Article Text

Abstract
Objectives To evaluate if higher cumulative occupational hand force requirements are associated with higher risks of surgery for trapeziometacarpal osteoarthritis and with surgery earlier in life.
Methods The study was based on Danish national registers. Among all persons born in Denmark 1931 to 1990, we included those who had been employed for at least 5 years since 1991 by the end of 2000, or later when this employment criterion was reached, up until the end of 2016. Cumulative exposure estimates for 10-year time windows (force-years) were assessed by combining individual year-by-year information on occupational codes with an expert based hand-arm job exposure matrix. First-time events of surgery for trapeziometacarpal osteoarthritis 2001 to 2017 constituted the outcome. Surgery rates were analysed by a logistic regression technique equivalent to discrete survival analysis using a 1-year lag. We also calculated rate advancement periods.
Results A total of 2 860 448 persons contributed with around 48 million person-years of follow-up, during which 3977 cases appeared (821 among men and 3156 among women). Compared with <5 force-years, the adjusted OR (ORadj) for ≥5 to <10 force-years was 1.39 (95% CI 1.14 to 1.68) and for ≥10 to 30 force-years 1.47 (95% CI 1.26 to 1.71) among men and 1.64 (95% CI 1.50 to 1.78) and 1.29 (95% CI 1.16 to 1.43) among women. The sex combined ORadj were 1.59 (95% CI 1.47 to 1.72) and 1.36 (95% CI 1.25 to 1.48). Among the exposed, surgery was advanced by 3 to 7 years.
Conclusion Medium/high cumulative hand force requirements were associated with elevated hazard rates of surgery for trapeziometacarpal osteoarthritis and advanced the time of surgery by several years.
- musculoskeletal
- osteoarthritis
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Trapeziometacarpal osteoarthritis (TMO) is a common condition, especially in women, but the evidence for a relationship to occupational exposures is limited.
What are the new findings?
Higher cumulative hand force requirements at work are associated with higher hazard rates of surgery for TMO for both men and women and advance the time of surgery for TMO by several years.
How might this impact on policy or clinical practice in the foreseeable future?
The results support preventive efforts to reduce occupational hand force requirements and may even help pave the way for future recognition of workers’ compensation claims regarding TMO.
Introduction
Trapeziometacarpal osteoarthritis (TMO), diagnosed as degenerative changes of the joint on plain radiographs, is a common condition.1 Symptoms of TMO include pain from the joint, especially during forceful hand and pinch grips, which may worsen to include pain at rest, but the severity of degenerative changes on radiographs does not correlate with clinical symptoms.2 3 When non-surgical treatment (eg, modification of activities, splinting or intraarticular steroid injections) is no longer sufficient with respect to symptoms, surgical treatment may be indicated, typically in the form of simple trapeziectomy,4 trapeziectomy with ligament reconstruction and/or tendon interposition (LRTI)5 6 or total joint arthroplasty.7
TMO is more prevalent among women and with advancing age.8 Whether persons employed in certain occupations have higher risks of developing TMO is unclear. Reviews from 20149 and 201810 showed that occupational risk factors for TMO had only been studied in few and small original studies, where most were characterised by cross-sectional designs and self-reported exposure estimates; no prospective cohort studies were identified. The reviews concluded that there was limited or insufficient evidence for a relationship between occupational exposures to the hand and TMO. Since then, a Swedish case-control study has shown an association between researcher-assessed physical demands of work and physician-diagnosed TMO,11 and a Danish register-based cohort study has shown an association between cumulative repetitive wrist movements according to a job exposure matrix (JEM) based on measured angular velocity and a hospital discharge diagnosis of TMO or surgery for TMO.12 The extent to which surgery for TMO occurs earlier in life in patients with higher occupational exposures to the hand has not been examined. If exposure-response relationships can be established between cumulative exposures to the hand and TMO, this would enhance our opportunities to understand disease mechanisms and point to potentials for prevention. Such results might even have implications for recognition of TMO as an occupational disease.
This study addressed the hypothesis that higher cumulative occupational hand force requirements are associated with higher risks of surgery for TMO and with surgery earlier in life for both men and women.
