Article Text

Abstract
The occupational epidemiological literature on extremely low frequency electric and magnetic fields (EMF) and health encompasses a large number of studies of varying design and quality that have addressed many health outcomes, including various cancers, cardiovascular disease, depression and suicide, and neurodegenerative diseases, such as Alzheimer disease and amyotrophic lateral sclerosis (ALS). At a 2006 workshop we reviewed studies of occupational EMF exposure with an emphasis on methodological weaknesses, and proposed analytical ways to address some of these. We also developed research priorities that we hope will address remaining uncertainties. Broadly speaking, extensive epidemiological research conducted during the past 20 years on occupational EMF exposure does not indicate strong or consistent associations with cancer or any other health outcomes. Inconsistent results for many of the outcomes may be attributable to numerous shortcomings in the studies, most notably in exposure assessment. There is, however, no obvious correlation between exposure assessment quality and observed associations. Nevertheless, for future research, the highest priorities emerge in both the areas of exposure assessment and investigation of ALS. To better assess exposure, we call for the development of a more complete job-exposure matrix that combines job title, work environment and task, and an index of exposure to electric fields, magnetic fields, spark discharge, contact current, and other chemical and physical agents. For ALS, we propose an international collaborative study capable of illuminating a reported association with electrical occupations by disentangling the potential roles of electric shocks, magnetic fields and bias. Such a study will potentially lead to evidence-based measures to protect public health.
Statistics from Altmetric.com
A substantial segment of the epidemiology on electric and magnetic fields (EMF) has focused on occupational settings, where exposures that are generally greater than those in the general population provide the potential for easier detection of effects. More importantly, EMF exposure is increasing in some occupational settings and concerns a large number of workers in a variety of industries. Further research affords an opportunity to prevent adverse health effects through exposure reduction, if warranted.
Most of the prior reviews focus on environmental exposures or on particular diseases, leaving many questions unanswered. To identify the highest priority research needs in occupational extremely low frequency (ELF) EMF epidemiology and to develop practical proposals to address remaining uncertainties, the Energy Networks Association (ENA) in the UK sponsored a meeting to which an international group of experts was invited. The sponsors imposed no constraints on the group’s review of the current state of knowledge or on their deliberations or recommendations. The meeting took place in Edinburgh, Scotland over 14–15 September 2006. In this summary report we review studies of occupational EMF exposure, discuss impediments in many of these studies, and present priority recommendations for research to address remaining uncertainties. Following extensive literature searches in PubMed and other databases, papers for detailed review were selected according to the judgment of workshop participants.
HISTORICAL OVERVIEW OF OCCUPATIONAL EMF EPIDEMIOLOGY
The occupational EMF literature encompasses a large number of studies with a variety of designs, such as proportional mortality studies, studies of workers in “electrical” occupations, studies of electric utility cohorts, and studies of the general population. The literature includes mortality and incidence studies.
Early studies were characterised by rather crude exposure assessment, sometimes limited to investigation of disease risk for individual job titles or to grouping of job titles as “electrical occupations”; often, an individual was classified as having an electrical occupation (variously defined) on the basis of a single job reported on a death certificate. Later studies improved exposure assessment through the use of job-exposure matrices (JEMs) based on workday measurements of magnetic field levels in various occupations. The most sophisticated and detailed JEMs relied on individual measurements for both individual work tasks and work environments. Initially, JEMs included occupations held predominantly by men and only recently have included those held mainly by women. Also recently, exposure assessment has shifted from jobs to relevant sources of exposure, permitting assessment of historical as well as current exposures.
Large cohorts of electric utility employees have contributed the most significant share of the occupational data.1–7 In addition, disease registries linked to JEMs have included workers in other industries.8–11 Following the first report by Wertheimer and Leeper in 1979 of an increased risk of adult cancer with work in electrical jobs,12 initial studies by Milham13 and others concentrated on leukaemia and brain cancer. Subsequent studies have investigated other cancers, notably breast cancer, and, more recently, cardiovascular and neurodegenerative diseases.
