Article Text

Abstract
Background: Pain in the neck and upper extremity is reported with high frequency in repetitive work. Mechanical overload of soft tissues seems a plausible mechanism, but psychological factors have received considerable attention during the past decade. If psychological factors are important for development of regional pain in repetitive work, stress symptoms would likely be on the causal path.
Aims: To examine whether objective measures of repetitive monotonous work are related to occurrence and development of stress symptoms.
Methods: In 1994–95, 2033 unskilled workers with continuous repetitive work and 813 workers with varied work were enrolled. Measures of repetitiveness and force requirements were quantified using video observations to obtain individual exposure estimates. Stress symptoms were recorded at baseline and after approximately one, two, and three years by the Setterlind Stress Profile Inventory.
Results: Repetitive work, task cycle time, and quantified measures of repetitive upper extremity movements including force requirements were not related to occurrence of stress symptoms at baseline or development of stress symptoms during three years of follow up.
Conclusions: The findings do not indicate that repetitive work is associated with stress symptoms, but small effects cannot be ruled out. Thus the results question the importance of mental stress mechanisms in the causation of regional pain related to repetitive work. However, the findings should be interpreted with caution because the stress inventory has not been validated against a gold standard.
- job control
- job demands
- monotonous work
- musculoskeletal disorders
- psychosocial strain
- stress reactions
Statistics from Altmetric.com
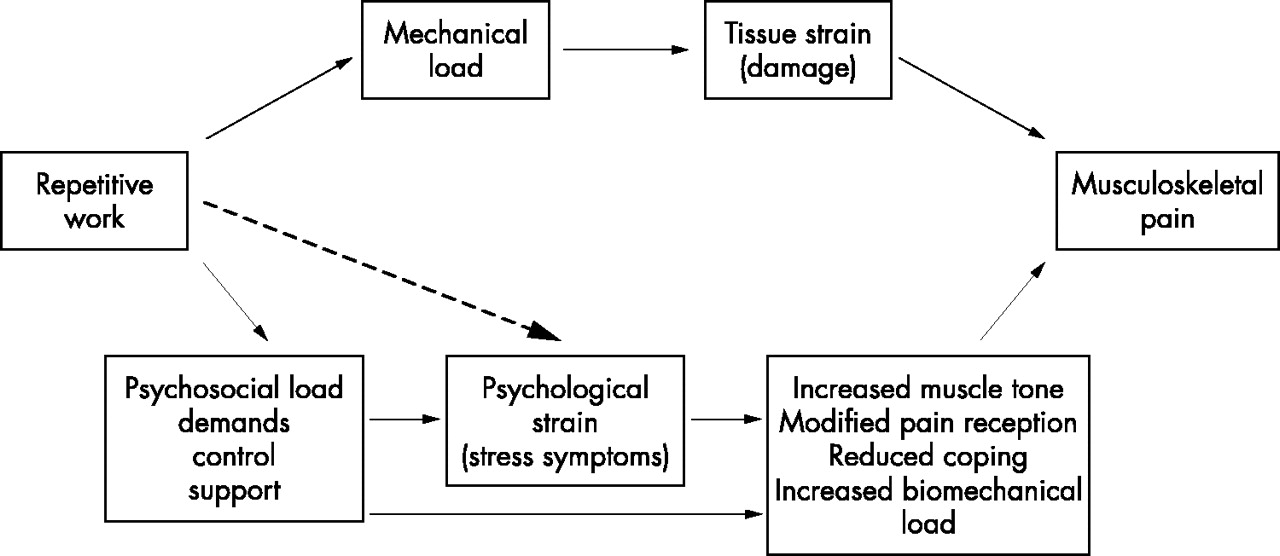
Discomfort and pain in the neck, shoulders, and upper extremities are reported with increased frequency in repetitive work.1 It seems straightforward to attribute pain reporting to mechanical tissue overload related to repetitive movements, force requirements, and awkward postures. Although repetitive work is defined by physical work characteristics (upper extremity movements), it is inherently correlated with psychosocial factors. For instance, one measure of repetitiveness is the task cycle time, which may be related to time pressure and perceived job demands. Moreover, repetitive work is most often associated with low job control, skill discretion, and decision latitude. Therefore it is plausible that the psychosocial load related to repetitive work could lead to stress symptoms and musculoskeletal pain.2–9 From a preventive point of view it may be important to clarify whether musculoskeletal pain related to repetitive work is accounted for by the physical characteristics of the work or by psychosocial correlates to the physical exposures. We have recently corroborated earlier findings of relations between perceived psychosocial job characteristics and pain in the neck-shoulder region by a longitudinal study of Danish industrial and service workers.10,11 Several mechanisms have been suggested to explain how psychosocial factors may cause musculoskeletal pain2–4,12,13 (see fig 1). Repetitive work may increase psychosocial load and cause psychological strain (stress symptoms), which in its turn may lead to musculoskeletal tenderness and pain by increased muscle tone, modified pain perception, reduced capacity to cope, or increased biomechanical load. It is also