Article Text

Abstract
Background Lung cancer incidence in Central and Eastern Europe (CEE) is among the highest in the world, and the role of occupational exposures has not been adequately studied in these countries.
Objectives To investigate the contribution of occupational exposure to polycyclic aromatic hydrocarbons (PAH) to lung cancer in CEE.
Methods A case–control study was conducted in the Czech Republic, Hungary, Poland, Romania, Russia and Slovakia, as well as the United Kingdom (UK) between 1998 and 2002. Occupational and socio-demographic information was collected through interviews from 2861 newly diagnosed lung cancer cases and 2936 population or hospital controls. Industrial hygiene experts in each country evaluated exposure to 70 occupational agents, whereof 15 mixtures containing PAH. ORs of lung cancer were calculated after adjusting for other occupational exposures and tobacco smoking.
Results The OR for ever exposure to PAH in the CEE countries was 0.93 (95% CI 0.77 to 1.14). The ORs for the highest category of cumulative exposure, duration of exposure and intensity of exposure were 1.13 (95% CI 0.80 to 1.58), 1.02 (95% CI 0.66 to 1.57) and 1.11 (95% CI 0.60 to 2.05), respectively. The OR for ever PAH exposure in the UK was 1.97 (95% CI 1.16 to 3.35).
Conclusion Occupational PAH exposure does not appear to substantially contribute to the burden of lung cancer in CEE. The apparently stronger effect observed in the UK may be due to high exposure levels and a joint effect with asbestos.
- Lung neoplasms
- polycyclic hydrocarbons
- aromatic
- occupational exposure
- Europe
- case-control studies
- epidemiology, cancer
Statistics from Altmetric.com
- Lung neoplasms
- polycyclic hydrocarbons
- aromatic
- occupational exposure
- Europe
- case-control studies
- epidemiology, cancer
Background
Polycyclic aromatic hydrocarbons (PAH) are a group of chemicals made up of two or more benzene rings interlinked in various arrangements and with different toxicological and carcinogenic properties. PAH are naturally present in fossil fuels and can be formed during incomplete combustion of any organic material, which makes them common in the environment. They are usually adsorbed on to fine particles in the air or appear as solids in soil or sediment and can enter the body by inhalation, ingestion or through the skin.1
PAH represent a major group of lung carcinogens in tobacco smoke. In addition, they are present in industrial emissions and motor exhaust, and therefore are a source of occupational exposures for significant groups of workers as well as contributing to urban air pollution.2
Several individual PAH and mixtures including PAH (eg, soot, coal-tars, diesel engine exhaust) are classified as carcinogenic or probably carcinogenic to humans by the International Agency for Research on Cancer.3 In addition, coal gasification, coke production, coal-tar distillation, paving and roofing, aluminium production and chimney sweeping, all entailing exposure to PAH mixtures, are classified as carcinogenic to humans.4 PAH exposure increases the risk of lung, skin and bladder cancer.5
Lung cancer is the leading cause of death from cancer in the world and tobacco smoking is the overwhelming risk factor in most populations.6 The incidence of lung cancer in Central and Eastern Europe (CEE) is among the highest in the world, and is also relatively high among non-smokers,7 which indicates that risk factors other than tobacco smoking, such as occupational and environmental agents, may be present.
We have investigated whether lung cancer burden in this region is influenced by occupational PAH exposure while controlling for potential confounders. We also included a companion study from the United Kingdom.
Methods
A case–control study on lung cancer was conducted during the period 1998–2002 in seven European countries. Sixteen centres were included: Borsod, Heves, Szabolcs, Szolnok, Budapest (Hungary), Lodz, Warsaw (Poland), Banska Bystrica, Bratislava, Nitra (Slovakia), Brno, Olomouc, Prague (Czech Republic), Bucharest (Romania), Moscow (Russia) and Liverpool (UK). Approvals were obtained from relevant ethics review committees.
