Article Text

Abstract
OBJECTIVES To systematically evaluate the available evidence on occupational risk factors of shoulder pain.
METHODS Relevant reports were identified by a systematic search of Medline, Embase, Psychlit, Cinahl, and Current Contents. The quality of the methods of all selected publications was assessed by two independent reviewers using a standardised checklist. Details were extracted on the study population, exposures (physical load and psychosocial work environment), and results for the association between exposure variables and shoulder pain.
RESULTS 29 Studies were included in the review; three case-control studies and 26 cross sectional designs. The median method score was 60% of the maximum attainable score. Potential risk factors related to physical load and included heavy work load, awkward postures, repetitive movements, vibration, and duration of employment. Consistent findings were found for repetitive movements, vibration, and duration of employment (odds ratio (OR) 1.4–46 in studies with method scores ⩾ 60%). Nearly all studies that assessed psychosocial risk factors reported at least one positive association with shoulder pain, but the results were not consistent across studies for either high psychological demands, poor control at work, poor social support, or job dissatisfaction. Studies with a method score ⩾60% reported ORs between 1.3 and 4.0. Substantial heterogeneity across studies for methods used for exposure assessment and data analysis impeded statistical pooling of results.
CONCLUSIONS It seems likely that shoulder pain is the result of many factors, including physical load and the psychosocial work environment. The available evidence was not consistent across studies, however, and the associations were generally not strong. Future longitudinal research should evaluate the relative importance of each individual risk factor and the role of potential confounding variables—such as exposure during leisure time—to set priorities for the prevention of shoulder pain in occupational settings.
- systematic review
- shoulder pain
- risk factors
Statistics from Altmetric.com
Shoulder pain is a common problem. The prevalence of shoulder pain in the general population may be as high as 6%–11% under the age of 50 years, increasing to 16%–25% in elderly people.1 2 Inability to work, loss of productivity, and inability to carry out household activities can be a considerable burden to the patient as well as to society. Swedish insurance data show that in 1994 about 18% of total paid sick leave for musculoskeletal disorders was spent on neck-shoulder problems, which meant that the costs of paid sick leave for neck-shoulder pain were almost equal to those of low back pain.3
The number of epidemiological studies reporting on potential risk factors for shoulder pain has greatly increased in the past decade. Work related factors are assumed to play an important part in the development of shoulder pain,4 5 and many studies have been conducted in various occupational settings. The cause of shoulder pain has been considered in several reviews,4-11 but most of these either did not consider shoulder pain specifically or did not use systematic methods for the selection of papers, assessment of methodological quality, or data extraction and analysis. An elegantly conducted meta-analysis published in 1991 summarised the results of workplace ergonomic risk factors for neck and upper limb pain.7 Unfortunately, only three studies, not specifically aimed at shoulder pain, met the relatively strict selection criteria and were included in this meta-analysis.
Since 1990 many additional papers on risk factors for shoulder pain have been published. The objective of this paper was to summarise the available evidence on occupational risk factors related to physical load and psychosocial factors, and to identify methodological shortcomings to set priorities for future research on the cause of shoulder pain.
Methods
SEARCH STRATEGY
Publications were retrieved by a computerised search of Medline (1966 to September 1998), Embase (1983 to September 1998), Psychlit (1966 to September 1998) and Cinahl (1982 to September 1998), with the following keywords (MeSH headings and text words): shoulder, shoulder joint, pain, cross-sectional, cohort, case-control, determinant, predictor, risk factor, etiology, aetiology, and causative. The references of all identified relevant studies, including reviews and meta-analyses, were hand searched for additional potentially relevant publications. All publications published until September 1998 were eligible for inclusion in the review.

