Article Text

Abstract
Objectives To describe the health burden among Fire Department of the City of New York (FDNY) emergency medical service (EMS) workers and examine its association with work at the World Trade Center (WTC) disaster site.
Methods In this observational cohort study, we used FDNY physician diagnoses to estimate the cumulative incidence of physical health conditions including rhinosinusitis, gastroesophageal reflux disease (GERD), obstructive airways disease (OAD) and cancer among EMS workers and demographically similar firefighters who were active on 11 September 2001 (9/11). Validated screening instruments were used to estimate the prevalence of probable post-traumatic stress disorder (PTSD), probable depression and probable harmful alcohol use. We also analysed the association between health conditions and WTC-exposure.
Results Among 2281 EMS workers, the 12-year post-9/11 cumulative incidence (11 September 2001 to 31 December 2013) of rhinosinusitis was 10.6%; GERD 12.1%; OAD 11.8%; cancer 3.1%. The prevalence of probable PTSD up to 12 years after exposure was 7%; probable depression 16.7%; and probable harmful alcohol use 3%. Compared with unexposed, EMS workers who arrived earliest at the site had higher adjusted relative risks (aRR) for most conditions, including rhinosinusitis (aRR=3.7; 95% CI 2.2 to 6.0); GERD (aRR=3.8; 95% CI 2.4 to 6.1); OAD (aRR=2.4: 95% CI 1.7 to 3.6); probable PTSD (aRR=7.0; 95% CI 3.6 to 13.5); and, probable depression (aRR=2.3; 95% CI 1.6 to 3.1).
Conclusions In this 12-year study, we documented a high burden of health conditions associated with WTC-exposure among FDNY EMS workers. These findings underscore the importance of continued monitoring and treatment of this workforce.
- World Trade Center
- Health Burden
- EMS Workers
- Cumulative Incidence
- Relative Risks
Statistics from Altmetric.com
What this paper adds
The health effects of the World Trade Center (WTC) disaster have been well-documented among rescue/recovery workers in general, and firefighters and police officers in particular.
Little is known, however, about the health impact of WTC on emergency medical service (EMS) workers.
In this first study to focus on Fire Department of the City of New York EMS workers, we found that the 12-year post-9/11 cumulative incidence of physical health conditions ranged from 12.1% for gastroesophageal reflux disease (GERD) to 3.1% for cancer; the prevalence of mental health conditions up to 12 years after exposure was 16.7% for probable depression and 7% for probable post-traumatic stress disorder (PTSD).
Compared with those who never worked at the WTC site, EMS workers who arrived earliest at the site had higher adjusted relative risks for nearly all health conditions, including nearly four times the risk for GERD and seven times the risk for probable PTSD.
Our findings demonstrated that the burden of disease over the 12-year study period was substantial, underscoring the need for continued monitoring and treatment of EMS workers.
Introduction
After the 11 September 2001 (9/11) World Trade Center (WTC) attacks, tens of thousands of individuals participated in the rescue and recovery effort at the disaster site. Rescue and recovery workers included first responders—firefighters, police officers and emergency medical service (EMS) workers—as well as operating engineers, iron workers, railway tunnel workers, sanitation workers, utility workers, and volunteers.1 Previous research has documented an array of WTC-related physical and mental health issues among these workers including: excess cancer risks;2–4 elevated rates of aerodigestive illnesses such as asthma5 or gastroesophageal reflux disease (GERD);6 and, increased risks of post-traumatic stress disorder (PTSD),7 depression,8 and frequent binge drinking.9 Substantial comorbidities between these health conditions were also found.10 ,11 While a number of studies have investigated the effects of the WTC disaster on rescue and recovery workers in general3–6 ,11–13 and Fire Department of New York (FDNY) firefighters2 ,8 ,14–16 and New York City (NYC) police officers17–20 in particular, no studies have focused on the effects in EMS workers.
EMS workers, a group including both paramedics and emergency medical technicians, face demanding work environments. Studies to date on EMS workers have analysed occupational injuries,21–23 general health24 and mental health states.25 ,26 Little is known, however, about the effects of a large-scale disaster on EMS workers.