The study population comprised all newly diagnosed lung cancer cases (age <75 years) in the participating hospitals. Population controls were selected from the electronic register of residents in Warsaw and from the general practitioner registry in Liverpool. In the other centres, controls were selected from patients admitted to the same hospitals as the cases or from general hospitals serving the same population. Patients with smoking-related conditions or other cancers were not considered eligible. No single disease represented more than 20% of the diagnoses of controls. The participation rate was above 84% in all countries except in the UK, where the participation rate was 45% among cases and 46% among controls. Reasons for non-participation were, besides not giving consent, that subjects had died, were too ill to be interviewed or had been discharged from hospital. Twenty two subjects, nine cases and 13 controls did not provide complete tobacco data and were excluded from the main analyses. A total of 2852 lung cancer cases and 2923 controls frequency matched to cases on age (±3 years) and sex were included in the analyses.
The interviews were conducted face to face and the questionnaire included a structured section concerning lifestyle and a semi-structured section for an occupational biography. All subjects provided a list of all occupations held for at least 1 year. If the job included one of 16 specific activities they also completed a specialised questionnaire. The interviewers were trained in probing in order to obtain as much information as the respondent could supply. Thereafter in each country industrial hygiene experts, blinded to the case–control status of the study subjects, assigned job (ISCO 1968) and industry codes (NACE rev. 1) and assessed whether any of 70 specific agents or groups of agents were present and noted the degree of confidence that the exposure actually occurred (possible, probable, definite). The experts also estimated the average level of exposure (low=1, medium=2, high=3) based on agent specific categories, and the frequency of exposure during a normal workweek (less than 5%, 5–30%, >30%). The definitions and cut-off levels for each exposure were provided in a coder's manual.
To model level of exposure to PAH, two indices were built: (i) duration of exposure across all job periods in years and (ii) cumulative exposure, calculated as the product of the frequency (mid-interval values of average work time: 3%, 17.5%, 65%), the intensity of airborne benzo[a]pyrene (mid-interval values: 0.075, 0.55, 3 μg/m3 estimated from quantitative measures of corresponding jobs in the literature8–10) and the duration of the exposure (years), summed over all work periods in the person's job history. The cumulative dose was categorised according to the quartiles of the exposure distribution among controls.
The experts assessed exposure to PAH directly based on the occupational questionnaires, but in most situations the level of PAH exposure was assigned to a subject according to an algorithm when any of the following 14 source exposures were indicated: soot and fumes from combustion of coal, coke, petroleum oil, wood, asphalt, coal tar and pitch, creosote fumes, diesel emissions, lubricating oil mist, cutting fluids and other mineral oil mist, carbon black dust, and plastics pyrolysis. In brief, all exposures derived from combustion of coal or coal compounds contribute high levels of PAH, exposures derived from combustion of wood and petroleum products contain medium levels of PAH and the remaining exposures (rubber pyrolysis, diesel exhausts, coke fumes, oil mists and carbon black) contribute low levels of PAH (details available upon request).
ORs of lung cancer and 95% CIs were estimated by unconditional logistic regression, adjusted for age groups (eight categories), sex, centre, tobacco pack-years ((average number of cigarettes per day×years)/20), and occupational exposure (ever/never) to silica, asbestos and metals (arsenic, chromium[VI], cadmium), which are known lung carcinogens, have a high prevalence in the study population and are frequent concurrent exposures with PAH.
Tests for linear trends were calculated using the log likelihood ratio test, comparing the model without the variable of interest with the model including the variable fitted as a continuous variable by using the mid interval value for each stratum.
Tests for heterogeneity across countries and between the CEE and the UK were calculated using the log likelihood ratio test.
Analyses were repeated with a 20-year lag, in which all jobs held within 20 years before the year of interview were considered not exposed.
The statistical package Stata 8.0 was used for the logistic regression analyses and R v 2.7.1 for the forest plots.
Results
Table 1 describes the study population with regard to sex, country, age group, tobacco smoking and relevant occupational exposures. As expected, we found a marked difference between cases and controls with respect to smoking.
Description of the study population
About 16% of men and 4% of women had experienced occupational PAH exposure. However, this prevalence varied substantially between the countries (p<0.001) including for high exposure levels (p<0.001). The majority of exposed men (57%) and almost all exposed women (92%) had been exposed only to low levels of PAH. However, 10% of exposed men had experienced high levels of PAH exposure and 32% medium levels. No woman had experienced high PAH exposure levels and 8% had experienced medium levels. All exposed subjects had at least one work period with probable or certain PAH exposure.