Material and methods
Design and population
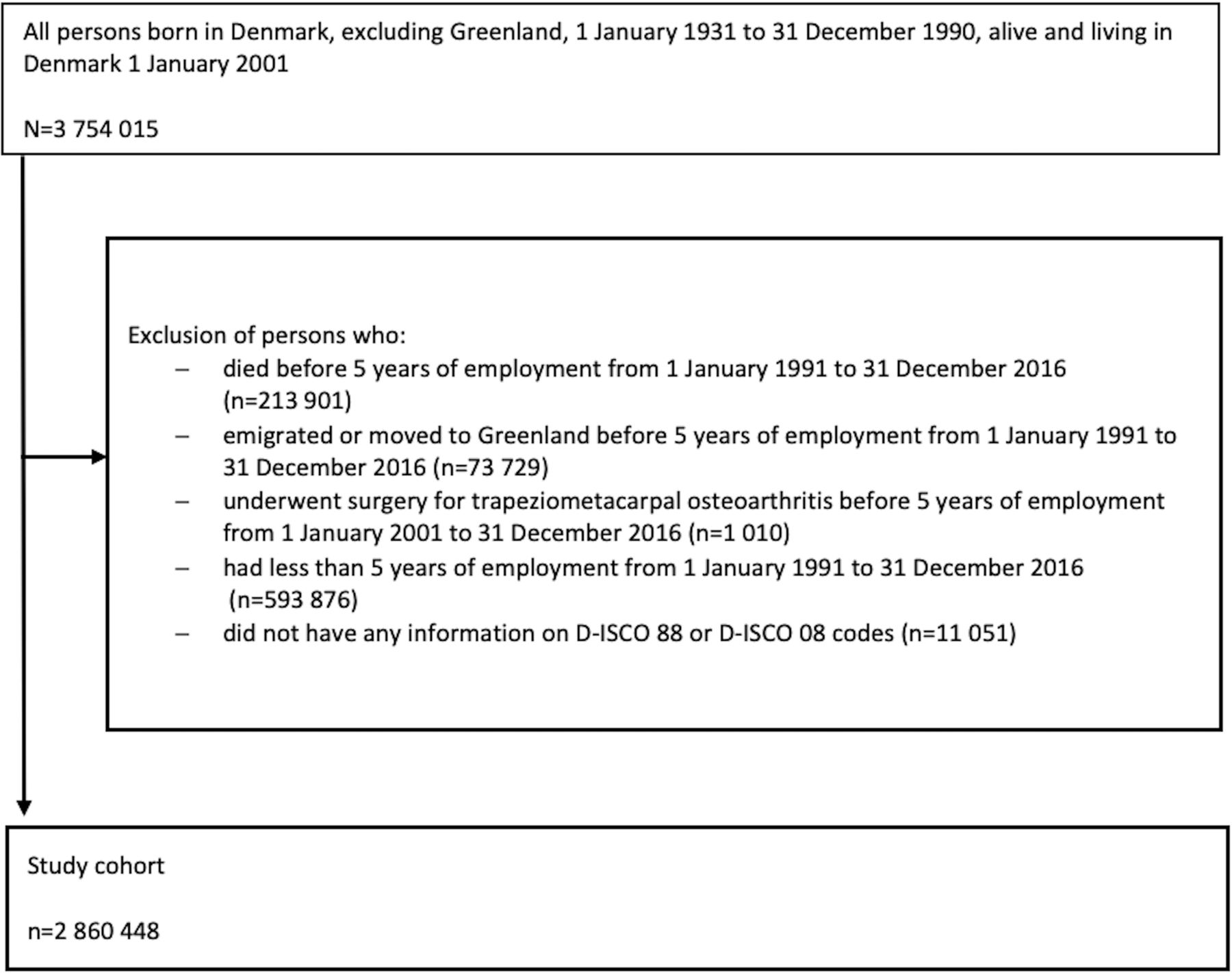
We conducted a nationwide cohort study by linkage of data from Danish national registers with a JEM.13 The cohort comprised all persons born in Denmark, excluding Greenland, between 1 January 1931 and 31 December 1990, who were alive and lived in Denmark on 1 January 2001 according to the Civil Registration System.14 We excluded persons who died, emigrated or moved to Greenland, and persons who underwent surgery for TMO before fulfilling our employment criterion of at least 5 years of employment between the ages of 20 and 70 in the period 1 January 1991 to 31 December 2016 according to the Employment Classification Module (ECM).15 Persons who did not fulfil the employment criterion and persons without any occupational codes at all (see below) were also excluded from the cohort. In Denmark, approval by health research ethics committees and patient consent are not required for register-based studies.