EPIDEMIOLOGICAL STUDIES OF OCCUPATIONAL EMF EXPOSURE AND HEALTH OUTCOMES
Cancer
A pooled analysis of major utility cohort studies published in 1999 found weak associations between occupational EMF exposure and leukaemia and brain cancer.14 Recent analyses of large electric utility cohorts in Denmark7 and the United Kingdom,5 6 welders in Sweden9 and railway workers in Switzerland15 showed no consistent risk increases for leukaemia or brain cancer with elevated occupational magnetic field exposure. Reduced exposure misclassification through improvements in exposure assessment methods, such as the use of detailed individual job histories augmented with full-shift measurements or JEMs, did not result in higher risk. Although a 2008 update to meta-analyses conducted in 199516 and 199717 found small risk increases for all types of leukaemia and brain cancer, pooled risk estimates were lower than in past meta-analyses, and leukaemia subtypes showed no consistent pattern when past and present meta-analyses were compared.18 Findings were not sensitive to assumptions, influential studies, weighting schemes, publication bias, study characteristics or funding source. Although a small risk increase for leukaemia and brain cancer cannot be entirely excluded, the lack of a clear exposure–outcome pattern suggests that magnetic fields as presently measured are by themselves not responsible for the observed excess risk. A recent World Health Organization review of occupational studies19 did not alter the International Agency for Research on Cancer’s 2002 conclusion that there is inadequate evidence to link magnetic field exposure to adult cancers.20
The hypothesis that magnetic field exposure increases breast cancer risk by suppressing nocturnal melatonin provided the motivation for studying breast cancer in relation to occupational magnetic field exposure. For male breast cancer, which is extremely rare, the literature consists mostly of studies with small numbers of cases. Both cohort and case–control studies show conflicting results, and overall do not provide strong support for an association.21–25
For female breast cancer, study results are mixed, with some studies reporting moderately elevated risks for premenopausal women and for oestrogen-receptor-positive breast cancers.25–28 Risk did not increase with elevated magnetic field exposure in a recent case–control study of more than 20 000 female breast cancer cases in Sweden that used an elaborate, female-specific JEM and included adequate control for potential confounders.10 Recent studies from Norway, the United States and China also indicated no association between occupational exposure to magnetic fields and female breast cancer.29–31 The epidemiological evidence available to date thus does not provide support for an association.
