Article Text

Abstract
OBJECTIVES To explore relations between two estimates of exposure to inhalable flour dust, and the incidence rates (IRs) of asthma and rhinitis in bakers.
METHODS This was a retrospective cohort study among 2923 bakers. A posted questionnaire registered the disease and work history. For every year, each baker was assigned an estimate of the exposure concentration to inhalable flour dust derived from reported job-tasks and dust measurements. Exposure at onset of disease was expressed as current dust exposure concentration, and as cumulative dose of exposure to dust. A multiple Poisson regression analysis assessed the impacts of the exposure estimates on the IRs of asthma and rhinitis.
RESULTS IRs of asthma and rhinitis increased by dust concentration at onset of disease. The IR of asthma for the bakers with highest exposure (dough makers) was 7.3/1000 person-years in men and 6.5 in women and for rhinitis 43.4 and 38.5, respectively. There was a significant association between the dust concentration at onset of disease and the risk for asthma or rhinitis, but not of the cumulative exposure.
CONCLUSION The risk of asthma seemed to be increased at inhalable dust concentrations ⩾3 mg/m3 (dough making or bread forming), whereas the risk of rhinitis was increased at all concentrations ⩾1 mg/m3, indicating an increased risk in all bakery job-tasks. The risks seemed to be less dependent on the cumulative exposure dust than the inhalable dust concentrations.
- bakers
- exposure-response relations
- flour dust
Statistics from Altmetric.com
Respiratory diseases such as asthma or rhinitis may occur in bakers due to inhalation of bakery dust. Several studies report the prevalence of asthma, chest symptoms, or rhinitis in bakers.1-5 A few register based studies have assessed the incidence rates (IRs) of asthma.6-8 We have recently reported an increased incidence of self reported, physician diagnosed asthma in male bakers,9 and increased IRs of self reported rhinitis in bakers of both sexes10 in a retrospective cohort study.
Cross sectional studies show a relation between exposure to dust and prevalences of chest or nasal symptoms in bakers.1 5 11It is not clear whether the increased risks of these symptoms are related to the current exposure (at time of onset of disease) or to the cumulative dose of dust.
The objective of this paper was to study whether the IR of self reported asthma and rhinitis in bakers was related to the current exposure to inhalable dust at the time of onset of disease or to the cumulative dose of inhalable dust. Our initial hypothesis postulated that asthma and rhinitis were work related only if onset was during bakery work.
Methods
This was a study of exposure-response relations within a retrospective cohort study on the IR of asthma and rhinitis with comparison between people who had completed bakery trade school and two control groups. Information on the diseases and the exposure was obtained from a postal questionnaire.
SUBJECTS
The subjects comprised people born in 1943–72 and found in the records of all bakery classes of Swedish trade schools in 1961–89. The bakery programme usually lasted for 2 years, beginning at the age of 16. All people who completed the last year of the programme were eligible for the study. In this way 2986 people were identified.
Two reference groups were used. School controls comprised people born in 1943–72, and from the same trade schools during the same period as the bakers, but of another programme. For every 10 bakers, four referents from the same school and year were selected at random, in total 1290 people.
Ninety five bakers and school controls were not found in the population register in 1992 and were excluded from the study. Of these 12 were dead, 14 had emigrated, and three changed address at the time of the study. The register was not allowed to give the addresses of another three people, and 63 people were not located in the register, probably because of changed social security numbers or emigration without notifying authorities. After exclusions 2923 bakers remained, of whom 2226 (76%) answered the questionnaire after two reminders. For the school controls there were 931 answers out of 1258 posted questionnaires (74%).
Population controls were selected at random from the Swedish population register, stratified for sex and age. This group also comprised 1258 people of whom 930 (74%) answered the questionnaire.
The study was approved by the committee of ethics of Göteborg University and by the Swedish Data Inspectorate.