Outcome
The outcome was defined as the first event of surgery for TMO as registered in the Danish National Patient Register16 17 from 1 January 2001 to 31 December 2017 with a diagnostic code of TMO according to the International Classification of Diseases, 10th revision (DM18.0 to DM18.9) and with a surgery code of trapeziectomy, trapeziectomy with LRTI or total joint arthroplasty according to the Danish version of the Nordic Medico-Statistical Committee Classification of Surgical Procedures (KNDG02, KNDG12, KNDB80). Data from both public and private hospitals were included.
Exposure
From the ECM, we obtained occupational codes according to the Danish version of the International Standard Classification of Occupations from 1988 to 2009 (D-ISCO 88) and from 2010 to 2016 (D-ISCO 08) for each job held since 1 January 1991; we also obtained an employment code (BESKST13) which made it possible to distinguish between years with and without employment. Cumulative exposure estimates for 10-year time windows were assessed by linking individual year-by-year information on employment status and D-ISCO 88 or D-ISCO 08 codes to a JEM. The construction of the hand-arm JEM has been described previously.13 In short, the JEM was based on five experts’ ratings of occupational mechanical exposures for all occupational titles in Denmark, divided into 169 groups of occupational titles with similar exposure profiles. Using a 5-point scale, forceful work (intensity of exertion) was scored as 0 (light), 1 (somewhat hard), 2 (hard), 3 (very hard) and 4 (near maximal).18 The score was a measure of the mean force used during a typical working day, and accordingly the near maximal score did not appear in the JEM. The JEM was later translated to occupational D-ISCO 88 and D-ISCO 08 codes. Exposure estimates of zero were used for years outside the labour market. If D-ISCO codes were missing for cohort members in years of employment, the mean exposure for all the person’s years with information on D-ISCO codes was used to replace the missing exposure estimates. The estimates of cumulative occupational exposures were expressed as force-years in accordance with the pack-year concept of cumulative tobacco consumption.19 One force-year was defined as having worked for 1 year with a force-score of 1.
Covariates
Covariates comprised sex (in sex combined analyses), age, administrative region (based on zip codes) to account for any regional differences in access to surgery for TMO and calendar year. Data from the ECM included year-by-year information on socioeconomic status (SOCIO13 with six levels) based on a person’s main income in the year. For every person we applied the socioeconomic status code that was used most often in the period 1991 to 2016.
Statistical analyses
Incidence rates were calculated as the number of first-time events of surgery for TMO divided by the number of person-years at risk. The correlation between force-years and age was calculated in terms of the Spearman correlation coefficient. We analysed the risk of surgery using a logistic regression technique equivalent to discrete survival analysis, yielding ORs with 95% CIs. The ORs may be interpreted as HRs.20 Models with time-varying exposures and a 1-year lag time were applied. Thus, the force-year estimates were calculated for the 10-year time period up to and including the year before the calendar year in question both for those who underwent surgery for TMO in that particular year and for those who were still at risk but did not undergo surgery for TMO that year. Follow-up began on 1 January 2001 for persons registered with at least 5 years of employment since 1 January 1991. For persons registered with less than 5 years of employment by 1 January 2001, follow-up began the year after the person had accumulated 5 years of employment up until 31 December 2016. Persons were followed until surgery for TMO, censoring due to death, disappearance or emigration/moving to Greenland, the person’s 70th birthday or 31 December 2017, whichever came first. The full model comprised three categories of force-years (low: <5, medium: ≥5 to <10 and high: ≥10 to 30; we thought that cumulative exposures <5 force-years would be negligible and chose the cut-off between the medium and high categories so that the remaining person-years were divided approximately equally), sex, age (continuous and time-varying), administrative region (n=5, time-varying) and calendar year (continuous); socioeconomic status was not included in the main analysis due to expected correlation with the exposure variable.