Among the subjects exposed to PAH, 34% were also exposed to silica, 28% were also exposed to metals (arsenic, chromium[VI] and cadmium) and 28% were also exposed to asbestos. Of the PAH exposed subjects, 11% had been exposed to asbestos and metals, and 5% had been exposed to asbestos, metals and silica.
Table 2 shows the most frequent jobs and activities in which subjects were classified as exposed to PAH.
Selected jobs and industries held by subjects classified as exposed to polycyclic aromatic hydrocarbons
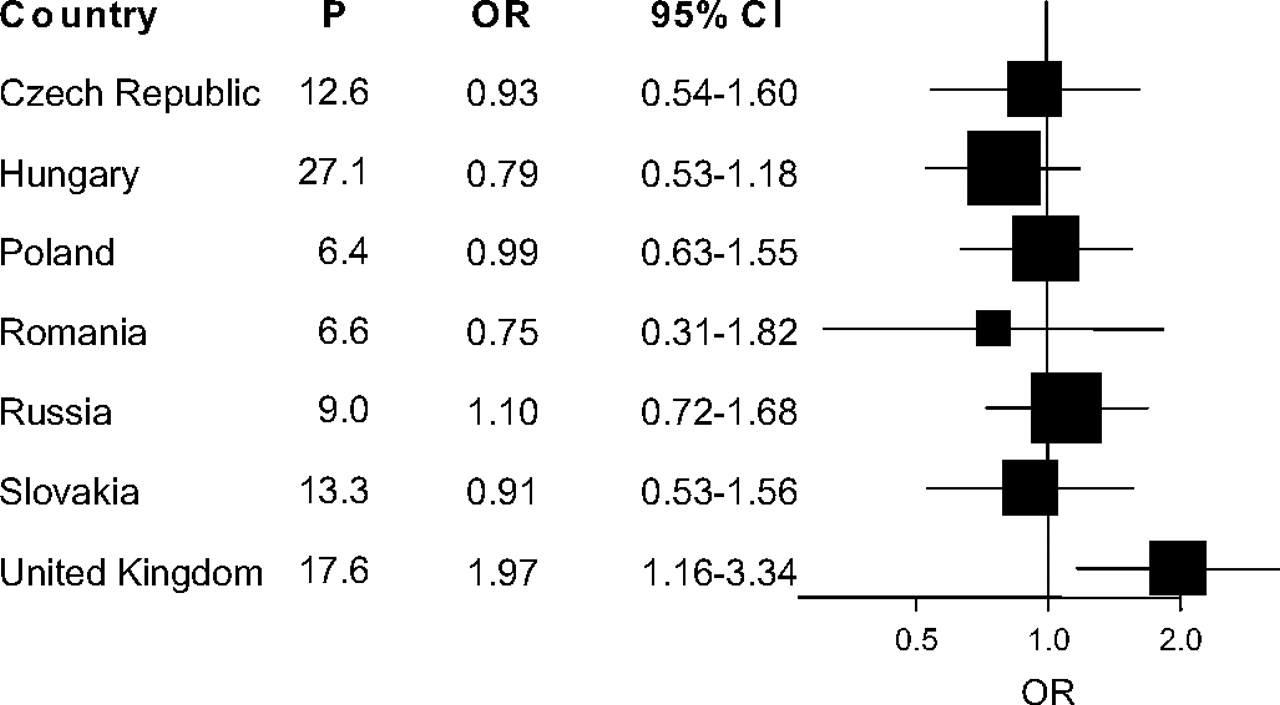
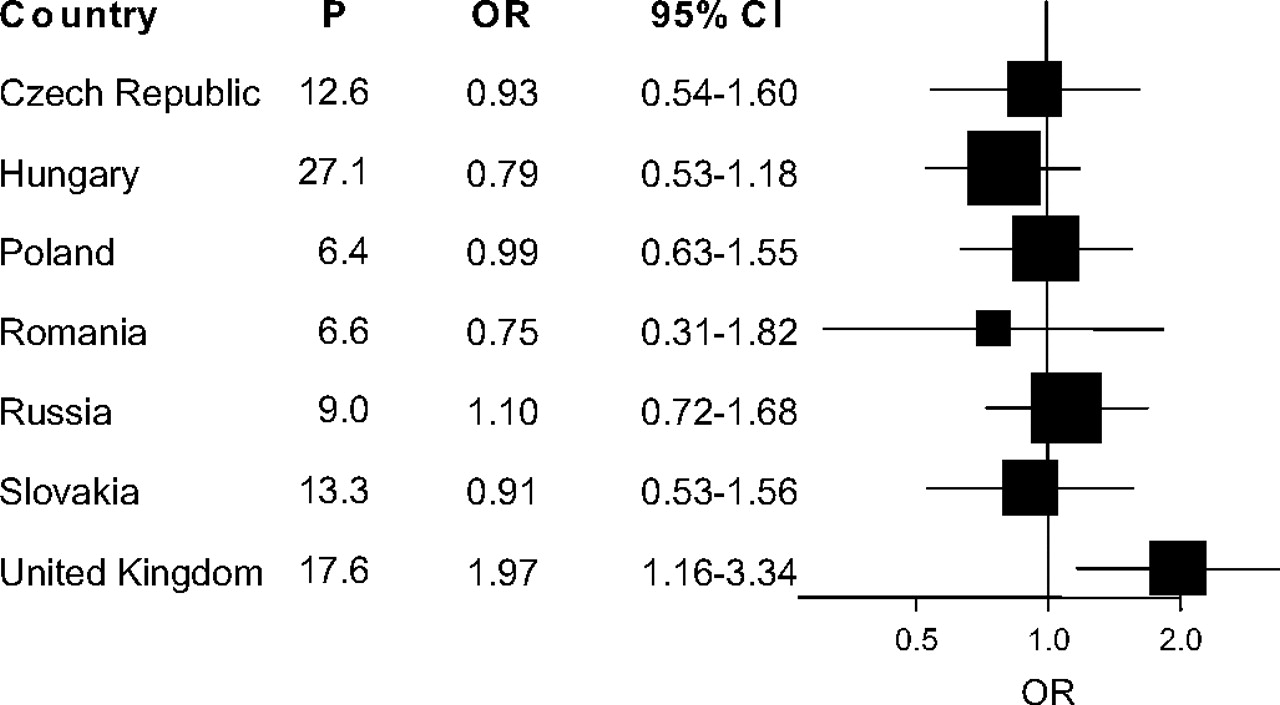
The country-specific prevalence of exposure to PAH among controls and ORs for ever PAH exposure are shown in figure 1. The lung cancer risk following exposure to PAH differed across countries (p=0.05); this heterogeneity was explained by a stronger effect in the UK compared to in the CEE countries (OR in CEE countries 0.93; 95% CI 0.77 to 1.14; difference between CEE countries and the UK: p=0.002). We found no evidence of heterogeneity within the CEE countries (p=0.73). The main analyses were therefore conducted separately for the CEE countries and the UK.
{kind=link}
Country-specific prevalence of occupational polycyclic aromatic hydrocarbon (PAH) exposure among controls and odds ratios for ever PAH exposure.
In CEE countries ever high-intensity exposure resulted in an OR of 1.11 (95% CI 0.60 to 2.05) (table 3). PAH exposure for 30 or more years was associated with an OR of 1.02 (95% CI 0.66 to 1.57) and the highest quartile of cumulative exposure was associated with an OR of 1.13 (95% CI 0.80 to 1.58). In the UK ever high-intensity exposure resulted in an OR of 2.68 (95% CI 0.74 to 9.77), and a linear trend was present for duration of exposure and cumulative exposure. The pattern of results did not change when studying those above the 90th percentile (>3.8 μg/m3-years) separately, and applying a 20-year lag did not modify the results either in the CEE countries or in the UK. Also, the risk estimates did not change markedly with regard to the time of exposure, that is, years since first exposure.