In this 12-year study, covering the period 11 September 2001 through 31 December 2013, we focused on EMS workers’ disease burden by examining selected physical and mental health conditions that are certified as WTC-related conditions under the James Zadroga 9/11 Health and Compensation Act of 2010.27 Specifically, we aim to: (1) describe the post-9/11 cumulative incidence of WTC-related physical health conditions and the prevalence of probable mental health conditions, including comorbidities, among FDNY EMS workers and (2) assess the associations between WTC-exposure and health outcomes. In addition, we performed a secondary analysis of certified WTC-related conditions in a subset of demographically comparable FDNY EMS workers and FDNY firefighters to contextualise the post-9/11 burden in FDNY EMS workers. To date, most epidemiological studies on WTC-exposed cohorts have been limited by the use of self-reported physician diagnoses to estimate disease prevalence.11 ,13 We and others, however, have found substantial variability between self-reported physician diagnoses and diagnoses obtained from medical records.28–30 Given our full access to the FDNY electronic medical record system, we have taken advantage of this unique opportunity to investigate these aims using confirmed physician diagnoses.
Methods
Starting in 1996, the FDNY Bureau of Health Services (FDNY-BHS) transitioned from paper records to an electronic medical record system. On March 17 of the same year, FDNY assumed responsibility for operating NYC's EMS ambulance system from the NYC Health and Hospitals Corporation. Subsequently, relevant background and medical information from all EMS workers was incorporated into the FDNY-BHS electronic record database.
Study population
The source population consisted of 2973 EMS workers who were active (ie, not retired) on 9/11. We excluded participants who did not consent to have either their physical or mental health information used for research (n=659) and those who had unknown or missing WTC-exposure (n=33). The present analysis focuses on the final analytic cohort of 2281 EMS workers.
Data sources
FDNY-BHS and its WTC Health Programme (WTCHP) schedule monitoring evaluations every 12–18 months for active and WTC-exposed retired FDNY responders and provide separate treatment care, as necessary. Monitoring visits include physician examinations and since 2001, self-administered health questionnaires. In December 2005, separate mental health questionnaires were added to the evaluation.
We used questionnaire data to describe participants’ WTC-exposure, smoking status and mental health symptoms. Demographic characteristics (age on 9/11, race, gender and retirement from FDNY as of the end of the study period) came from the FDNY employee database. Physical attributes (measured height and weight) were recorded at the monitoring visits. We obtained FDNY physician diagnoses from the FDNY-BHS electronic medical record database.
WTC-exposure
Intensity of WTC-exposure was taken from participants’ first post-9/11 health questionnaire. We categorised exposure based on initial arrival time to the disaster site as follows: arrival on the morning of 11 September 2001 (arrival group 1); on the afternoon of 11 September 2001 (arrival group 2); on the following day, 12 September 2001 (arrival group 3); between 13 September 2001 and 24 September 2001 (arrival group 4); and after 24 September 2001 (arrival group 5).16 Among the WTC-exposed, arrival group 1 is considered to be the most exposed and arrival group 5 the least exposed. Participants who reported never being present at the site were classified as unexposed.
In addition to arrival time, job tasks performed at the WTC site were similarly obtained from participants’ first post-9/11 health questionnaire.
FDNY physical health diagnoses
To describe the post-9/11 cumulative incidence of physical conditions, we reviewed participants’ electronic medical records for aerodigestive diagnoses16 of rhinosinusitis, GERD, chronic bronchitis, chronic obstructive pulmonary disorder or emphysema (COPD/emphysema), and asthma occurring before the end of the study period, 31 December 2013.
To be classified as having a confirmed physician diagnosis, participants were required to have at least two diagnoses of rhinosinusitis, GERD, COPD/emphysema and asthma documented at least 30 days apart on separate physician visits. For chronic bronchitis, we required two diagnoses within 1 year and at least one additional diagnosis within the following 3 years. Participants were classified as having obstructive airways disease (OAD) if they were diagnosed with asthma, chronic bronchitis or COPD/emphysema. For each of the aerodigestive conditions, participants with a first diagnosis date prior to 11 September 2001 were not considered to have a post-9/11 incident condition. We did not have information on the presence of these conditions prior to 17 March 1996, as FDNY-BHS began maintaining medical records for EMS workers at that time.