In supplementary analyses, we calculated force-years for the more remote and the more recent 5 years of each 10-year exposure time window and included these variables together in the adjusted model to evaluate if remote exposures did in fact play a role, which would indicate cumulative effects. Analyses restricted to employees at intermediate or basic level were also performed. These levels were defined by SOCIO13 codes 133 (intermediate level), which corresponds to D-ISCO 08 major group 3 (technicians and associate professionals) and 134 (basic level), which comprises D-ISCO 08 main groups 4 to 8 (4 clerks, 5 service workers and shop and market sales workers, 6 skilled agricultural and fishery workers, 7 craft and related trades workers and 8 plant and machine operators and assemblers). The SOCIO13 groups were selected to represent a wide range of exposures, while minimising confounding by socioeconomic status.
We calculated rate advancement periods (RAPs) with 95% CI using adjusted coefficients and variance estimates from the logistic regression analyses.21 RAPs describe how much earlier in life a given outcome occurs with increasing exposure. The accelerated occurrence (number of years) is calculated as the ratio between the regression coefficient for the exposure and the regression coefficient for an increment of 1 year of age. Calculation of RAPs requires that the risk of the outcome increases uniformly with age, which is the case for TMO in the included age interval.3 We calculated sex separate RAPs as the ratio between the adjusted regression coefficient for each force-year category (≥5 to <10 and ≥10 to 30) and the adjusted regression coefficient for age.21 RAPs were also calculated for men and women together. Analyses were performed on Statistics Denmark’s research platform using Stata V.15.1 (StataCorp, College Station, Texas, USA).
Results
The formation of the study cohort is shown in figure 1. The cohort consisted of 2 860 448 persons, 1 474 352 men and 1 386 096 women. The most frequent D-ISCO codes (D-ISCO 88 and D-ISCO 08 codes combined) with force requirements ≥1.5 were ‘carpenters and joiners’, ‘construction and maintenance labourers’ and ‘agricultural or industrial machinery mechanics and fitters’ for men and ‘wood and related product assemblers’, ‘butchers, fishmongers and related food preparers’ and ‘construction and maintenance labourers’ for women. Characteristics of the person-years of follow-up are shown in table 1. Men were increasingly over-represented with increasing force-years. In 8% of the observed person-years, missing exposure values were imputed.

{kind=link}
Flowchart.
Characteristics of the 48 333 440 person-years of follow-up within the study cohort of 2 860 448 persons
A total of 3977 first-time events of surgery for TMO were identified during follow-up, 821 among men and 3156 among women (2001 to 2006: 375 surgeries, 2007 to 2012: 1598 and 2013 to 2017: 2004). This corresponded to incidence rates of 0.3/10 000 person-years for men and 1.4/10 000 person-years for women. Force-years and age were only weakly correlated (Spearman correlation coefficient=0.0054) so it was possible to disentangle the effects of force-years and age. Table 2 shows sex specific ORs of surgery for TMO in relation to force-years and age. Analyses including both men and women showed that female sex (ORadj 4.36; 95% CI 4.03 to 4.72), increasing age (ORadj 1.08 for an increment of 1 year; 95% CI 1.07 to 1.08) and force-years ≥5 (≥5 to <10: ORadj 1.59; 95% CI 1.47 to 1.72 and ≥10 to 30: ORadj 1.36; 95% CI 1.25 to 1.48) were associated with higher odds (hazard rates) of surgery for TMO.