Several studies examined various other types of cancer.19 20 24 32–39 Overall, there is no consistent indication of any relationship between these cancers and occupational magnetic field exposure.
Neurodegenerative diseases
Research investigating risk of neurodegenerative diseases has focused mainly on Alzheimer disease (recently reviewed by Santibáñez et al40) and amyotrophic lateral sclerosis (ALS), and, to a lesser extent, on Parkinson disease.
A notable weakness in neurodegenerative disease studies is case identification. In some studies, cases were identified in hospitals and controls among patients with other diseases at the same hospitals or among friends or relatives of cases. These studies are likely to have greater potential for selection bias than population-based studies, which, on the other hand, have often identified cases from mortality registries and thus have greater potential for disease misclassification.41
No consistent evidence has linked Parkinson disease to high occupational EMF exposures. Most of the available studies found no evidence of increased risk.4 42–49
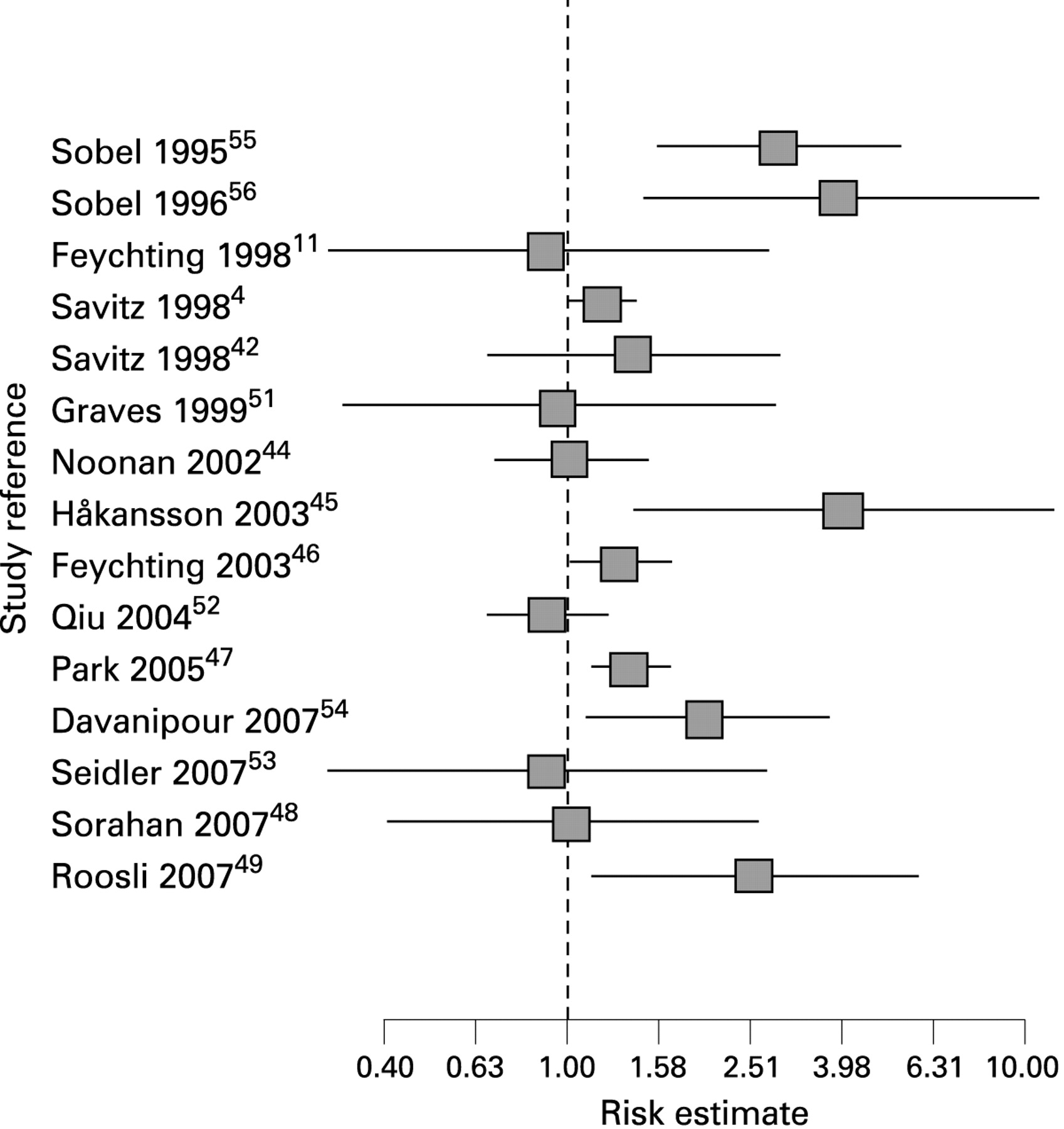
Early studies of Alzheimer disease provided weak evidence of an association with EMF.50 The strongest evidence came from two clinic-based studies, whereas evidence from four population-based studies was considerably weaker and more inconsistent, for example, in terms of exposure timing.4 11 42 51 Eight studies published in 2000 or later were population based, and again the results were mostly inconsistent,44–49 52 53 whereas one clinic-based study54 was consistent with previous studies by the same investigators that used their original design.55 56
Figure 1 provides risk estimates. Findings of increased risk do not seem to have been influenced by exposure assessment method or, with the exception of clinic-based studies, source of case identification. Subgroup analyses within studies strengthen the impression of inconsistency in the data. One recent study of mortality among electricity generation and transmission workers in the UK indicated no increase in Alzheimer disease,48 whereas a Swiss study of railway employees found an increasing risk of Alzheimer disease with increasing exposure.49

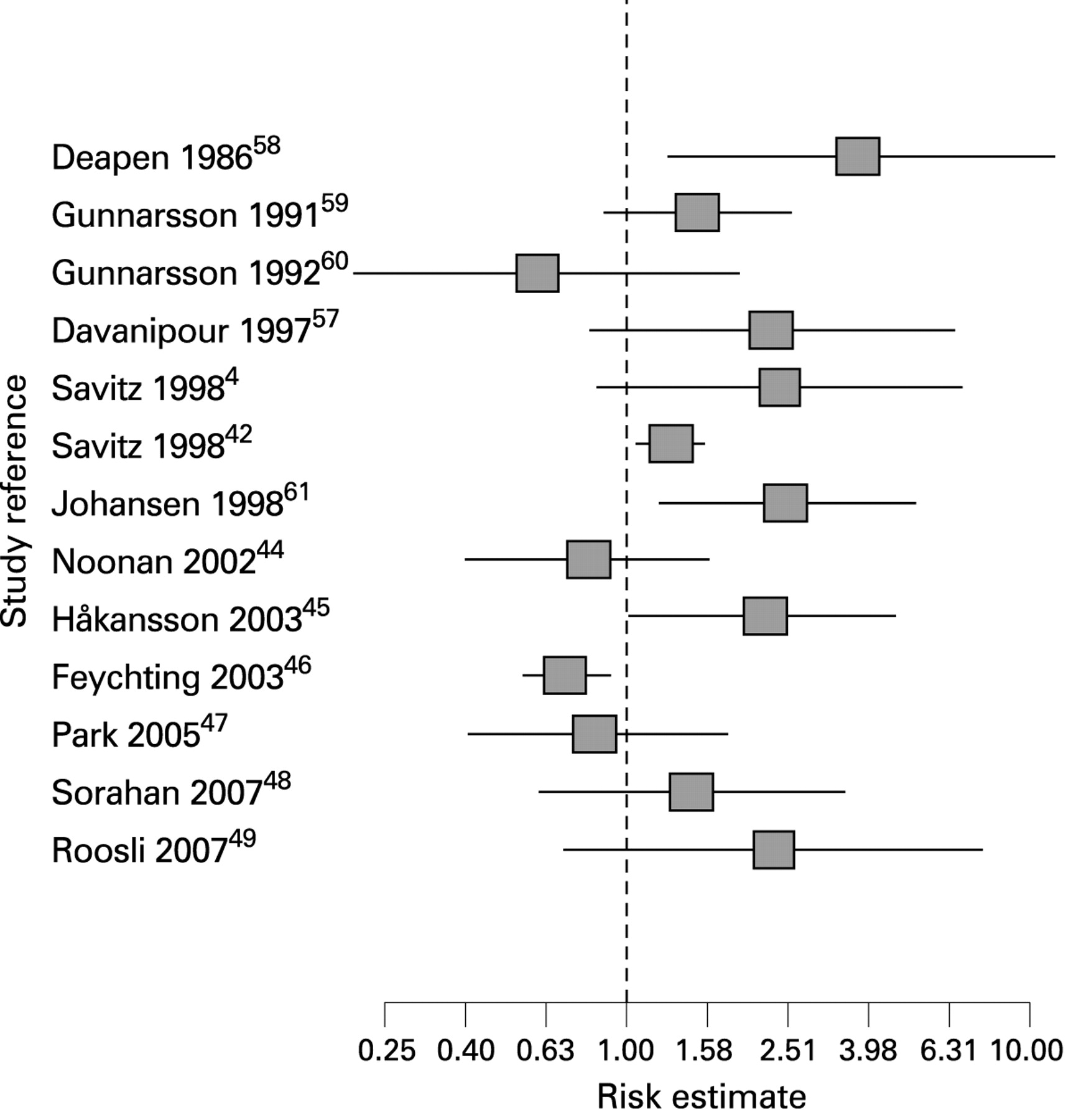