Occupational exposure to polycyclic aromatic hydrocarbons (PAH) and lung cancer risk
The apparently stronger effect of PAH in the UK warranted further analyses. We suspected residual confounding from exposure to asbestos because a large proportion of the UK subjects had been exposed to asbestos, 47% among men and 4% among women compared to 11% in men and 2% in women in the CEE countries, but the risk estimates did not change when a five-level variable was introduced to adjust for asbestos exposure in the regression model. The effect of PAH is present also in people unexposed to asbestos in the UK, which also points against confounding by asbestos. In contrast, asbestos exposure and smoking seemed to slightly modify the effect of PAH (table 4).
Odds ratios (ORs) for lung cancer following combined exposure to polycyclic aromatic hydrocarbons (PAH) and asbestos or tobacco smoking
The most frequent lung cancer types in the current study were squamous cell carcinoma (43%), adenocarcinoma (23%) and small cell carcinoma (14%). Table 5 shows how PAH exposure affects different types of lung cancer. PAH exposure does not seem to influence the risk of adenocarcinoma and small cell carcinoma, but for squamous cell carcinoma we see a non-significant association in the highest quartile of cumulative exposure, OR 1.33 (95% CI 0.91 to 1.96).
Odds ratios (ORs) of specific lung cancer types for cumulative polycyclic aromatic hydrocarbon (PAH) exposure in Central and Eastern Europe and the UK combined
Discussion
We found no evidence of an association between occupational PAH exposure and risk of lung cancer in the CEE countries after adjusting for relevant occupational exposures, but did find a significantly increased risk in the UK component of the study. In the UK there was also a clear excess risk (unlike in the CEE countries) following exposure to asbestos11 and the OR for joint PAH and asbestos exposure was close to multiplicative.
Retrospective exposure assessment is likely to be subject to some misclassification. The national experts were blinded to the disease status of the subjects when assigning exposures, suggesting that any misclassification of exposure from this source would be non-differential between cases and controls. Nevertheless, recall of job histories could differ between cases and controls, thus influencing the quality of the expert exposure assessment leading to a differential misclassification. A validation study on the occupational exposure assessment in our study showed that experts had low sensitivity and high specificity12 and simulations suggested that the likely effect of misclassification on risk estimates was an attenuation towards the null, in particular for exposures with low prevalence in the study population.13 High exposure prevalence, such as observed in the UK, may have resulted in less severe attenuation effect due to non-differential exposure misclassification.
Strengths of the current study include its size and the fact that data were collected from the subjects themselves in a face-to-face interview. Repeated training sessions and exercises for the national experts were conducted to assure high quality and comparability of the exposure assessment. Nevertheless, the prevalence of PAH exposure among controls was different between the countries, which could reflect a discrepancy in quality of exposure assessment in the different countries. Alternatively, the exposure circumstances in the UK versus CEE countries reflect true differences, which could be related to the economic development of the respective region or country, as CEE countries have experienced a economic lag compared to Western Europe.14
High levels of PAH are found in heavy industries, where workers commonly are exposed to other lung carcinogens as well, which makes it difficult to distinguish the effect of PAH from the effects of other occupational exposures. Consequently, we included occupational exposure to asbestos, silica, arsenic, chromium[VI] and cadmium as covariates in the statistical models, and we observed that the ORs for PAH exposure decreased by approximately 15% after adjustment for silica and metals.
Armstrong et al conducted a review and meta-analysis of 39 cohort studies, mostly representing highly exposed working environments, and reported a relative risk of 1.20 (95% CI 1.11 to 1.29) at 100 μg/m3 years benzo[a]pyrene exposure.15 A case–control study in Canada, for which the method of individual expert assessment was first developed,16 found an increased risk of lung cancer following PAH exposure among the highest exposed with an OR of 1.8 (95% CI 1.1 to 3.0), but only among non-smokers and light smokers.17 Pooled analysis of data from two German case–control studies based on a similar approach, showed an elevated OR of 1.53 (95% CI 1.14 to 2.04) for ever exposure to occupational PAH, and in addition a dose–response relationship.18 The exposure to PAH was estimated from defined jobs within 10 industries by applying measurements of benzo[a]pyrene at different workplaces,19 which resulted in a group of highly exposed subjects. Gustavsson et al conducted a population based case–control study in the Stockholm area and found a significantly increased risk of lung cancer in the highest PAH quartile with an OR of 1.60 (95% CI 1.09 to 2.34).20 A difference in the current study is that it also includes PAH exposure from mixtures containing low levels of PAH, such as diesel emissions and oil mists, while the Swedish and the German studies excluded these mixtures from their estimates. This group of studies is broadly in agreement with our results; the differences in risk estimated may be explained by choice of PAH definition, exposure assessment method and adjustment variables in the analyses.