{kind=link}
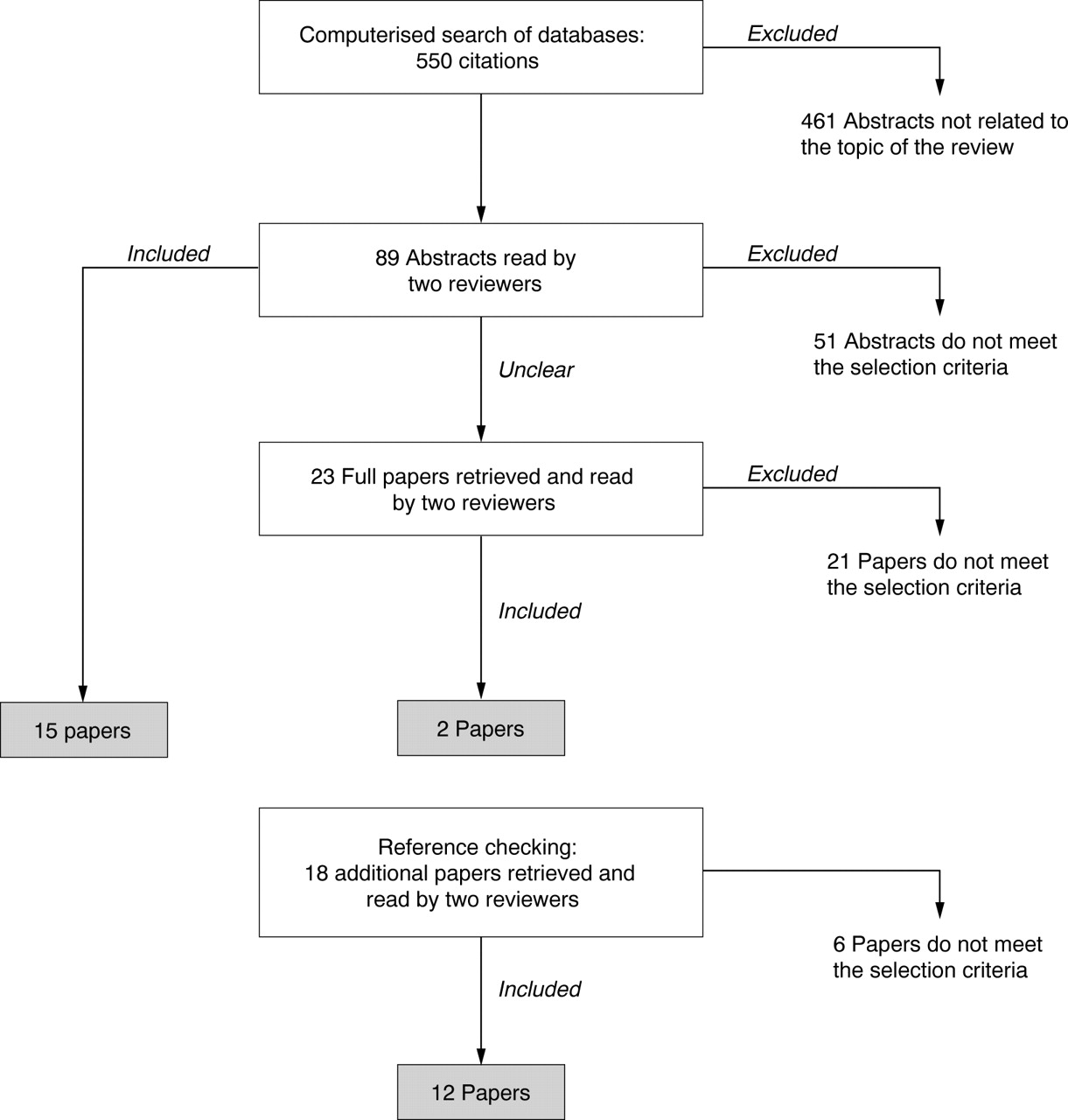
Flow diagram of papers accepted and rejected by the two reviewers during the selection procedure.
Two reviewers (DAWMW and ET) independently applied the selection criteria to the abstracts of the publications retrieved by this search strategy. Full papers were retrieved if the abstract provided insufficient information to enable selection. During a consensus meeting any disagreements about selection were resolved.