Table 1 summarises selected ALS studies; fig 2 shows risk estimates. Studies up to 2000 yielded more consistent evidence (table 1), with several clinic- and population-based studies suggesting an increased risk with employment in electrical occupations.44257–61 Two of six recent studies reported an increased risk with EMF exposure; one of the two may have been confounded by co-exposure to neurotoxic agents,45 and the other was restricted to railway workers.49 Three of the studies reporting no effect on ALS risk estimated magnetic field exposure through JEMs444647; like the earlier studies, however, two of these studies4446 found an increased risk for electrical occupations. A recent UK study reported broadly similar results for magnetic field exposure but found no risk increases in any job categories for motor neuron disease mortality among electricity generation and transmission workers compared to the general population.48 Thus, the evidence linking electrical occupations to an increased risk of ALS is remarkably consistent, but the evidence of an association with measured magnetic field levels is weaker. One explanation could be that another risk factor causes the increased risk in electrical occupations. Exposure to electric shock is a possibility,505861 although it is not likely to explain the entire risk increase.46

{kind=link}
{kind=link}
Other diseases
Cardiovascular disease
A 2007 review provides a detailed summary of studies of EMF and cardiovascular disease.62 Early descriptive studies reporting arrhythmias and tachycardia among Russian high-voltage switchyard workers first raised concern about cardiovascular effects from EMF exposure. Later studies were designed to investigate the hypothesis that long-term exposure to EMF may increase cardiovascular disease mortality by reducing heart-rate variability.63–67 In a 1999 cohort study of electric utility workers, Savitz et al found elevated risks of mortality from cardiovascular disease.68 A number of epidemiological studies in several countries that used a variety of study designs did not confirm Savitz’s findings.62 69–73 Additionally, recent experimental studies of volunteers74 found no decrease in heart-rate variability after exposure to EMF. We therefore conclude that occupational exposure to EMF does not appear to play a role in the aetiology of cardiovascular diseases.
Suicide
A pathway involving a possible effect of EMF on melatonin production, the role of melatonin in depression, and depression as an important risk factor for suicidal behaviour makes suicide a potential consequence of EMF exposure.75 76 Selected occupational studies on this subject are summarised in table 2.