conceivable that increased psychosocial load in repetitive work can cause musculoskeletal pain through these mechanisms without subjective perception of stress symptoms (fig 1). Nevertheless, numerous studies have shown strong relations between job related stress symptoms and reporting of musculoskeletal pain, and several authors pay attention to the stress hypothesis—that is, psychological load and stress symptoms are on the causal path from repetitive work to musculoskeletal pain7,8–14 (fig 1). Since almost all earlier studies are cross-sectional using self-reports on psychological load, stress symptoms, and pain,14 the results could reflect that individuals with musculoskeletal pain perceive the working environment as stressful and report more stress symptoms. Cross-sectional associations may simply reflect individual psychological characteristics rather than causal relations between independent phenomena.15 In order to help distinguish between the crucially different options for understanding the causation of musculoskeletal pain in repetitive work (fig 1), we examined prevalent and newly developed stress symptoms in a longitudinal study of workers with and without repetitive work. Thus this paper puts the association indicated by the dotted arrow in fig 1 to a critical test.
{kind=link}
Biomechanical and psychosocial models to explain the high occurrence of musculoskeletal pain in repetitive work. The association put to a critical test in this paper is indicated by the dotted arrow in bold. Repetitive work is the objective work setting characterised by repeating a single work task over and over while performing repetitive movements of the upper extremities. Load (whether of mechanical or psychological nature) is the term used for exposure related to repetitive work. Strain (whether of biological or psychological nature) is the term used for the outcome (the response to an exposure somewhere on a causal pathway): unspecified tissue damage (biological) or stress symptoms (psychological), respectively.
METHODS
During 1994 and 1995 a total of 4198 workers at 19 workplaces throughout Denmark were invited to participate in the study. The workplaces were selected to represent the main types of repetitive manual work among men as well as women in Denmark in the mid-1990s. Our sample included four food processing companies, three textile plants, four electronic plants, three cardboard industries, and five companies performing service work (two postal sorting centres, one bank, and two supermarkets). The workers were approached through the companies by one of three regional occupational health clinics. With the exception of apprentices all currently employed male and female workers were eligible. Participants gave written consent and the appropriate ethics committees approved the study protocols. Selection of participants and methods are described in detail elsewhere.16,17 Altogether 3123 workers filled in a questionnaire on demographic and medical characteristics, stress symptoms, lifestyle, and spare time activity (74.4% of 4198 eligible workers; table 1). Identical questions on stress symptoms were to be completed by all participants approximately one, two, and three years after the baseline questionnaire was administered. The actual time span between the follow up rounds ranged from 4 to 24 months (25th–75th centile in workers with repetitive work: 8.7–12.2 months; and in workers with non-repetitive work: 8.2–12.5 months; table 2).