QUESTIONNAIRE
Respiratory disease
A self administered questionnaire was posted to all participants in late 1992. The questionnaire included questions on the occurrence of asthma and rhinitis. Asthma was defined as positive answers to the two questions: “Do you have or have you had asthma?” and ” If 'yes', was your asthma diagnosed by a doctor?” The two questions about nasal symptoms were: “Do you have or have you had hay fever?” and “Do you have or have you had other nasal symptoms than hay fever (a blocked or runny nose and/or attacks of sneezes without having a cold)?” Rhinitis was defined as a positive answer to the last question. Affirmative answers to any of the questions on asthma or rhinitis were followed by a question about when the disorder started. There were also questions on hand eczema and atopy. The estimated IRs for asthma, rhinitis, and hand eczema have been reported elsewhere.9 10 12
The reliability of the questions on doctor's diagnosed asthma and on rhinitis was satisfactory with κ coefficients 0.90 and 0.66, respectively.9 10 A test of the reliability of the temporal aspect of onset of asthma and rhinitis showed that 47 of 65 people with asthma reported onset within 2 years when answering the questionnaire on two occasions. The corresponding figures for rhinitis were 29 out of 42 people.
Task grouping and exposure assessment
The former bakery students were questioned for bakery work from the time of graduating from trade school to the end of 1992. There were six preselected bakery job-tasks; dough making, bread forming, confectionery work, oven work, packing, and management work. A job period was defined as employment in a specified bakery. For each job period the bakers were asked to report every job-task with duration of >1 hour a day. Thus, from one up to six tasks could be reported. The exposure was assessed for each combination of job-tasks.
In a previous paper we reported measurements of inhalable dust from a random sample of Swedish bakeries.13 That study aimed at characterising exposure to inhalable dust in different exposure groups. It showed that job-task was the principal source of variance of dust exposure, explaining 61%–69% of total variability. There was large variation within each task group with geometric SDs around 2. This indicated that the number of exposure groups should be low to avoid too much overlapping between groups. From that study and experiences from working conditions in bakeries, three exposure concentrations were distinguished; 1, 3, and 6 mg/m3 for the different combinations of reported job-tasks. The 1 mg/m3 category included confectionery, packing, management, and oven work. The 3 mg/m3 category comprised bread forming as the only task, bread forming together with one or more other task (except dough making), and dough makers who reported two or more other tasks. The 6 mg/m3 category comprised dough making only or dough making together with one additional task.
For every calendar year each person was classified into one of the three current exposure categories (1, 3, or 6 mg/m3) if he or she worked in a bakery. According to the initial hypothesis he or she was in the null category if he or she did not work in a bakery irrespective of previous exposure. The cumulative dose of flour dust for a person in a calendar year wasΣiCi, whereC is the estimated inhalable dust concentration of the exposure category (1, 3, or 6 mg/m3) and i is the number of years from the calendar year of graduating from the school to the end of the calendar year of observation.
In the analysis of the association between current exposure and incidence of asthma or rhinitis, the baker's exposure in the calendar year of onset of the respective disease was used.
ANALYSES
The IRs were calculated as the number of new cases of asthma or rhinitis respectively, per person-years of observation. For the IRs 95% confidence intervals (95% CIs) were calculated assuming a Poisson distribution. The person-years for the bakers and the school controls were calculated from the year of graduating from the trade school programme. The population controls contributed with person-years from 18 years of age, the age at which most bakers finished school. If asthma or rhinitis occurred before 18 years of age or if the starting year of any disorder was unknown, the subject was excluded from the analyses. For bakers the IRs were studied separately according to current exposure or cumulative dose of inhalable dust. The observation period was from the calendar year of graduating from the school until onset of disease or to the end of 1992. From the cumulative exposure calculations three different exposure groups were established: 1–9, 10–29, and ⩾30 (years×mg/m3). Each group was represented by their arithmetric mean cumulative dose of inhalable dust (four in the 1–9 group, 16 in the 10–29 group, and 47 years×mg/m3 in the ⩾30 group).
The association between IRs during bakery work and current exposure or cumulative dose of inhalable dust and sex was analysed with a multiple Poisson regression analysis in log linear models, with the GLIM package. p Values are two tailed.
Results
The mean age in 1992 and smoking habits were similar in bakers and controls (table 1).