In a study of electric utility workers, van Wijngaarden et al observed an exposure–response relationship with recent but not distant magnetic field exposure, with an OR of 1.7 in the highest exposure group.76 However, other electric utility worker studies provide only limited support.61 77 Studies using job title as a surrogate for EMF exposure are equally inconsistent.78–81 Lack of information on potential confounding factors in most studies further hampers the interpretation of these findings.
CHALLENGES
Occupational EMF exposure assessment
ELF magnetic field exposures
Exposure assessment, including the use of JEMs, remains a major challenge in occupational EMF epidemiology. For the past 15 years, the better studies have assessed the magnitude of time-weighted average (TWA) magnetic fields with JEMs based on personal measurements. JEMs for electric utility workers82 83 and for the general population84 85 have been constructed from extensive full-shift measurements with three-axis magnetic field meters that record an approximation to the “resultant” field every few seconds. These resultant data are combined with activity records to calculate either the TWA of the magnetic field or other metrics.
One problem with JEMs is that occupation is not the main determinant of magnetic field exposure. A person’s occupational exposure depends on magnetic field sources encountered during work, the average strength of sources, and the proportion of time spent at different locations relative to sources. Consequently, measured exposure varies widely among individuals within occupational groups.86 Furthermore, when JEMs are populated solely from measurements, they cannot properly represent historical exposures. Thus, JEMs can misclassify ELF magnetic field exposures.
Several improved JEMs have been developed. Miller et al constructed a JEM that classifies exposure measurements by location as well as by job.87 Renew et al assessed exposures of power station workers with a magnetic field model that takes account of the engineering design, layout and operational history for each power station.88 Results from this model were combined with the proportion of time spent in specific station areas for each job and with occupational history to give individual exposure values. This approach has the added advantage of reconstructing historical exposures. In another approach, Coble et al (submitted) modified the JEM’s average magnetic field for an individual by using interview information on exposure times and locations relative to reported sources. A combination of these innovations might reduce exposure misclassification in future studies. However, considerable attention to detail is required when applying improved exposure metrics to ensure that they result in exposure assessments which are more accurate.