Cancer cases were obtained from FDNY's internal cancer registry. Information on cancer cases in the FDNY registry were acquired from two sources: most cases (N=65; 92.9%) were obtained by matches to nine state cancer registries selected to represent 98% of EMS workers’ current addresses (New York, New Jersey, Florida, Pennsylvania, North Carolina, Virginia, Connecticut, South Carolina and Arizona). Some cases (N=5; 7.1%) came from participants’ self-reports of cancer on questionnaires or during medical monitoring visits and were only included as cases when confirmed by medical records. We excluded non-melanoma skin cancers and in situ cancers with the exception of in situ bladder cancers. Only participants with a first ever diagnosis of cancer between 11 September 2001 and 31 December 2011 were included as cases of post-9/11 incident cancer, as after that date, state cancer registries were not complete.
Mental health screening
We estimated the prevalence of three mental health conditions up to 12 years after 9/11: PTSD, depression and harmful alcohol use through the use of validated screening questionnaires.31–33 As these screening questionnaires are symptoms-based and not diagnostic instruments, we qualify our findings using the term ‘probable.’ To analyse participants’ current mental health burden, we obtained results from their most recent survey taken before 31 December 2013.
Probable PTSD
We assessed probable PTSD using the PTSD Checklist (PCL)-Civilian Version,31 a 17-item questionnaire corresponding to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnostic criteria for PTSD. The PCL investigates participants’ symptoms related to a specific traumatic event (eg, ‘WTC attacks’) during the 30 days preceding their questionnaire date. Each symptom was rated on a 5-point Likert scale (1=not at all; 5=extremely); total scores range from 17 to 85. Participants with scores ≥44 were categorised as having probable PTSD.34
Probable depression
We used the Centers for Epidemiological Studies Depression Scale (CES-D), a 20-item survey that inquires about depressive symptoms to evaluate probable depression.32 Each symptom is scored on a scale from 0 to 3 (0=none or rarely (less than 1 day per week); 3=most or all of the time (5–7 days per week)), with four items that required reverse scoring. The FDNY version inquires about symptoms in the past month. We used the cut-off ≥16 to classify participants as having probable depression.
Probable harmful alcohol use
Harmful alcohol use was assessed using the Alcohol Use Disorders Identification Test (AUDIT),33 a 10-item survey that inquires about alcohol behaviours during the past year. Items are scored on a Likert scale from 0 to 4 (0=never, 4=daily or almost daily). Participants with scores ≥8 were classified as having probable harmful alcohol use.33
Statistical analyses
We compared the prevalence of pre-9/11 physical health conditions (diagnoses between 17 March 1996 and 11 September 2001) by WTC-exposure status to assess the comparability of the WTC-exposed and WTC-unexposed groups using either Pearson's χ2 test or Fisher's exact test. We also analysed demographic and other characteristics by exposure status (arrival group) and health outcomes. The post-9/11 cumulative incidence was calculated by dividing the number of individuals with a newly diagnosed health condition during the study period by the total number of individuals at risk for that condition. Cumulative incidence was estimated for rhinosinusitis, GERD, OAD in general and asthma in particular and cancer. We also described the prevalence of probable PTSD, probable depression and probable harmful alcohol use. Prevalence was estimated by dividing the number of individuals who screened positive for a mental health condition by the total study population.
For multivariable analyses, we used modified Poisson regression models with robust error variance35 to estimate the relative risks (RR) and 95% CIs for each health outcome of interest. We evaluated the following potential confounders: age on 9/11 (18–29; 30–39; 40–49; 50–65), race/ethnicity (white/non-white), gender, smoking status (ever/never) and BMI (<25; 25–29; ≥30 kg/m2). Variables were included as confounders in the final models if they were associated with both WTC arrival group and the outcome of interest. We repeated these analyses with WTC arrival group as an ordinal variable to test linear trends of an exposure–outcome association, with separate models for each health outcome.
Two secondary analyses were conducted. First, we examined the cumulative incidence and prevalence of health conditions and their associations with WTC-exposure among EMS workers who had at least one monitoring visit to FDNY-BHS in the final 2 years of the study. We did this to assess possible differential cohort attrition by WTC-exposure status.