Characteristics of the study population at baseline by type of work
Symptoms from the Setterlind Stress Profile Inventory18
Main messages
-
A nationwide prospective study did not indicate that workers performing repetitive work develop stress symptoms more often than workers having varied work.
-
Results do not support the widely held hypothesis that regional pain in repetitive work is mediated by job related mental stress reactions, but the findings do not exclude this possibility.
Measures of repetitive work characteristics
The physical exposure characteristics were assessed in four steps at baseline by a task based exposure assessment strategy.17 Firstly, ergonomists visited the 19 workplaces, and work tasks were classified as either repetitive or control tasks. A task was defined as repetitive if it involved continuous repetitive hand or arm movements. A control task was characterised by varied activities. Examples of repetitive task groups were deboning ham, sewing machine work, deboning poultry, packing, continuous data entering, shop cashier, and manual machine feeding. Non-repetitive or control tasks included varied office work, supervision of machines, different kinds of maintenance work, or internal transportation. Thus the classification of work task as repetitive or non-repetitive was based on judgements undertaken during work site visits by several ergonomists and not on measurements. The classification was approved by all members of the project team in the initial phase of the study. While the repetitive tasks were validated by measurements of hand and arm movements, no measurements of control tasks were undertaken.
Secondly, we aggregated repetitive tasks with comparable levels of physical exposure in two task groups. Thirdly, between one and seven workers in each of the 103 task groups were videotaped from three camera angles for at least 10 working cycles or for a minimum period of 10–15 minutes. Based on repeated reviews of the video recordings, the following exposure variables were quantified: (a) the duration of the task in seconds (cycle time); (b) the percentage of the cycle time with exertions of the upper extremities; (c) the number of dominant wrist movements/minute; and (d) wrist force requirements. The force requirements were subjectively assessed and computed by the observer using five point ordinal scales (zero to four), relative to maximum voluntary contraction (MVC). The four measures of physical repetitive work characteristics were selected to obtain quantifiable and general indicators of the physical characteristics of repetitive work. The final step involved allocation of time weighted exposure measures to each participant on the basis of self-reported task distribution during a normal week of 37 hours.
Workers were classified as doing repetitive work if at least one of their tasks belonged to a repetitive task group (2033), otherwise they were classified as doing non-repetitive work (813). Altogether 277 workers were excluded from further analyses because they performed activities that could not be allocated to a task group. Among workers in repetitive tasks, 55% had only one task. The remaining 45% of the workers who had more than one task, spent on average 31% (range 2–50%) of their total working time in repetitive work.
Policy implications
-
Attention to the psychosocial work environment should not distract from preventive measures addressing the physical risk factors in repetitive work
Stress symptoms
Somatic, emotional, and cognitive symptoms were recorded at baseline and at each of the three follow ups by 18 questions from the stress profile questionnaire developed by Setterlind and Larsson.18 This stress profile includes three dimensions of stress symptoms—namely somatic (six items), emotional (eight items), and cognitive symptoms (four items) (table 2). At each occasion participants were asked to answer the questions with a consideration of the past four weeks. Each item was rated on a five point scale ranging from “very often” (1) to “never” (5).
Scores for each dimension were scaled to range from 0 (low stress) to 4 (high stress). Finally, the three stress dimension scores were summed to obtain an overall score of stress symptoms ranging from 0 to 12. A state of stress at baseline was defined by an overall stress score of 4 or more which corresponds to reporting of at least one third of the somatic, emotional, and cognitive stress symptoms very often or often during past four weeks. Development of new stress symptoms during the follow up period was defined by an overall stress score less than 4 at baseline combined with an increase in overall stress symptom score of 4 (33% of the scale) from baseline to the first, second, or third follow up round. Thus a gradual increase in stress symptoms through several follow up rounds as well as a rapid increase from one round to the next contributed to the definition of new stress symptoms. The arbitrary cut-off values were chosen as trade-offs between magnitude of stress score (baseline) or change of stress score (follow up) and the number of participants fulfilling the stress criteria. We aimed at a substantial stress score or change in stress score to increase specificity and a sufficient number of participants to obtain reasonable power. The cut-off values were fixed before any analyses of exposure-outcome relations were performed.