The effect of PAH on squamous cell carcinoma seems stronger as compared to other histological types. As a result, the effect of PAH on lung cancer overall may be weaker in more recent studies as there has been a decline in the proportion of squamous cell carcinoma over time.21
We observed a suggestive joint effect of PAH and asbestos in the UK, with an OR of 4.4 for concurrent exposure, 2.1 for only PAH and 2.3 for only asbestos, which goes beyond an additive relation. A synergistic effect of occupational PAH and asbestos exposure has to our knowledge not been reported in epidemiological studies before but appears biologically plausible. Several epidemiological studies show evidence of a joint effect of smoking and asbestos exposure22–24 and a number of experimental studies have demonstrated a synergistic effect of PAH and asbestos.25–28 The mechanism may be linked to the strong ability of asbestos fibres to effectively bind PAH and deliver them to cells of the lung.29–31 However, our results concerning a synergistic effect are not statistically significant and therefore need to be replicated in other populations before a conclusion can be reached.
A limitation with our study is that hospital controls were used in all centres, except in Warsaw and Liverpool. The hospital controls were selected from a list of acceptable diseases by the interviewer from all eligible controls and no disease made up more than 20% of the control group. Hospital controls may not represent a random sample of the source population that generated the cases. A potential disadvantage is that the diseases of the controls may be associated with the PAH exposure, which then would provide a biased control group. Another concern is if different types of controls (hospital vs population controls) recall exposures differently, which could result in an information bias. In the current study Warsaw has the lowest prevalence of PAH exposure while Liverpool has the second highest prevalence, suggesting that type of controls was not systematically associated with either low or high exposure.
The response rate in the UK was lower (∼45%) compared to the CEE countries (∼85%) but similar to the average response rate achieved in surveys in the UK.32 Low response rate can lead to (i) selection bias, where respondents are systematically different from the non-respondents with respect to characteristics correlated with exposure or outcome, and (ii) loss of power to detect effects due to a resulting inadequate sample size. The proportion of exposed subjects in the UK component of the study could be underestimated because non-respondents are commonly more likely to be less well educated and have poorer lifestyles,33 which is also likely to be associated with highly exposed jobs.
Conclusion
The results from this case–control study indicate that occupational PAH exposure does not contribute substantially to the high incidence of lung cancer seen in CEE countries. In the UK, we observed an increased risk of lung cancer following exposure to PAH, as well as a possible joint effect of PAH and asbestos exposure.
What this paper adds
In a large study of occupational polycyclic aromatic hydrocarbon (PAH) exposure in Central and Eastern Europe, a region with a high risk of lung cancer, this group of agents does not appear to substantially contribute to the burden of the disease.
A stronger effect of PAH exposure was observed in the UK, which may be due to higher exposure levels and a joint effect with asbestos.
Community-based case–control studies with detailed assessment of exposure are useful to quantify the carcinogenic role of occupational agents.
Acknowledgments
We acknowledge the work of the coders and collaborators in each centre. We acknowledge also the contribution of Dr L Nadon and J Siemiatycki to the design of the study and G Ferro and N Travier regarding data management.
References
Footnotes
Funding This work was supported by a grant from the European Commission's INCO-COPERNICUS program (contract no. IC15-CT96-0313). In Warsaw, the study was supported by a grant from the Polish State Committee for Scientific Research, grant no. SPUB-M-COPERNICUS/P-05/DZ-30/99/2000. In Liverpool, the work was funded by the Roy Castle Foundation as part of the Liverpool Lung Project.
Competing interests None.
Ethics approval Ethics approvals were obtained from the relevant ethics review committees in each country, and subsequently by the IARC ethical review committee on 19 March 1999.
Provenance and peer review Not commissioned; externally peer reviewed.