Second, we compared findings in the EMS study population to findings in a sample of firefighters who were active on 9/11, consented to research, and had non-missing exposure information to contextualise the health burden in EMS workers. Owing to demographic differences between the two workforces, we restricted analyses to firefighters and EMS workers who were non-Hispanic white males, aged 30–40 years on 9/11 and compared the cumulative incidence, prevalence and comorbidity rates of health conditions using Pearson's χ2 test or Fisher's exact test.
All results were considered significant with p value <0.05. Analyses were conducted using SAS (V.9.4; SAS Institute Inc, Cary, North Carolina).
Results
Table 1 displays study participants’ characteristics and post-9/11 cumulative incidence and prevalence of health conditions by WTC-exposure intensity based on arrival group. Participants were primarily non-Hispanic white males, most of whom remained active in the FDNY EMS workforce as of the conclusion of the study (31 December 2013). The most commonly reported initial exposure to the WTC was during the afternoon of 9/11 (arrival group 2–25.3%); fewer than 20% of the cohort reported no work at the WTC site (n=418). The median age on 9/11 was 36.2 years (IQR=29.9–42.1). Nearly half of the participants were never smokers (49.9%); more than a third were former smokers (36.4%); and a small proportion were current smokers (13.7%).
Participant characteristics and post-9/11 cumulative incidence and prevalence of selected health conditions in the Fire Department of the City of New York (FDNY) emergency medical service study population
EMS workers who arrived earliest on 9/11 (arrival group 1) had the highest post-9/11 cumulative incidence of rhinosinusitis, GERD, OAD and the highest prevalence of probable PTSD and probable depression. GERD has the highest overall cumulative incidence (12.1%) followed by OAD (11.8%), and rhinosinusitis (10.6%). Among mental health conditions, probable depression has the highest prevalence (16.7%). Seventy participants (3.1%) had a first primary cancer diagnosis during the study period. The cumulative incidence and prevalence of most health conditions were similar between whites and non-whites, but differed by gender. Compared to males, females have significantly higher incidence of rhinosinusitis (17% vs 8.9%; p value <0.0001), GERD (17.9% vs 10.5%; p value <0.0001), OAD (20.3% vs 9.5%; p value <0.0001) and significantly higher prevalence of probable PTSD (10.4% vs 6.1%; p value=0.0011), and probable depression (23.5% vs 14.8%; p value <0.0001).
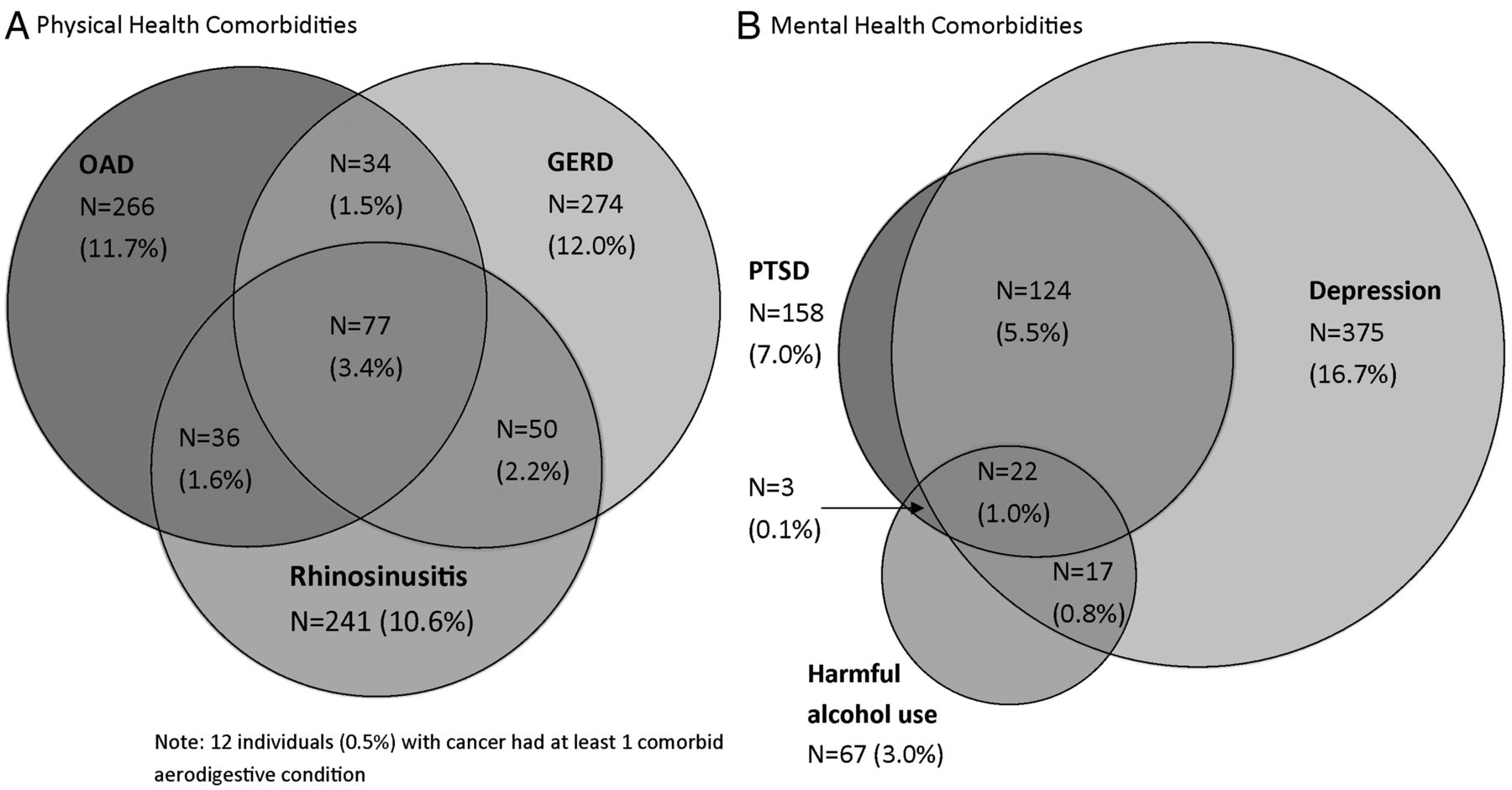