SELECTION CRITERIA
Studies were included in the review if the following conditions were met: (a) the study was a cross sectional, case-control, or prospective cohort study; (b) the paper was a full report published in English in a peer reviewed journal; (c) information was presented on physical load or psychosocial risk factors at work; (d) exposures were assessed with standardised observational methods or standardised interviews or questionnaires; (e) shoulder pain was self reported or confirmed by physical examination; (f) in studies on combined neck and upper limb pain or other pain symptoms, data on shoulder pain were presented separately. Excluded were studies on acute injuries due to trauma or sports injuries, studies that estimated exposure from job titles only, letters, and abstracts.
QUALITY ASSESSMENT
Differences in methodological quality across studies can indicate that the results of some studies are more likely to be affected by bias than others. It is important, therefore, to take the quality of a study into account when evaluating the potential causal distribution of risk factors. Two reviewers (DAWMW and ET) independently assessed the quality of each study. We used a modified version of the checklists for quality appraisal designed by Ariëns et al 12 and Hoogendoorn et al.13 Slightly different checklists were used for the quality assessment of cross sectional studies (17 items), case-control studies (21 items), and prospective cohort studies (19 items). Each item was scored as positive, negative (potential bias), or don't know (unclear) if the paper provided insufficient information on a specific item. A summary of the checklists and the conditions for scoring either positive or negative are presented in table 1.
Standardised checklist for the assessment of methodological quality of cross sectional studies (CS), case-control studies (CC), and prospective cohort studies (PC)
If the design included only an evaluation of either physical load or the psychosocial work environment, the studies were scored for the evaluated exposures; the items referring to the other dimension were scored as not applicable. Disagreements between the reviewers on individual items were identified and solved during a consensus meeting. Subsequently, method scores were computed as the total number of positively scored items over the total number of applicable items. The studies were ranked according to their total score for methodological quality (as a percentage of the maximum attainable score).
DATA EXTRACTION AND ANALYSIS
For each study we extracted details on the study population (setting, sampling frame, sample size, response rate, age, and sex), exposure to risk factors (physical load and the psychosocial work environment), and outcome (definition of shoulder pain, and the association with exposure variables in terms of relative risks or odds ratios (ORs)). Pooled risk estimates were calculated only if there was homogeneity across studies for exposure variables (type of risk factor and method of assessment) and outcome (similar case definition of shoulder pain). A random effects model was used to allow for additional heterogeneity across studies.14 15
STRENGTH OF EVIDENCE
In epidemiological studies it is not possible to establish a direct causal link between risk factors and shoulder pain. If the assocation is established in studies of relatively high quality, the strength of evidence for causality of a risk factor can be evaluated by summarising the available evidence about the following criteria: temporal relation, consistency of the association across studies, strength of the association, and biological plausibility of the association.7 9 10 16 Although none of these criteria can bring indisputable evidence for or against the cause-effect hypothesis and none can be required as an essential condition,16 they do facilitate a systematic evaluation of the literature. We defined the following (arbitrary) decision rules to summarise the strength of evidence for each risk factor of shoulder pain.
Temporal relation
Prospective cohort studies provide stronger evidence for causality than case-control or cross sectional studies.
Relatively high methodological quality
Conclusions will be based on studies with a method score equal to or higher than the median method score of all publications in the review.
Strong association
The association between the risk factor at issue and the occurrence of shoulder pain is strong (OR or risk ratio (RR) >2.0), significant (p<0.05), or a dose-response relation is established.
Consistent results
At least 75% of the studies report a strong association for the risk factor at issue.
Results
SEARCH STRATEGY
The search of the computerised databases identified a total of 550 citations. After checking for doubles, and excluding studies clearly not related to the objective of our review—for example, studies on shoulder distocia in newborn infants, traumatic injuries, pain after surgery, or complications after stroke—89 abstracts were considered in the selection procedure. Screening of the references of all relevant papers resulted in 18 additional studies. The flow diagram in the figure describes the number of abstracts accepted and rejected by the two reviewers during the selection procedure.
A total of 29 studies were finally included in the review.17-46 Of the 107 papers submitted to the selection procedure 78 were excluded, often for more than one reason: studies reporting on combined neck-shoulder pain (38 papers), no evaluation of occupational risk factors (nine papers), assessment of exposure by job title only (eight papers), no separate presentation of results on shoulder pain (seven papers), literature review (13 papers), or various other reasons (20 papers).