Sex specific crude and adjusted ORs of first-time surgery for trapeziometacarpal osteoarthritis (TMO) in relation to cumulative occupational hand force requirements (force-years) and age
In analyses of the more remote and the more recent 5 years in each exposure time window—mutually adjusted for each other, sex and age—the adjusted ORs for the more remote 5 years were 1.30 (95% CI 1.15 to 1.46) for ≥2.5 to <5 force-years and 1.08 (95% CI 0.93 to 1.25) for ≥5 to 15 force-years compared with <2.5 force-years. For the more recent 5 years the adjusted ORs were 1.33 (95% CI 1.18 to 1.50) for ≥2.5 to <5 force-years and 1.25 (95% CI 1.07 to 1.45) for ≥5 to 15 force-years compared with <2.5 force-years. Thus, exposures accrued both back in time and recently were associated with higher hazard rates of surgery. Analyses restricted to employees at basic or intermediate level showed adjusted ORs of 1.49 (95% CI 1.35 to 1.65) for ≥5 to <10 force-years and 1.42 (95% CI 1.27 to 1.59) for ≥10 to 30 force-years compared with <5 force-years.
Table 3 shows sex specific RAPs in relation to force-years. Surgery for TMO occurred several years earlier in the medium and high force-year categories than in the low force-year category among both men and women. Sex combined RAPs were 6.2 (95% CI 5.1 to 7.3) and 4.1 (95% CI 2.9 to 5.3).
Sex specific adjusted regression coefficients and rate advancement periods (RAPs) for surgery for trapeziometacarpal osteoarthritis in relation to cumulative occupational hand force requirements (force-years)
Discussion
Higher cumulative occupational hand force requirements were associated with an elevated risk of surgery for TMO with ORs in the order of 1.5 but the results did not indicate a clear exposure-response relationship, particularly not among women. Surgery for TMO occurred several years earlier in relation to medium and high cumulative hand force requirements.
A strength of the present study was that it was based on nationwide longitudinal registers with near-to-complete coverage. The JEM-based exposure assessment removed any risk of recall bias due to overestimation of occupational exposures by persons with hand complaints. Moreover, the JEM has shown good predictive validity in studies of neuropathy of the ulnar nerve13 22 and clinically suspected scaphoid fracture.23 It may be considered a limitation that JEMs inherently assign the same exposure estimate to all persons in the same job group irrespective of within-group exposure variations. However, the risk estimates will—in general—not be biassed by this misclassification of exposure, while the precision of the risk estimates will be reduced.24 The force-scores in the hand-arm JEM do not specifically concern the thumb, but medium/high force exertions with the hands/arms will require forceful hand grips involving the thumb since the thumb must resist the combined force of the other fingers during grasp.25
We focussed on hand force requirements because previous studies have suggested that forceful hand and pinch grips play a role for TMO.9 Additionally, it has been shown that a load of 10 kg in hand grip produces compression forces of around 120 kg in the trapeziometacarpal joint, while a load of 1 kg in pinch grip produces joint compression forces of around 12 kg.25 Other occupational hand exposures, including hand-arm vibrations and repetitive movements of the thumb may have been differentially distributed across the categories of force-years in our study, which may have confounded our results to the extent that these exposures are also risk factors for TMO. Different occupational mechanical exposures to the hand often occur in combination, which makes it difficult to disentangle effects of specific exposures. Our force-year estimates may have captured combined effects of several exposures, but in any case, the results point to the existence of relationships between occupational mechanical exposures and TMO. To the extent that repetitive work occurred together with low hand force requirements, we may even have underestimated the relationships. Likewise, the relatively high OR in the middle force-year category among women might have to do with combinations of medium force requirements and repetition, particularly among women.
Previous findings among dentists compared with teachers have suggested that hand use may increase the risk of hand pain given radiographic osteoarthritis.26 This raises the question whether the relationship that we found between force-years and surgery for TMO can be regarded as causal or if high exposures only aggravated TMO-related symptoms and thereby led to an increased probability of surgery. In the latter case, however, we would not expect to find a relationship with force-years accrued during the more remote 5 years in each 10-year exposure time window. Thus, the results may not be explained by aggravation, but point to a causal relationship.