Number of people, age, and smoking habits in bakers and controls
As previously reported,9 10 the IRs nearly doubled for asthma in men and for rhinitis in both sexes during bakery work, compared with other work (table 2).
Incidence rates (number of cases/1000 person-years) (95% CIs) of asthma and rhinitis in bakers, school controls, and population controls, and number of cases/sum of person-years
The IR of asthma in men increased during bakery work by current exposure at time of onset from 0.5 to 7.3 cases/1000 person-years (fig1, p for trend=0.0010). There was no significant increase in IR by current exposure in women (p=0.60). However, there were only eight incident cases of asthma in women: and only one in the 6 mg/m3 group.
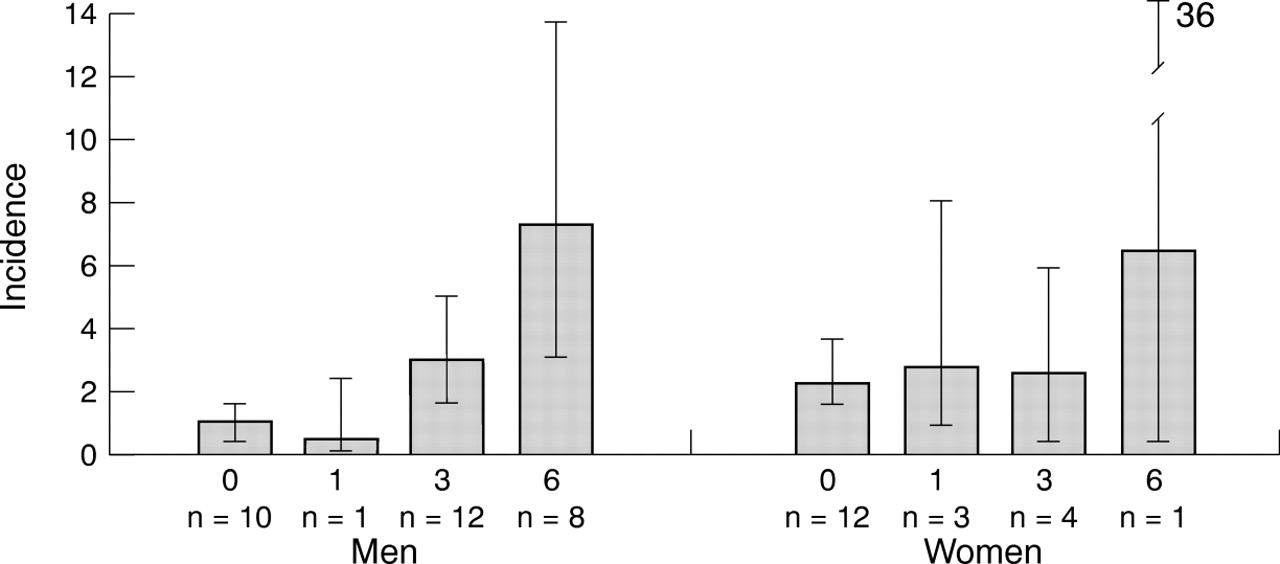
The IRs (95 % CIs) of asthma (number of cases/1000 person-years) in bakers relative to the current exposure to inhalable dust at time of onset of asthma. Current exposures were 1, 3, or 6 mg/m3. Zero class was included for comparison only. The number of cases differs from table 2 due to missing information on job-task.
The IR for asthma in men increased from 2.3 to 4.8 cases/1000 person-years by cumulative dose (fig 2). However, the test for trend was not significant (p=0.15). In women, the increase was from 2.0 in the 1–9 group to 5.5 in the 10–29 group but there were no cases in the ⩾30 group (p for trend=0.82).

The IRs (95% CIs) of asthma (number of cases/1000 person-years) in bakers relative to the cumulative dose of inhalable dust at time of onset of asthma. Cumulative doses of flour dust were 1–9, 10–29, or ⩾30 years×mg/m3. Zero class was included for comparison only. The number of cases differs from table 2due to missing information on job-task.