We quantified aerodigestive and mental health comorbidities in figure 1A, B, respectively. A small number of participants (8.6% of the cohort) had physician diagnoses for two or more of the three aerodigestive conditions: rhinosinusitis, OAD and GERD (figure 1A). Similarly, 7.4% of the cohort screened positive for two or more of the three probable mental health conditions: PTSD, depression and harmful alcohol use (figure 1B). We also analysed comorbidities between aerodigestive and mental health conditions. Among 412 participants who screened positive for at least one mental health condition, 145 (35.2%) also were diagnosed with at least one aerodigestive condition: 70 (17%) have rhinosinusitis; 92 (22.3%) have GERD; and 82 (19.9%) have OAD. Further, among 507 participants who were diagnosed with at least one aerodigestive condition, 145 (28.6%) also have at least one mental health condition: 65 (12.9%) participants screened positive for probable PTSD; 135 (26.7%) for probable depression; and 20 (4%) for probable harmful alcohol use.

{kind=link}
Comorbid health conditions among Fire Department of the City of New York (FDNY) emergency medical service workers by post-9/11 physical health conditions (A) and probable mental health conditions (B). (B) Does not include participants with missing mental health survey results at the end of the study period (n=34). Percentages of rhinosinusitis, GERD and OAD are calculated out of the total study population. OAD, obstructive airways disease; GERD, gastroesophageal reflux disease; PTSD, post-traumatic stress disorder.
The low prevalence of pre-9/11 physical health diagnoses was similar between WTC-exposed and WTC-unexposed EMS workers, suggesting that pre-9/11 health status did not affect the likelihood of later work at the WTC site (table 2). Therefore, unexposed EMS workers served as the reference group in all statistical models. In modified Poisson regression models with robust error variance, we evaluated the crude and adjusted associations between WTC-exposure and physical health conditions (table 3) and between WTC-exposure and mental health conditions (table 4). Compared with the unexposed, arrival group 1 had significantly higher risks for rhinosinusitis (adjusted RR=3.7; 95% CI 2.2 to 6.0); GERD (adjusted RR=3.8; 95% CI 2.4 to 6.1); OAD (adjusted RR=2.4; 95% CI 1.7 to 3.6); and asthma (adjusted RR=2.9; 95% CI 1.9 to 4.5; table 3). Subsequent arrival groups also had greater risks for aerodigestive conditions compared with the unexposed: in adjusted analyses, arrival groups 2, 3, 4 and 5 had significantly higher risks for rhinosinusitis and GERD, and arrival group 2 had significantly higher risks for OAD in general and asthma in particular (table 3).