Electric fields, shocks and contact current
Magnetic fields are not the only aspect of the ELF electromagnetic environment, which also includes electric fields, electric shocks, microshocks (spark discharge) and contact current.
In electric utility environments, typical elevated electric fields induce greater current in the body than typical elevated magnetic fields, and far greater currents occur in the body during electric shocks, albeit very briefly. Miller reported an association for leukaemia in utility workers that was much stronger for electric fields than for magnetic fields,87 and electric shocks have been suggested as a risk factor for ALS.
Elevated electric field exposures occur only where there are unshielded high-voltage conductors. Moderate-to-high levels (0.1 to >1 kV/m) are found only near high-voltage transmission lines or exposed busbars in substations. In these limited environments, adequate estimates of TWA electric field exposures can be obtained from spot measurements or computer modelling.89
A “taxonomy of electric shocks” that identifies the different types of shocks is needed for future investigations. Severe electric shocks among utility workers are rare and are reportable to government authorities in some countries; this may be useful for compiling data about the rate of severe but non-fatal shocks. Microshocks can be experienced by a person on touching a conducting object in an electric field greater than about 2 kV/m. Contact current flows imperceptibly into the person’s body while the person remains in contact with the conductor.
Alternative magnetic field exposure metrics
The absence of an established mechanism by which magnetic fields could produce health effects90 makes it difficult to identify the definitive metric for assessing exposure. Misspecification of the exposure metric is likely to bias risk estimates towards the null.
A possible source of misclassification in EMF exposure assessment is the sole use of the resultant magnetic field as the exposure metric, on the assumption that TWA adequately represents magnetic field exposure. Other magnetic field metrics that may be more biologically relevant include percentage of time above a threshold, induced current in the body, combinations of ac and dc fields, the ratio of the major and minor axes, and intermittency of exposures.91 Although many alternative metrics such as these are highly correlated with the TWA, some are not. We can now measure alternatives to the resultant using instruments that capture the magnetic field vector waveform in great detail,92 combined with software that calculates the alternative metrics from the waveforms (Bowman et al, in preparation). The use of multiple metrics for measuring EMF exposure is likely to lead to associations that are purely due to chance. To minimise this possibility, the number of metrics should be limited to either those used in previous studies or those arising from a particular biophysical interaction requiring epidemiological investigation.
Multivariable statistical techniques93–97 may also be useful in analysing multiple exposure metrics obtained by using measurement data from vector waveform monitors.97–99
Health outcome assessment
Misclassification of health outcomes can be an important source of error in occupational epidemiology research. Occupational cohort studies frequently rely on mortality data for outcome determination. For diseases with high case fatality rates (for example, ALS and some cancers), mortality provides a reasonably complete and accurate indication of disease incidence. However, diagnostic information inferred from death certificates may be inaccurate for other outcomes, such as Alzheimer disease, cardiovascular disease and suicide.41 100 In addition, cases may go undetected or, if identified, may be inaccurately reported. Where feasible, obtaining clinical and pathological information would highly benefit disease diagnosis.