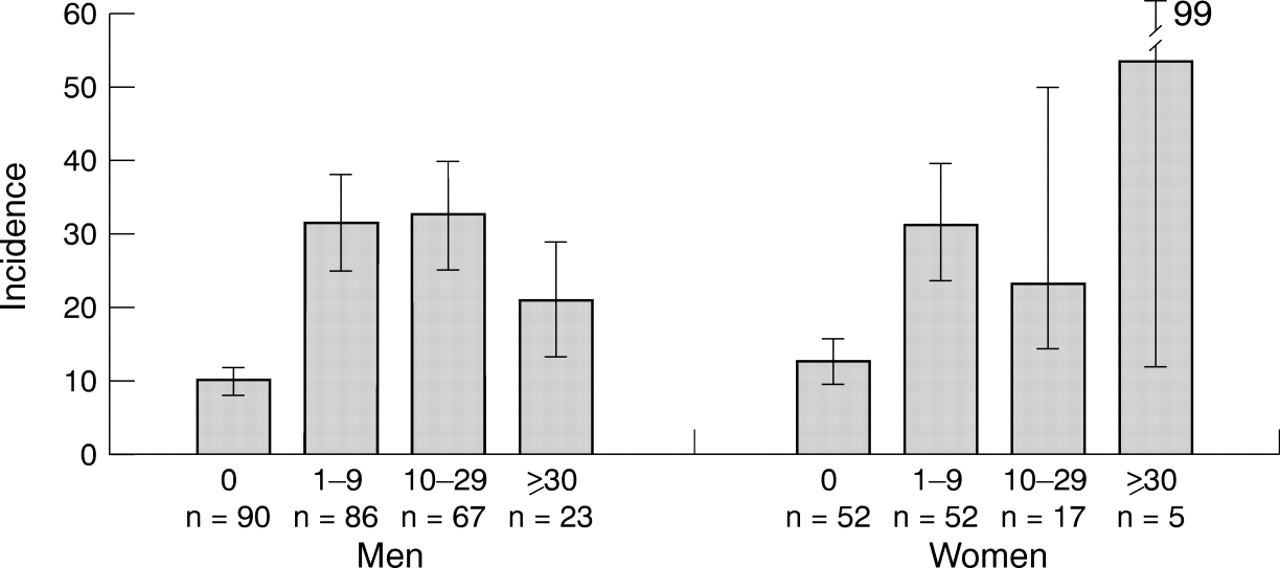
The IR of rhinitis increased by current exposure at time of onset from 18.8 to 43.4 cases/1000 person-years in men (fig 3, p for trend=0.0004) and from 29.6 to 38.5 cases/1000 person-years in women (p for trend=0.65).

The IRs (95% CIs) of rhinitis (number of cases/1000 person-years) in bakers relative to the current inhalable dust exposure at time of onset of rhinitis. Current exposures were 1, 3, or 6 mg/m3. Zero class was included for comparison only. The number of cases differs from table 2 due to missing information on job-task.
There were no significant increases in IRs of rhinitis by cumulative dose at onset, either in men (negative coefficient, p for trend=0.09), or in women (p for trend=0.48, fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The IRs (95% CIs) of rhinitis (number of cases/1000 person-years) in bakers relative to the cumulative dose of inhalable dust at time of onset of rhinitis. Cumulative doses of flour dust were 1–9, 10–29, or ⩾30 years×mg/m3. Zero class was included for comparison only. The number of cases differs from table 2 due to missing information on job-task.
In the multiple analyses including sex, current exposure, and cumulative dose of dust there were significant associations between inhalable dust concentration at onset and the IRs of asthma (p for trend=0.003) as well as of rhinitis (p for trend <0.00001). There was no positive relation between cumulative dose of dust and asthma or rhinitis (p for trend=0.70 for asthma, and a negative coefficient with p=0.03 for rhinitis) or sex (p for trend=0.09 for asthma, and 0.26 for rhinitis).
Discussion
Our study indicated that the current exposure of inhalable flour dust at the time of onset of disease was associated with the risk of contracting self reported asthma or rhinitis in bakers, whereas the cumulative dose of dust seemed less important.