Measures of other characteristics
Leisure time activity was categorised into none or light physical activity for less than 4 hours/week, and physically active (light physical activity for more than 4 hours/week or hard physical activity for more than 2 hours/week). Body mass index was calculated from measured weight and height. Pressure pain threshold was measured by means of an algometer (Somedic, Stockholm, Sweden). Pressure was applied with an increased rate of 50 kPa s−1 through a circular rubber coated pressure head (area 1 cm2). The mean values of measures on the tibia and vastus medialis muscle were thought to give an expression of the person’s overall pain threshold. These values were dichotomised for the purpose of analysis using the 25th centile as the cut-off point (<411 kPa for women and <665 kPa for men).
Personality traits were measured by the dimension “intrinsic effort” from Siegrist’s effort-reward model.19 The 29 items from the four subscales, “need for approval”, “competitiveness”, “disproportionate irritability”, and “inability to withdraw from work” were summed up to an index and dichotomised into high versus low intrinsic effort on the basis of the 25th centile of the mean values.
Design of analysis
The baseline association between observed measures of repetitive work and the prevalence of stress symptoms was analysed by logistic regression.20 Subsequently, in a longitudinal approach, we analysed baseline determinants for development of stress symptoms during follow up in the subset of participants without stress symptoms at baseline (total stress symptom score below 4). The number of follow up rounds taken to develop stress symptoms was analysed by logistic regression using a follow up round as the observational unit. Thus, the actual duration of the time interval from one round to the next was not accounted for. Only small differences in the average duration of time intervals between rounds in workers with and without repetitive work were observed (difference in average durations from round 1 to 2: 5.2%; from round 2 to 3: 1.6%; and from round 3 to 4: 8.2%). Observations were right censored when the criterion on newly developed stress symptoms became fulfilled. This application of logistic regression is equivalent to discrete survival analysis.21 The odds ratios describe the relation between the follow up outcome (new stress symptoms: yes/no) and determinants at baseline. In order to account for changes in work tasks during the follow up period, which might dilute an effect related to baseline exposures, we performed an analysis only including the first round of follow up. Furthermore, two dummy variables were designed to indicate increase and decrease, respectively, in the time weighted duration of work tasks (task cycle time). The dummy variables were included in the regression models to examine whether time varying exposure during follow up changed the association between baseline physical job characteristics and stress symptoms.
To account for possible confounding conferred by the skewed distribution of several characteristics across workers with and without repetitive work (table 1), we adjusted all models by the following medical, psychological, and social characteristics which were considered for inclusion a priori: centre (Glostup/Aarhus/Herning), gender (woman, yes/no), age (continuous), physically active in leisure time (yes/no), body mass index (above 75th centile, yes/no), low algometric pressure threshold (yes/no), high intrinsic effort personality (yes/no19), living as married (yes/no), and self-reported psychiatric disorder (yes/no). It is considered state-of-the art to stratify on centre in multicentre studies. Moreover, adjustment for centre accounts for possible geographical differences in exposure and perception of stress, which might bias the risk estimates. Intrinsic effort personality and psychiatric disorders are plausible determinants of stress perception and were included in the models because of consistent and strong bivariate associations with stress symptoms in the present dataset. A number of hypothetical determinants such as gender, age, pain threshold, high body mass index, and marital status were also included because of skewed distribution among workers with and without repetitive work. Educational level was not included since the study population comprised only unskilled workers. The determinants remained in the models whatever the magnitude or significance of effect. Spearman correlations of the ranks of the 18 Setterlind Stress Inventory variables were computed (SAS corr procedure (Spearman option)). The t test and χ2 test were computed using standard methods. The models were examined with the Hosmer-Lemeshow goodness of fit test (SAS logistic procedure20).