Analyses
Control, evaluation and modelling of potential biases
Recent advances in statistical modelling provide powerful tools that may prove useful for resolving some of the thornier EMF-related analytical issues; for example, for disentangling individual and joint effects of jobs, shocks and magnetic fields in future ALS studies or for taking the exact timing of EMF and other exposures into account. For example, hierarchical regression methods provide a generalised framework for regression analysis that encompasses a number of different approaches, including non-parametric regression, empirical Bayes regression, random-coefficient regression, multilevel analysis, generalised estimating equations, G-estimation, penalised-likelihood analysis, ridge regression and Stein estimation.101
Traditional sensitivity analysis, which estimates what the true effect measure (for example, relative risk) would be in light of the observed data and a hypothetical level of bias, can also be improved through the use of Bayesian or Monte Carlo methods.102–104
Combining results across different studies
The proliferation of new EMF studies in recent years provides excellent opportunities for combining data across studies. Although attempts have been made to combine results using meta-analysis of summary results from published epidemiological studies of EMF-exposed workers,18 the only effort to perform analyses of actual data sets pooled from multiple studies was attempted for the utility worker cohorts.14 Pooled analyses can avoid many difficulties associated with meta-analytic techniques but require that participating investigators develop standardised protocols for reconciling study differences, for example, exposure assessment protocols and information on confounding factors and co-exposures.101
RESEARCH RECOMMENDATIONS
Much has been learned from occupational EMF epidemiology; however, several issues remain to be resolved. Research should employ improved case ascertainment and diagnosis, better exposure assessment, and better assessment of potential confounding factors. Future studies should also be large enough to investigate modifying factors such as age at disease onset, sex and the effect of exposure timing.
The highest occupational EMF research priorities emerge in the areas of exposure assessment and investigation of specific health outcomes.
Health outcomes
The most promising research would focus on clarifying the reported association of electrical occupations with ALS. As ALS is almost invariably fatal within a few years of diagnosis, ALS deaths in the cohort mortality studies are likely to closely reflect incidence. However, extremely low incidence presents a major difficulty in studying ALS, even over a protracted period within a single cohort. Thus, the number of cases for analysis in individual studies has been small. A pooled analysis of previous cohorts, combined with a JEM refined to the extent possible for past job descriptions, could give a better indication of whether a true causal factor or the presence of biases produced the observations published to date.
Exposure assessment
Methods for exposure assessment remain among the most influential determinants of study quality; thus, broader and more precise exposure assessment can be an important advancement. First, the improved method developed to quantify magnetic field exposure for workers in power stations should be pursued in future studies of existing electric utility cohorts. New studies should include detailed information from interviews or company records for groups of jobs with regard to field sources encountered during work, the average strength of these sources (depending on the facility), and the proportion of time spent at different locations relative to sources. To estimate exposures for each subject, algorithms that combine this information with existing EMF exposure data need to be developed and validated against workplace measurements. Second, methods for assessing exposure to electric fields, spark discharge and contact current are worthy of further research, as is an investigation of alternative exposure metrics for magnetic fields. With new data, we can develop a more complete JEM that combines job title, work environment and task, and an index of exposure to electric fields, magnetic fields, spark discharge, contact current, and other chemical and physical agents.
CONCLUSIONS
Although the epidemiological evidence suggests excess risk with occupational EMF exposure for some health outcomes, there is no outcome for which the combined evidence is strong or consistent enough to support the conclusion that a health hazard exists. For some health outcomes, results from different studies are inconsistent; for others, the evidence is fragile because of small numbers and poor precision, or because of the inherent difficulties of studying particular conditions and exposures. In vitro, in vivo or mechanistic evidence has not provided clues for further investigation in occupational epidemiology. ALS is deemed the highest priority health outcome to pursue in future studies, along with improvements in exposure assessment. The development and application of methods to determine the presence and magnitude of biases using sensitivity analyses also deserves further consideration.
Acknowledgments
We thank the Energy Networks Association (ENA) and all participants at the ENA-sponsored workshop Future Needs of Occupational ELF Epidemiology for their contributions. Special thanks to Gail Lundell for expert scientific editing.
REFERENCES
Footnotes
-
Competing interests: This paper is based in part on deliberations at a workshop sponsored by ENA, a UK trade association. L Kheifets and JM Harrington organised and chaired the workshop, with other co-authors as participants. R Kavet and G Mezei are employed by the Electric Power Research Institute; DC Renew is employed by National Grid plc and worked on this paper with the company’s permission.
-
Disclaimers: The findings and conclusions in this paper have not been formally disseminated by the U.S. National Institute for Occupational Safety and Health and should not be construed to represent any agency determination or policy. The views expressed in this paper are those of the authors and not necessarily those of National Grid.