VALIDITY
Our diagnoses of asthma and rhinitis were based on posted questionnaires. Definitions of asthma often include clinical features of the airways such as reversible narrowing, hyperresponsiveness, and inflammation.14 15 As clinical tests are cumbersome to use, self administered questionnaires have been used extensively in epidemiological settings.16-18 Questionnaires usually ask for “physician diagnosed asthma” and this definition of asthma was adopted in our study.
The validity of self reported asthma in questionnaires has been estimated in several studies, as reviewed by Torénet al.19 The sensitivity varies between 48% and 100%, but the specificity is high, especially for the question about “physician diagnosed asthma” (specificity ⩾99%).14 As asthma is a rare disease, a high specificity is important, otherwise the true number of people with asthma are swamped with false positives, attenuating the risk estimate.20
The validation of self reported rhinitis is hampered by the lack of an agreed definition.21 Our questionnaire asked for a combination of nasal symptoms (sneezing, runny nose, and blocked nose), without having a cold, which is in agreement with a proposed definition of rhinitis for epidemiological use.22 Sibbald and Rink23 reported a good agreement between a posted questionnaire on self reported rhinitis and in depth interviews. The sensitivity was 96% and the specificity 91%, with the interviews as the gold standard.
The reliability of the time of onset of asthma and rhinitis was satisfactory, as reported previously.9 10
The IRs were similar in bakers working in other occupations and in controls (table 2), indicating that information bias dependent on the dichotomy of exposure versus no exposure was unlikely among the bakers. A previous analysis showed that atopy, defined as a family history of hay fever, was an effect modifier of rhinitis among the bakers.10 If people with atopy avoided dusty environments the risks could have been underestimated. The prevalence of people with a family history of hay fever with any exposure to 1, 3, or 6 mg/m3 was 15.9%, 15.8%, and 14.5%, respectively.
As this was a nation wide retrospective cohort study it was not feasible to perform dust measurements in the bakeries of the participating bakers. The assessment of dust exposure during bakery work is based on self reported bakery job-tasks, inhalable dust measurements in bakeries, and experiences of working conditions in bakeries. Our measurements showed job-task to be a predictor of the exposure variability.13 Other studies report similar results and grouping strategies.1 24 25 As the exposure of dough makers might depend on short term high exposure, we reanalysed the exposure data. The mean of samples with sampling times <2 hours was 8 mg/m3 and the mean of samples with sampling times >2 hours was 6 mg/m3. The difference was not significant.
Most of the bakers of the present study worked in small or middle sized bakeries (<11 bakers working at the same time) between 1975 and 1992. Dust measurements in such bakeries in the 1980s showed concentrations similar to our measurements.13 We found that there were no substantial changes in how often flour and dough were manually handled in these bakeries during this period. Therefore, the estimated exposure to flour dust of Burdorf et al 13 was extrapolated to the entire observation period.
The bakers were not aware of our classification of exposure in the different tasks. It seems unlikely that a baker with a disorder would report a dustier task at the time of onset than healthy workers, so recall bias was improbable. However, there was a considerable variability in exposure within the different task-groups and some misclassification of exposure was probable. As such misclassification was based on task and not on outcome it was probably random, most likely attenuating an exposure-response relation.
We decided initially that the highest exposure category should include 5 years in dough making—30 year×mg/m3. The second category was primarily chosen to be half of the highest category, but the distribution of person-years and incident cases was very skewed towards low exposure. We therefore used 10 mg×years/m3 as the lower limit for the second category. The sensitivity of the grouping strategy of cumulative exposure was examined by classifying the material in categories of 5 mg/m3×year, 1–4, 5–9, 10–14, etc, including sex in the model. The multiple regression analyses did not indicate a significant association between cumulative exposure and asthma (p=0.08), but a negative association with rhinitis (p=0.02)—that is, a decreasing incidence of rhinitis with increasing dose.