Pre-9/11 prevalence of physical health conditions by World Trade Center (WTC) exposure status in Fire Department of the City of New York (FDNY) emergency medical service workers
Unadjusted and adjusted relative risks (aRR) for physical health conditions in Fire Department of the City of New York (FDNY) emergency medical service workers using Poisson regression
Unadjusted and adjusted relative risks (aRR) for mental health conditions in Fire Department of the City of New York (FDNY) emergency medical service workers using Poisson regression
Examining mental health conditions, arrival group 1 had significantly higher risks for probable PTSD (adjusted RR=7.0; 95% CI 3.6 to 13.5) and probable depression (adjusted RR=2.3; 95% CI 1.6 to 3.1; table 4). In crude analysis, arrival group 1 had significantly higher risks for probable harmful alcohol use, although this association became attenuated in the adjusted model and no longer remained statistically significant. After adjusting for other covariates, compared with the unexposed, arrival groups 2, 3, 4 had significantly higher risks for probable depression, and arrival groups 2, 3 and 5 had significantly higher risks for probable PTSD (table 4). The crude and adjusted associations between WTC-exposure and cancer were not statistically significant.
We repeated the above analyses with arrival time as an ordinal variable to analyse the linear trends of WTC-exposure–response associations. In adjusted analyses, we found that increased intensity of WTC-exposure was associated with significantly higher risks of receiving the following diagnoses: rhinosinusitis (p for trend: <0.0001), GERD (p for trend: <0.0001), OAD (p for trend: <0.0001), asthma (p for trend: <0.0001), probable PTSD (p for trend: <0.0001), probable depression (p for trend: <0.0001) and probable harmful alcohol use (p for trend: 0.0219).
As a secondary analysis, we restricted EMS study participants to those who had at least one monitoring visit in the 2 years before the end of the study period, to ensure that both WTC-exposed and unexposed participants had seen FDNY physicians who could have diagnosed the conditions of interest. We found that 83.2% of WTC-exposed EMS workers and 80.9% of unexposed EMS workers had a monitoring visit within the final 2 years of the study, providing evidence that the groups had similar opportunity to become diagnosed by an FDNY physician. Further, in this subgroup, the cumulative incidence of health conditions and their associations with WTC-exposure were similar to the results in our primary analyses (data not shown).
Comparisons with firefighters
In the final secondary analysis, we compared the post-9/11 cumulative incidence and prevalence of various conditions in EMS workers with the incidence in firefighters. Since there were demographic differences between the two workforces, we restricted analyses to 362 EMS workers and 4134 firefighters who were non-Hispanic white males, aged 30 to 40 years on 9/11. Compared with firefighters, EMS workers had lower cumulative incidence of nearly all conditions, with substantially fewer physician diagnoses of rhinosinusitis (8.1% vs 34.3%; p-value <0.0001); GERD (10.3% vs 29%; p value <0.0001) and OAD (9.5% vs 24.7%; p value <0.0001). Further, fewer EMS workers screened positive for probable harmful alcohol use (3.6% vs 9.3%; p value=0.0003) although the prevalence of probable PTSD, probable depression, and the incidence of cancer were similar between the groups (data not shown).
EMS workers also had lower comorbidity rates of both physical and mental health conditions. Compared with firefighters, fewer EMS workers had diagnoses of at least two aerodigestive conditions: rhinosinusitis, OAD, and/or GERD (8% vs 26.7%; p value <0.0001) and fewer screened positive for at least two of the three probable mental health conditions: PTSD, depression and/or harmful alcohol use (5.8% vs 9.8%; p value=0.0128).