Since the design of the analysis was based on a discrete disease outcome that may be less sensitive than analyses based on continuous stress scores, we performed additional analyses of the within subject change of the stress score from baseline to the first follow up examination. The difference in stress score exhibited a symmetrical distribution. The impact of discrete and continuous measures of repetitive work at baseline was analysed by a general linear model (SAS PROC GLM).
RESULTS
The baseline prevalence of stress symptoms according to our definition was 4.9% (95% CI 4.1 to 5.7) and the average incidence of new cases with stress symptoms during follow up was 21/1000 person-years (95% CI 17 to 26; table 3). The incidence of new cases declined gradually from 25.1/1000 person-years during the first follow up round to 15.2/1000 person-years in the third follow up round.
Incidence of stress symptoms during follow up of workers without stress symptoms at baseline*
All 18 items constituting the Setterlind Stress Inventory were significantly correlated, the Spearman correlation coefficients ranging between 0.18 and 0.67. So were the emotional, cognitive, and psychosomatic dimensions of stress (correlation coefficients ranging from 0.23 to 0.38), and on average the three dimensions contributed almost equally to the summary stress score (somatic symptom scores 31%, emotional scores 37%, and cognitive scores 31%). In some 50% of workers the stress symptoms disappeared from one round to the next (data not shown).
The average summary stress score varied between 0.65 (a postal sorting centre) and 1.21 (a textile plant) across the 19 companies, but an analysis of variance did not indicate significant impact of company (workplace) on the mean stress score.
Repetitive work defined as continuous repetitive movements of the upper extremities was not associated with stress symptoms in the baseline comparisons (table 4), nor were the three quantifiable measures of repetitive work, namely the time weighted task cycle time, the duration of exertion, and the number of wrist movements per minute (table 4). Furthermore, stress symptoms did not develop more frequently in workers with repetitive work tasks, although small increments cannot be ruled out. Among workers with repetitive work, the data revealed no indication of an increase of stress symptoms with shorter task cycle times, higher level of exertion, or higher number of wrist movements per minute (table 4). Similar results were obtained when the follow up analysis was restricted to the first round of follow up to counteract possible effects of changing exposures during the follow up period. Inclusion of dummy variables to indicate increase or decrease in the time weighted number of wrist movements during the follow up period did not change the measures of association between physical factors and stress symptoms (data not shown).
Adjusted odds risk ratios* for stress symptoms according to work characteristics at baseline
Extraneous factors that consistently had significant associations with stress symptoms in cross-sectional as well as longitudinal analyses included algometric pressure pain threshold (a low threshold associated with a high occurrence of stress), marital status (not living as married associated with stress), high intrinsic effort personality, and self-reported psychiatric disorder. Since the adjusted risk odds ratios were close to crude risk ratios, only the former has been included in table 4.
The average summary stress score was at the same level at baseline in workers with and without repetitive work. In the former the average stress value was 0.82 on a scale from 0 to 12, and in the latter 0.80. The average change in stress score from baseline to the first follow up examination was 16% of the baseline value in workers without repetitive work and 20% in workers with repetitive work (p>>0.05). No indication of increase of stress score with increasing repetitiveness was revealed (data not shown).
DISCUSSION
The findings of this study did not indicate that physically monotonous and repetitive work is associated with occurrence or subsequent development of stress symptoms. Thus, our findings question the hypothesis that job induced stress symptoms are intermediary between repetitive work and musculoskeletal pain disorders—a hypothesis that has achieved considerable attention during the past 10 years.2,4–7,9,13,22–24 In a 1993 review of psychosocial factors and musculoskeletal disease, Bongers et al concluded that monotonous work, high perceived work load, and time pressure are related to musculoskeletal symptoms and that some studies indicate that stress symptoms contribute to the development of the disease2—although firm conclusions on the role of these factors in the aetiology of upper extremity pain are not possible due to the cross-sectional nature of most studies.14 Lundberg reported an association between perceived stress and increased trapezius electromyographic (EMG) activity in women performing repetitive work and proposed that mental stress contributes to development of upper extremity disorders.13 Similarly, Rissen et al found a relation between perceived stress symptoms (feeling stressed, exhausted, tense) and EMG activity during work that could be of importance for musculoskeletal disorders.25 Most studies addressing the impact of work related psychosocial factors on pain reporting are at risk from circularity between causes and suggested effects unless independent measures of exposure and outcomes are applied in longitudinal designs.2,26 Our study did not indicate that objective measures of repetitive work were related to occurrence or development of stress symptoms. However, several alternative interpretations and various limitations of the study need to be considered.