Cumulative exposure estimates equal the mean exposure intensity multiplied by the exposure duration. Our cumulative force-year variable was calculated for fixed exposure time windows of 10 years, that is, the exposure duration was constant. This means that we could not really distinguish between true cumulative effects and effects of exposure intensity. Therefore, we performed supplementary analyses, where we included force-years for the more remote and the more recent 5 years of each 10-year exposure time window in the same model. The fact that exposures accrued in both 5-year periods were associated with higher ORs of the outcome indicates that the elevated ORs of surgery for TMO were due to cumulative effects of high hand force requirements.
A given number of force-years could be accrued through long durations of low hand force requirements or short durations of high hand force requirements. With a view to preventive interventions, insight into the maximum hand force requirements, which could be endured for prolonged periods without an increased risk of clinically significant TMO, would be valuable. To that end, an obvious way to proceed would be to apply a new analytical approach which was recently developed to identify safe exposure intensities.27
Our outcome definition did not include hospital discharge diagnoses of TMO. This means that we may have underestimated the relationship under study to the extent that current high hand force requirements were associated with a lower probability of surgery given the same severity of TMO. According to our experience, surgery was used more cautiously in case of high hand force requirements during the earlier years of follow-up, meaning that we reduced (but probably did not eliminate) this potential source of bias by adjusting for calendar year in the analyses. There may be a social gradient with a tendency for comorbidity and manual work to co-occur. However, comorbidity is not very likely to influence the decision for or against surgery for TMO, especially not before the age of 70. Additionally, socioeconomic differences in access to surgery are minimised by a public and tax-paid healthcare system in Denmark. We did not adjust for socioeconomic status in our main analyses because we thought that this would lead to over-adjustment. However, sensitivity analyses restricted to employees at basic or intermediate level showed results like the main analyses. This indicated that socioeconomic status was not an important confounder of our results. Moreover, it is still unclear if there is any association between TMO and lifestyle factors such as body mass index, smoking and alcohol consumption,28 29 which may be associated with socioeconomic status.
To our knowledge, the present study is the third large scale epidemiological study based on independent exposure estimates that has been performed since the reviews9 10 mentioned in the introduction. The previous Danish cohort study12 included around 30% of the population in the present study so the results cannot be considered entirely independent. On the other hand, the outcome definition in that study differed from ours in that it included hospital discharge diagnoses of TMO in addition to surgery for TMO, and the exposure in focus was repetitive work. In that way, the two studies complement each other, and they agree with the results of the Swedish case-control study with physical demands as the exposure and physician-diagnosed TMO as the outcome.11 Jointly, these three studies indicate a moderate increase in risk of TMO in relation to occupational mechanical exposures to the hand and therefore add to the existing weak evidence of a relationship. If we are right that the reported associations represent a causal relationship, interventions to reduce high hand force requirements may prevent more cases of TMO than indicated by our results regarding surgeries, which only represent the tip of the iceberg. Such interventions will most likely also contribute to preventing other upper limb disorders including carpal tunnel syndrome, which seems to share risk factors with TMO. We found that surgery for TMO occurred several years earlier in relation to high cumulative hand force requirements for both men and women. This is a new finding which suggests that the preventive potential may be larger than indicated by the moderate increase in risk.
In conclusion, the results supported our hypothesis that the risk of surgery for TMO is elevated in relation to higher cumulative occupational hand force requirements for both sexes and thereby added to the existing weak evidence of a relationship. We also found indications that higher hand force requirements lead to surgery for TMO earlier in life.
Acknowledgments
We acknowledge Sorosh Tabatabaeifar, MD, PhD, for converting the hand-arm JEM to D-ISCO 88 and D-ISCO 08 codes.
References
Footnotes
Contributors All authors took part in the planning and design of the study. LK, with the help of PF, performed the statistical analyses. LK wrote the first draft of the manuscript. All authors contributed to the interpretation of the results, revision of the manuscript and final approval of the manuscript. All authors take responsibility for integrity of the work as a whole.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Danish Data Protection Agency (j.no. 1-16-02-523-16).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data from the hand-arm JEM are available upon reasonable request. Data from the Danish national registers are available through online access at Statistics Denmark under standard conditions.