To understand the differences in incidence proportions, prevalence and comorbidity rates between EMS workers and firefighters, we analysed self-reported rescue/recovery tasks performed at the disaster site on 9/11. Compared with EMS workers, substantially more firefighters reported digging on the pile at the disaster site (91.5% vs 14.4%; p value <0.0001).
Discussion
This is the first study to examine the WTC-related disease burden in FDNY EMS workers. We documented the post-9/11 cumulative incidence of physical health conditions (aerodigestive conditions and cancer) and the prevalence of probable mental health conditions (PTSD, depression, harmful alcohol use), as well as their comorbidities. WTC-exposure was significantly related to the incidence of these health conditions: we observed an exposure–response gradient based on WTC arrival group in linear models for nearly all conditions, and we found that the most intensely exposed group—those arriving during the morning of 9/11—had significantly higher risks for most conditions in Poisson models.
Since we do not know of any non-FDNY studies that use physician diagnoses from medical records to estimate the incidence of WTC-related conditions, we compared the health burden in demographically similar FDNY firefighters to the burden in FDNY EMS workers. Overall, our results demonstrated a lower burden in EMS workers. Different job tasks during the WTC rescue/recovery effort probably placed EMS workers at lower risk for developing some adverse health outcomes. Although some EMS workers and firefighters arrived at the WTC site at the same time, firefighters, on the basis of their job assignments, were at considerably higher risk for inhalation exposures. For example, considerably more firefighters than EMS workers reported digging at the disaster site, increasing firefighters’ exposures to respiratory irritants such as inorganic dust, products of pyrolysis and other respirable materials.16 EMS workers, on the other hand, were more likely to have provided emergency care and performed transport activities such as delivering patients to hospitals or bodies to morgues. Despite these differences, our study showed that within the population of EMS workers, WTC-exposure was associated with elevated risks for aerodigestive and probable mental health conditions.
Consistent with our EMS findings, previous 9/11 health studies found increased risks among WTC-exposed cohorts for aerodigestive conditions such as GERD6 and asthma,5 as well as for symptoms indicative of PTSD,7 depression,8 and harmful alcohol use.9 Unlike prior studies, ours is the first to concentrate on EMS workers, especially important as we used confirmed physician diagnoses from FDNY medical records rather than self-reports to describe the post-9/11 cumulative incidence of physical health conditions.
We found that female EMS workers have higher post-9/11 cumulative incidence for aerodigestive conditions and higher prevalence of probable PTSD and probable depression than males. Similarly, Brackbill et al36 found that more females than males screened positive for PTSD symptoms in a longitudinal cohort of individuals exposed to the WTC disaster. However, contrary to our findings, Li et al37 reported that post-9/11 gastroesophageal reflux symptoms did not differ by gender among WTC-exposed individuals. Different case definitions of GERD may have contributed to the discrepant findings.
We did not find a statistically significant association between WTC-exposure and cancer. This finding contrasts with the findings in our previous study on cancer where Zeig-Owens et al2 reported a modest excess of cancer cases in WTC-exposed firefighters compared with their unexposed counterparts. We remain cautious in the interpretation of our findings on cancer because we were likely underpowered to detect an association in the much smaller EMS population. Since we observed so few cases, we also did not calculate standardised incidence ratios for either all-sites or specific cancers. Further, we only included cancers with diagnoses dates on or before 31 December, 2011, and so the time interval since 9/11 was relatively short for cancer outcomes in our study. Over time we may observe more emergent cancers, which future studies may be better able to investigate.
This study has two primary strengths. First, we used confirmed physician diagnoses obtained directly from FDNY medical records and confirmed cancer cases rather than self-reported diagnoses to describe the post-9/11 cumulative incidence of aerodigestive conditions and cancer. We are confident in our disease estimates as self-reported diagnoses often over-report conditions, and may also be subject to recall bias.30 It is also important to note that FDNY physicians use consistent clinical criteria to diagnose health conditions, including aerodigestive conditions, thereby limiting diagnostic variations.