Musculoskeletal complaints were not included in the presented analyses. Could the absence of associations between the independent and quantified measures of repetitive work and self-reported stress complaints simply reflect that work related pain in the neck and upper extremities is not prevalent in our study population? Probably not: three earlier papers based on data from the cohort have shown increased risk of shoulder disorders as well as neck/shoulder pain in relation to repetitive work and to quantified measures of repetitiveness.10,11,16 Although the study was not designed to obtain a random or otherwise specified sample of repetitive work in Denmark in the mid-1990s, the study does encompass the main types of monotonous repetitive work in industrial and non-industrial occupations. Thus the external validity of the study must be considered high and the lacking relation between objective measures of repetitive work and development of stress symptoms cannot be rejected with reference to an unexpected low occurrence of musculoskeletal complaints.
Could limitations in study design have bearings as to the lack of relation between objective measures of repetitive work and stress complaints? The duration of follow up spanned up to three years. Newly onset stress symptoms induced by long term repetitive work would not be identified. But the lack of associations in the cross-sectional analysis at baseline does not indicate long term effects since the average seniority of repetitive work in our population was 9.1 years (SD 7.1 years). The study was designed according to the full panel design implying that measurements of exposures as well as outcomes were repeated at each follow up occasion to allow for changes in exposure during follow up.27 To account for gradual as well as abruptly developed stress symptoms, the main analysis focused on stress symptoms developed during the entire follow up period in relation to baseline estimates of repetitive work. In additional analyses taking account of time varying exposure during follow up, we were still unable to identify associations between any of the objective measures of repetitive work and stress symptoms.
We focused on a discrete disease outcome in order to give priority to effects that may be of clinical relevance. This corresponds to the upper tail of the stress score distribution while variation in the lower end is of less interest. Analyses based on the continuous outcome measure would give weight to mean values, and strong assumptions with respect to the linearity of the stress scale would be needed. Nevertheless, sensitivity analyses of the within-person change in the summary stress score between baseline and the first follow up round did not indicate that we missed any effect of repetitive work on development of stress symptoms by giving priority to the less sensitive discrete disease outcome strategy.
If work related stress symptoms are mainly developed during the first months or years of a new employment, they could be hard to detect in a “steady state” population with an average duration in the present job of nine years. However, our data are not consistent with this hypothesis. The prevalence of stress symptoms at baseline and the incidence of new stress symptoms during follow up increased with increasing duration of the employment at baseline. The adjusted odds ratio for stress symptoms among workers employed for more than five years compared to workers employed for less than two years was 2.8 (95% CI 1.6 to 4.9). Moreover, the relation between repetitive work and stress symptoms was not modified by duration of employment in either analyses of baseline occurrence or occurrence of new cases during follow up.
The statistical power of the study is reflected by the confidence intervals. The majority of the upper limits were at or below 1.5 (table 2) indicating an acceptable power, although small effects cannot be ruled out. Some upper limits in the longitudinal analyses were higher, up to 3.7 (table 2), but without any evidence for exposure-response relations.
We implemented a group based exposure assessment strategy which has been described in detail previously.17 Although this approach is expected to result in less attenuation of risk estimates than individual exposure measurements,28 misclassification of exposure may be considerable and would reduce the chance to detect real associations, if any. However, the basic categorisation of workers into those performing repetitive work task and those doing varied work is reliable and findings were consistent across the crude and the refined exposure assessments.