SEX DIFFERENCES
We have previously reported an increased incidence of asthma in male bakers, but not in women.9 For rhinitis, there was a relative risk of about 2 in both sexes.10 In the present study there were no significant associations between exposure and rhinitis or asthma in the analysis restricted to women. However, women had in general a lower exposure than did the men, with few person-years in highly exposed groups. In multiple analyses including both men and women, there were no significant differences between the sexes. Furthermore, we are not aware of any mechanistic theory that explains why women should have a different risk from men at similar exposure to bakery dust. In our view, the most probable explanation of the sex differences, was low statistical power due to few female person-years in highly exposed groups.
CURRENT EXPOSURE OR CUMULATIVE DOSE?
The multiple analysis considering current and cumulative dose of flour dust simultaneously, favoured the hypothesis that the risk of asthma due to inhalation of flour dust was more closely associated with the current exposure at the time of onset rather than with cumulative dose (table 3). However, the two exposure estimates are correlated; of the 14 men with asthma with a cumulative dose of dust >10 years×mg/m3, six had a current exposure of 6 mg/m3 at the time of onset of disease and the remaining eight had 3 mg/m3. As an example, the correlation between current and cumulative exposure was calculated for the last year of exposure or onset of rhinitis, whichever came first. A moderate correlation was indicated (Pearson coefficient of correlationr=0.44, p<0.001). This correlation between the exposure estimates may explain the apparent association between cumulative dose of flour dust and incidence of asthma in men in figure2.
Association (coefficients (95% CIs)) between current or cumulative exposure to dust and asthma or rhinitis according to Poisson regression analysis
The cumulative exposure was calculated on the basis of more information (reported work task, duration of work tasks, and estimated dust concentrations) and was more prone to be biased towards a no exposure-response relation than the current exposure.26Furthermore, a grouped based exposure assessment was used for the cumulative dose of dust, probably giving a less biased but attenuated exposure-response relation.27 Hence, there were several possible explanations for the absence of a cumulative dose-response relation.
It was indicated that a current exposure of ⩾3 mg/m3 was associated with an increased risk of asthma (figure 1). The incidence of rhinitis was about doubled at a current exposure of 1 mg/m3 compared with non-exposed bakers or controls (table2). This may indicate that nasal symptoms were induced at lower air concentrations of flour dust than asthma. This is plausible as most airborne flour dust particles are large enough to be deposited in the nose.28 29 Hence, the nasal mucosa is exposed to more inhaled flour dust per surface unit than the lower airways.
Our initial hypothesis was that work related asthma or rhinitis in bakers had onset only during exposure, and this was supported by the comparisons with the reference groups (table 2). The hypothesis has impact on the calculation of cumulative dose of dust, and we reperformed the Poisson regression analyses considering all time after entering bakery work. This approach gave less association between IRs and cumulative dose of flour dust than considering time as an exposed baker. This favours our initial hypothesis that bakers' asthma and rhinitis start during exposure.
WHICH BAKERY JOB-TASKS ARE DANGEROUS?
Male bread formers and dough makers ran increased risks for contracting asthma. Due to limited statistical power, the risk for women performing those tasks was not well established. The same uncertainty applied for bakers of both sexes during other job-tasks. All kinds of bakers ran increased risk for rhinitis. Apart from exposure to the highest mean concentrations of flour dust in bakeries, dough making also entails high peak exposures of short (minutes) duration30 and exposure to fungal α-amylase enzyme with sensitising properties.31 These exposures may also be of importance to the risk for contracting airway disease. Our results are in line with the conclusions of Houba et al 32 that inhalable dust concentrations in bakeries should be reduced to about 0.5 mg/m3.
Conclusion
Swedish bakers, mainly working in the 1970s and 1980s, ran increased risks of rhinitis in all kinds of job-tasks. Male bakers working as bread formers or dough makers also had increased risk for asthma. The risk for asthma and rhinitis was increased by current exposure to dust at the onset of disease. This indicates that mean concentrations of inhalable dust should be <1 mg/m3 to prevent rhinitis and <3 mg/m3 if only asthma is considered. Furthermore, the risk of asthma or rhinitis is less dependent on the cumulative dose of inhaled dust than on current exposure to dust.
Acknowledgments
This work was supported by the Swedish Council for work life research, the Swedish Asthma and Allergy Foundation and the Vårdal Foundation.