A second strength of this study is that the cohort was established prior to 9/11. In contrast to other 9/11 study cohorts that were assembled after the disaster, the present analytic cohort has limited selection bias as individuals cannot self-select into FDNY's WTC cohort. For this reason, we believe that we were better able to determine the health impact of the WTC disaster. We also had pre-9/11 health information on WTC-exposed and unexposed FDNY EMS workers who were active on 9/11. This information permitted us to determine that the prevalence of pre-9/11 physical health conditions was similar in unexposed EMS workers compared to their exposed counterparts, suggesting that pre-9/11 health status was not associated with WTC-exposure status (ie, unexposed EMS were not less likely to participate in WTC work because of poor health). Consequently, unexposed EMS workers were presumed to be a comparable reference group in statistical models.
Despite this study's strengths, it also has some limitations. First, we did not have access to pre-1996 diagnoses in EMS workers because data for this workforce was merged with the FDNY-BHS medical record system beginning 1996. With the exception of cancer, where we have cancer registry data, we cannot rule out exacerbations of pre-existing aerodigestive conditions diagnosed prior to 1996. Therefore, we acknowledge possible misclassification of post-9/11 incident cases of aerodigestive conditions, although this would have been non-differential by WTC exposure status.
Second, we do not have mental health symptoms information prior to 9/11. Since we could not identify the individuals who were at risk for mental health conditions at the beginning of the study period, we calculated the prevalence of probable mental health conditions instead of the cumulative incidence. We also used screening questionnaires instead of clinical diagnoses to describe the prevalence of probable PTSD, depression and harmful alcohol use. However, other studies have shown that the PCL, CES-D and AUDIT have strong performance properties including high internal consistency, convergent validity and discriminant validity.38–40 While these instruments have been validated to screen for their respective conditions, it is important to mention that the PCL and CES-D include overlapping symptom questions (eg, both ask about difficulty sleeping). Accordingly, we do not know if the comorbidity rates between probable PTSD and probable depression in our study (figure 1B) reflect clinical reasons for co-occurrence or might instead be attributed to screening overlap. Further, we acknowledge that there may be unmeasured confounders in the associations between WTC-exposure and mental health conditions. Nonetheless, we found striking relative risks for probable PTSD and probable depression: EMS workers who were present during the morning of 9/11 had nearly seven times the risk for screening positive for probable PTSD and twice the risk for probable depression compared with those who never worked at the WTC site.
Finally, we did not include information from physicians outside of FDNY-BHS, as we do not have access to their medical records. Therefore, there may be some under ascertainment of cases. Although medical diagnoses given by external physicians may be noted in participants’ FDNY medical records, we included only confirmed FDNY physician diagnoses in our case definitions of aerodigestive conditions. We believe that this had only a minimal impact on our results: most WTC-exposed participants seek care from FDNY-BHS and its WTCHP because it provides free healthcare, including free medications. We note, however, that WTC-unexposed individuals are ineligible for free FDNY care and medical monitoring after retirement. Yet, in a secondary analysis on a subset of EMS workers who had at least one monitoring visit in the 2 years before the end of the study period, we found that retention rates were similar between exposed and unexposed, and that the associations between WTC-exposure and health outcomes were similar to results from the primary analyses.
Conclusion
In summary, these study results underscore the health consequences associated with WTC-related work among FDNY EMS workers. We found that WTC-exposed EMS workers had statistically significant elevated risks for nearly all health conditions and for probable PTSD in particular, despite the fact that the cumulative incidence of these conditions was generally lower than that of firefighters. Although we failed to detect a statistically significant association with cancer cases, possibly because of the short time interval since 9/11 for cancer outcomes and insufficient statistical power in this study, we plan to investigate this association in future studies. Our findings demonstrated that the burden of disease over the 12-year study period was substantial, highlighting the need for continued monitoring and treatment of EMS workers.
References
Supplementary materials
Press release
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
Footnotes
Contributors JY, RZ-O, MPW, AK and DJP designed the study, analysed and interpreted the data. RZ-O had the initial idea for the study. JY drafted the first manuscript with critical revisions from RZ-O, MPW, AK and DJP. CBH, XL, JW, MV and TS contributed to study design, analyses and revisions of the manuscript. KJK contributed to the clinical diagnoses. All authors have approved the final manuscript.
Funding This project was supported by research grants and contracts from the National Institute of Occupational Safety and Health.
Competing interests None.
Ethics approval Institutional Review Board of Montefiore Medical Center/Albert Einstein College of Medicine
Provenance and peer review Not commissioned; externally peer reviewed.