METHODOLOGICAL QUALITY
Only one out of the 29 studies in the review (described by two papers) was designed as a prospective cohort study.34 35However, the occupational exposures were evaluated at the same time as the occurrence of shoulder pain, and consequently, the study was included in our review as a cross sectional study.
The results of the quality appraisal are presented in table 2, separately for cross sectional (n=26) and case-control studies (n=3). For each study, the table shows the score for each individual item, the items on which the reviewers initially disagreed, and the total method score. The studies are ranked according to their total score, and in cases of equal ranking, in alphabetical order of the first author's surname. The reviewers agreed in 400 out of 480 scored items (83.3%). Disagreements often were about items 12 (assessment of occupational exposure in the past) and 13 (assessment of shoulder pain in the past). All disagreements were resolved during a consensus meeting. The median (range) method score of the cross sectional studies was 60% (43%–83%). This score of 60% was used as a cut off point to identify studies of relatively high methodological quality. The three case-control studies scored 37%, 43%, and 74%, respectively.
Results of the quality assessment of cross sectional studies and case-control studies
The following items were rated as negative in most studies: methods used for exposure assessment (items 7 and 8); assessment of important potential confounders (exposure during leisure time, item 11, or occupational exposure in the past, item 12); and presentation of data on the history of shoulder pain (item 13). Information about methods to blind assessment of exposure to the disease status was usually not provided (item 15). Only one study was assigned a positive score for this item, indicating an attempt to prevent information bias.28
STUDY CHARACTERISTICS
Table 3 presents a summary of the study characteristics, including the case definition, sampling frame, study size, and risk estimates, separately for cross sectional and case-control studies. The table presents multivariate risk estimates together with their 95% confidence interval (95% CI), and provides information on adjustments for confounding of the final statistical analysis if reported by the authors. To limit the size of the tables, only significant associations and effect estimates with relative risks or ORs >2.0 or <0.5 are presented. Additional information on the design and results of each study can be obtained from the corresponding author.
Design and results of cross sectional and case-control studies on occupational risk factors for shoulder pain
Table 3 shows that there was a wide variety across papers of study settings, exposures measured, and assessment of shoulder pain. This hampered the possibilities for statistical pooling of results, and necessitated a qualitative summary of the results. Moreover, the presentation of results on associations between exposures and the occurrence of shoulder pain was often inadequate. Some studies only presented levels of significance, without presenting estimates of risk. Adjustments for confounding were performed by several studies, but varied from stratification by sex only to the use of a multivariate model adjusting for all potential confounders. In some papers it was unclear which confounders had been included in the final model. This complicated the interpretation of the magnitude of the reported associations and ruled out sensible statistical pooling.
PHYSICAL LOAD
The wide variety of physical work load factors were grouped into the following categories: heavy physical load (14 studies); awkward postures, including twisted postures, working with forward flexed trunk, and working with arms above shoulder level (13 studies); repetitive movements (eight studies); conducting the same activity for a prolonged period—such as typing or driving a car—(five studies); vibration (six studies); and duration of employment (10 studies). Table4 gives a qualitative summary of the available evidence for these categories. The table presents the number of studies on each risk factor, the proportion of studies reporting positive associations (consistency of findings), a summary of the strength of the association, and the median method score for studies that either did or did not report positive findings.
Summary of the strength of evidence of risk factors for shoulder pain
As nearly all studies adopted cross sectional designs, a temporal relation between occupational risk factors and shoulder pain has, as yet, not been established. It must also be noted that some risk factors were evaluated by a few studies. In studies with relatively high method scores (method score ⩾60%), consistent positive associations (at least 75% positive findings) were reported for repetitive movements,17 26 44 vibration,18 23 and duration of employment.19 22 24 Working in awkward postures and conducting similar work for a prolonged period (typing) were also found to be associated with shoulder pain in most studies, but mainly in studies with relatively low method scores.
