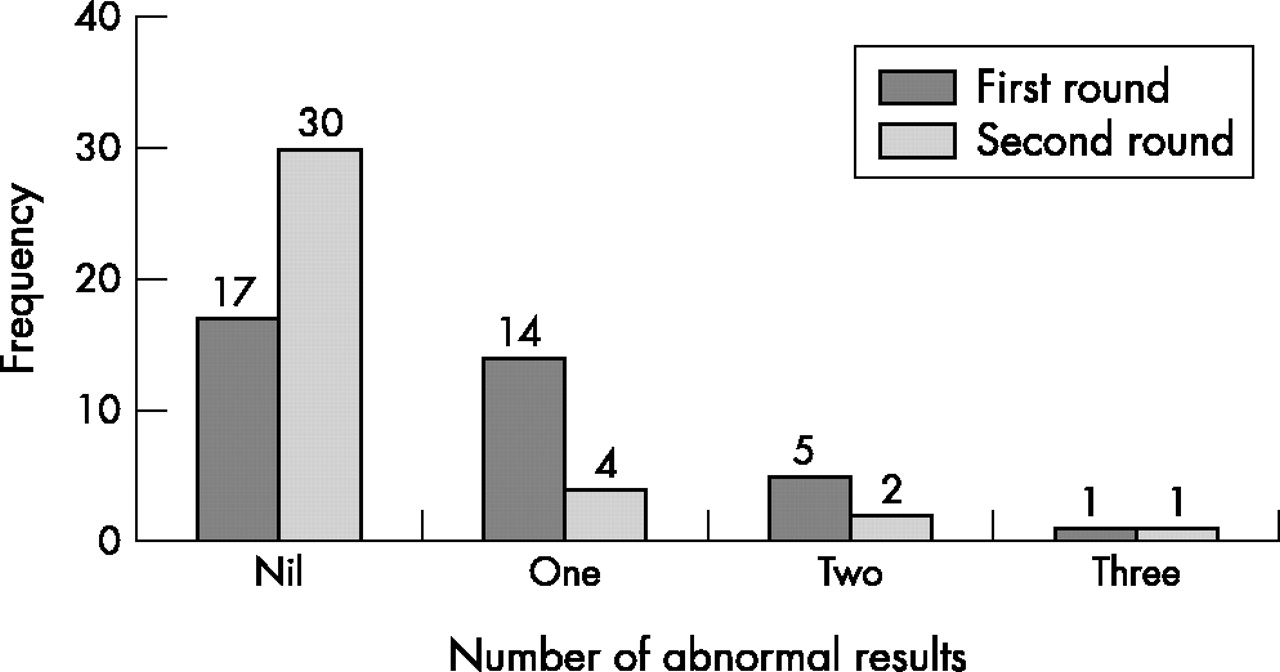
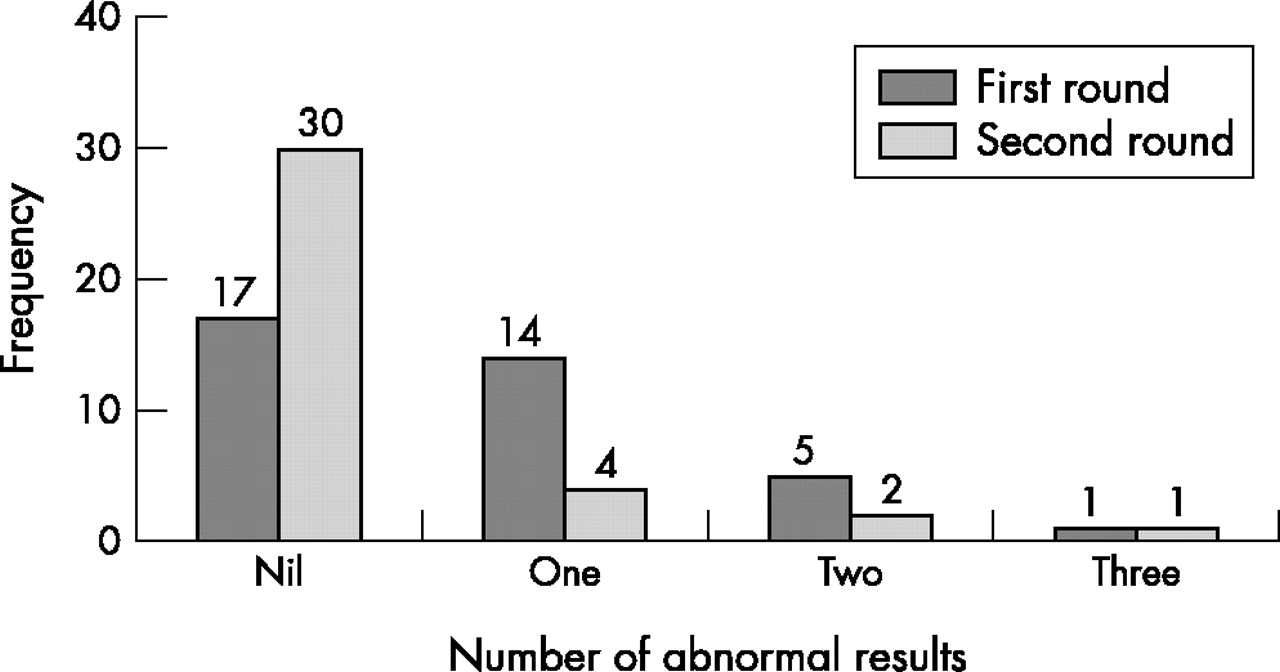
Figure 2 shows the number of subjects, aged 16–65, with a given number of raised proximal tubular markers when compared to the HSE laboratory’s reference population. In the first round of tests 20 (54%) had at least one abnormal result, and six (16%) had two or more raised values. At follow up, the number of subjects with at least one abnormal result had reduced to seven (19%). This again shows that the proximal tubular effects improved when the residents left the homes.
{kind=link}
{kind=link}
Comparison of number of abnormal proximal tubular markers (table 2) shortly after (first round) and at least 10 months (second round) after subjects left their homes (subjects aged 16–65).
DISCUSSION
This longitudinal study has shown that about half of the adults exposed to HCBD showed evidence of a subclinical proximal tubular effect. Similarly, about a quarter of adults displayed a distal tubular effect. We also found, on subsequent follow up, that in many cases these abnormalities improved when they left their homes. There was no evidence that glomerular function was affected.
In drawing our conclusions about the possible link between these observations and exposure to HCBD, we applied the Bradford-Hill criteria.26 The key criteria used here to consider whether HCBD exposure is linked to the renal effects observed are: (1) temporal relation; (2) specificity; and (3) biological plausibility.
A temporal relation is evident when exposure to pollution occurs before onset of effects and, depending on the nature of the effect, is followed by recovery when exposure ceases. In our investigations it has been possible to show the latter part of this relation.
As stated above, the urinary enzyme analyses employed in this investigation do not specifically test for the toxic effects of HCBD. It is possible, though we believe unlikely, that the proximal tubular effect is related to exposure to other chemicals from the quarry or from a nearby petrochemical complex.
These results are consistent with the predicted toxicological effects of HCBD from animal investigations. As the application of these tests is also consistent with biological models, it is highly plausible that these findings are related to exposure to this substance.