The reported strength of the associations varied widely (ORs 1.4–46), and was difficult to interpret due to the previously mentioned variation in definition and assessment of exposures, outcomes, and methods used for analysis and presentation of data. The quality of the available evidence was not impressive for most risk factors, with median method scores for positive findings between 47% and 62%. Noteworthy is the finding that for heavy physical load, awkward postures, and for conducting similar activities for long periods, the methodological quality was higher for studies that were unable to confirm the association than for the studies that did report positive results.
Many studies evaluated additional, more specific job characteristics that do not fit within the categories mentioned already—for example bricklaying and rock blasting in the construction industry,23 type of ward in nursing,21scaling in dental hygienists,19 or lancing (cleaning air vents in the furnace of a pulp and paper mill).38 These factors rarely showed a positive association with shoulder pain. Finally, the influence of the work environment was evaluated by Popeet al.45 Hot, cold, damp, and noisy conditions seemed to be associated with an increased occurrence of shoulder pain (range of RR 2.2–6.4).
PSYCHOSOCIAL WORK ENVIRONMENT
Psychosocial risk factors may be related to psychological demands at work (mental stress, job pressure, 14 studies); control at work (participation in job decision making, influence on work schedule, 11 studies); social support at work (from coworkers and supervisors, 12 studies); and job satisfaction or stimulus at work (work content, monotonous work, career prospects, 12 studies). In the last category we also included the concept investigated by Hales et al 25; fear of being replaced by computers.
Nearly all studies that included an assessment of the psychosocial work environment reported positive findings for at least one specific risk factor. The summary of evidence presented in table 4, however, shows that consistent positive findings (at least 75% positive outcomes) were not found for any of the four categories. The reported strength of the associations seems to be moderate, with the range of ORs 1.3–2.0 for most associations. Larger risk estimates were reported for poor job control,17 and for job dissatisfaction.25 43The quality of the available evidence seems to be fairly good for job control, with a median method score of 68%. However, median method scores were also relatively high for studies that were unable to show a positive association between shoulder pain and psychological work demands, job control, and social support. Noteworthy may be the fact that three of the four good quality studies that reported positive associations for job control had defined shoulder pain as symptoms with an onset during the current job,17 22 24 whereas only one of the studies with negative findings had made that distinction.26 This finding may increase the strength of evidence for job control as a risk factor for shoulder pain.
Discussion
This systematic review evaluated the results of 29 studies on occupational risk factors for shoulder pain. Variables related to both physical load and the psychosocial work environment were associated with the occurrence of shoulder pain. The review found substantial heterogeneity across studies for study setting, exposures measured, methods of exposure assessment, statistical analysis, and data presentation. This heterogeneity impeded sensible statistical pooling of results, and hence, a qualitative summary was undertaken. The available evidence was not consistent for most risk factors, not of generally high methodological quality, and the strength of the associations was modest.
The strengths of associations were difficult to interpret due to the heterogeneity across studies, but also due to the use of the OR in most cross sectional studies. The prevalence of shoulder pain was often high, which reduces the reliability of the OR as an estimate of the relative risk, and results in an overestimation of the magnitude of the association.21 45 Only a few studies have considered these difficulties and have presented relative risks or prevalence rate ratios instead of, or as well as ORs.21 27 29
QUALITY APPRAISAL
All items of our methodological checklist received equal weight. This has the disadvantage that studies with only few, but very important flaws, may still be ranked among the best studies. The three highest ranked studies, for example, did not receive positive scores for response rate (item 4),17-19 which may be considered to be an important aspect of methodological quality. Readers who consider certain items to be particularly important may use the information from tables 2 and 3 to conduct their own sensitivity analyses. The same holds for the cut off point we used to identify studies of relatively good quality (the median score of 60%), and our definition of consistency of findings (75%).
A few items did not discriminate well among studies, and could be omitted from the checklist. For example, item 1 (description of research objective) scored positive in almost all studies. A few other items were also not very useful in identifying high quality studies, as they were rated negative for most studies. These items (11,12,13, and 15), however, may represent important potential flaws. Future studies should aim to prevent these shortcomings, although that may be difficult to achieve—for example, blinding of assessment of exposure to disease status.