The distal effect is more difficult to explain because of the limited exposure assessment undertaken by the company. The site specific toxicity of HCBD in rats is dependent on the restriction of the enzyme β-lyase to the proximal tubular cells.8 This enzyme is responsible for the production of the reactive electrophile trichlorovinyl-chlorothioketene. The distal tubular effect is unlikely to be caused by this compound travelling from the proximal to distal tubule, in the tubular fluid, as it reacts with surrounding tissue far too rapidly. It has been shown that β-lyase is present in human proximal tubular cells.27 We are unaware of any human data regarding its presence in distal tubular cells but this remains nevertheless a possibility.
Thus far, the long term effects of human environmental exposure to HCBD are unknown. Nonetheless, the renal effects noted in this study improved when exposure ceased, and so it is anticipated that the non-carcinogenic risks will be minimal. The future carcinogenic risk is unknown. This data therefore supports the residents’ choice to leave their homes, in response to the health authority’s advice that they should reduce their exposure.
To improve our understanding of the health effects of exposure to contaminated land, further study of the use of these analytical techniques in population settings is required. To this end we suggest that population and age related reference ranges for the markers of early renal effects are established. These may be applied in a cross sectional study throughout Halton to determine whether residents not exposed to chemicals from Weston Quarry, but living in this highly industrialised area, have increased results. We also suggest that longitudinal follow up studies of the exposed residents are indicated. These studies will improve both our understanding of the human toxicology of HCBD, and of these investigations themselves, so that in future we can be clearer about interpretation of results.
Land contamination exists throughout the UK. In the light of this evidence, and the government’s policy of building 60% of new housing on previously developed land, the public, planning authorities, and development agencies need to be aware of the potential health risks when considering how brownfield sites may be utilised in future.