VALIDITY OF THE STUDIES IN THE REVIEW
Exposure during leisure time or occupational exposure in the past were often not evaluated. These variables are important potential confounders of the association between current occupational exposures and shoulder pain. The most important limitation of research to date, however, is the lack of longitudinal research, which makes it difficult to establish whether the risk factors appraised actually preceded the occurrence of shoulder pain. Temporality may be considered to be the only valid criterion for causality.48 Cross sectional studies with a case definition that includes only symptoms with an onset during the current job (table 3) may, therefore, be preferred to cross sectional studies that do not seem to check whether the exposure actually preceded the onset of shoulder problems.
Information bias can result from differential or non-differential misclassification and can accordingly influence the estimate of the strength of the association. Information bias can only be prevented by attempting to blind assessment of exposure to disease status or vice versa. These measures were rarely taken by the studies included in the review. Finally, cross sectional studies have a potential risk for survivor bias (healthy worker effect). Workers who develop shoulder pain may have left the workplace or selected different jobs, which may not be accounted for in cross sectional designs.7 This phenomenon will tend to underestimate the magnitude of an association. Ohlsson et al 40 for example, showed that for younger subjects the odds of having shoulder pain increased considerably with the duration of employment, whereas for older workers there was no significant change with duration of employment. Among the reasons that may explain this discrepency is survivor bias—that is, the selective leaving of workers with shoulder pain, and healthier subjects remaining in the job.
Longitudinal research is costly and may be a challenge to the investigator. Monotonous jobs or jobs with high work loads may have a high turnover of personnel, with difficulties tracing workers who have left the job. Work conditions and exposures may alter during the study, complicating the interpretation of results. Nevertheless, the development of improved methods of exposure assessment and the availability of user friendly statistical software for the analysis of longitudinal data, will facilitate the design and conduction of high quality prospective cohort studies on occupational risk factors for shoulder pain.
CAUSES OF SHOULDER PAIN
It seems likely that shoulder pain is the result of a concerted action of many factors, including individual factors, physical work load factors, and the psychosocial work environment. Several authors have proposed multifactorial models to explain the aetiology of musculoskeletal problems, and more specifically shoulder pain.9 11 49 50 Increased levels of muscle activity with few periods of low activity (micropauses) during awkward and static postures, and during repetitive movements, may result in shoulder pain.51-53 Psychosocial factors seem to be important in both the development and maintenance of subacute and chronic problems. Pain behaviour may be learned over time and may eventually cause the pain problem to persist even after physical healing has occurred. In this model pain is considered to be more than a neurophysiological entity, having both cognitive and behavioural dimensions.49 A poor social work environment, together with an inadequate personal capacity to cope with these factors, may increase work related stress. The increase in stress may increase muscle tone directly, or strengthen the relation between physical work load and musculoskeletal symptoms. This may result in an enhancement of the perception or reporting of symptoms, or a reduction of the capacity to cope.9 11
CONCLUSIONS AND RECOMMENDATIONS
In summary, both physical load and the psychosocial work environment seem to be associated with shoulder pain. However, the available evidence was not consistent for most risk factors, not of generally high quality (method score ⩾60% in 14 out of 29 studies), and the associations were generally not strong. In studies of relatively good methodological quality, however, consistent positive associations were found for repetitive movements, vibration, duration of employment, and to a lesser extent, job dissatisfaction.
Study of the aetiology of shoulder pain still faces many challenges for the assessment of exposure, development of adequate case definitions, and in particular, the design of longitudinal research. Prospective cohort studies that evaluate new and current employees for musculoskeletal symptoms and provide periodical follow up assessments, will provide valuable information on temporal and dose-response relations. To establish the relative contribution of each risk factor and the role of potential confounding variables, studies should evaluate not only physical work load factors and the psychosocial work environment, but also exposures in the past and during leisure time. Such studies will provide the information needed to set priorities for the prevention of work related shoulder pain.
Acknowledgments
This study was financially supported by the Netherlands Organisation for Scientific Research (NWO), grant no. R96–173.