Quite a large proportion of workers (277) were excluded because they could not be allocated to a task group, and it proved unfeasible to organise additional separate exposure assessments. This may have bearings as to the external validity of the study but is not expected to bias the risk estimates.
The stress profile inventory that we used to measure stress reactions has not been validated against external gold standards.18 It is not known to which extent the somatic, emotional, and cognitive symptoms reflect reactions to stressors. Several of the symptoms included in the Setterlind questionnaire are unspecific health complaints that could be caused by various somatic disorders and conditions not related to external stressors (cf table 3). It has recently been shown in longitudinal analyses of these data that stress symptoms predict development of regional pain.10 Perhaps the stress profile is reflecting individual susceptibility to development of pain rather than reactions to job related stressors. Moreover, it must be acknowledged that the findings of this study do not contradict that psychosocial factors in general are related to pain perception and reporting.
The Setterlind stress profile inventory contains 18 questions on various symptoms. Answers were given equal weight to an overall summary stress score, which has a skewed continuous distribution without a natural or logical cut-off value to define individuals with and without stress. The selected cut-off values for this study were arbitrary and an alternative selection of cut-off values could result in other findings. Therefore we repeated the main analyses using lower as well as higher cut-off values to define stress and change in stress level, but the point estimates were in the same range. Thus our findings are not dependent on the selection of stress score cut-off values.
More sophisticated statistical analysis based on continuous stress scores is possible but would introduce other methodological issues. We focused on a discrete disease outcome in order to give priority to effects that may be of clinical relevance. This corresponds to the upper tail of the stress score distribution while variation in the lower end is of less interest. Analyses based on the continuous outcome measure would give weight to mean values, and strong assumptions with respect to the linearity of the stress scale would be needed. Nevertheless, sensitivity analyses of the within-person change in the summary stress score between baseline and the first follow up round did not indicate that we missed any effect of repetitive work on development of stress symptoms by giving priority to the less sensitive discrete disease outcome strategy.
Psychosocial stress mechanisms related to repetitive work could operate at a subconscious level that escapes the individuals’ perception, interpretation, and reporting. For instance, psychosocial work factors (job demands, lack of control) might influence or be related to ergonomic factors such as repetition and posture that have been identified as risk factors for musculoskeletal pain.3 Thus, work related psychosocial factors could contribute to musculoskeletal pain even in the absence of stress symptoms (fig 1).
While the initial participation rate of 74% was within the range of the acceptable, only some 45% of workers enrolled at baseline participated in the last follow up examination (table 2). The main reason for the dropout was a high worker turnover, transfer of textile companies to other countries, and logistic difficulties in keeping track of workers once they left the companies to get jobs at other sites. The dropout was not strongly related to health indicators at baseline, although the risk of dropout given stress symptoms at baseline was slightly increased in workers with repetitive work (OR 1.6, 95% CI 1.0 to 2.6) compared to other workers (OR 1.0, 95% CI 0.5 to 1.9. Therefore we do not believe that dropout biases our findings substantially. The declining incidence of stress symptoms during follow up most likely reflects a survival phenomenon since the remaining part of the population still at risk during later rounds of examinations is expected to be less vulnerable. Incident cases of stress were not captured exactly at the time of appearance but were identified by repeated cross sectional surveys of stress symptoms during the preceding four weeks. The effect of this design is an underestimate of the true incidence since stress symptoms may have appeared and disappeared in the intervals between examinations. On the other hand, an analysis of recovery from stress symptoms indicates that in a majority of workers, stress symptoms are not very transient. Although our method of identification of incident cases will reflect aetiological as well as prognostic factors, it is not clear how this could result in biased estimates of associations between exposure and outcome.
All analyses were adjusted for several potential confounding factors. We are not aware of any well established determinants for stress symptoms that were not controlled for—perhaps with the exception of coping ability. Stress coping skills can be considered as a measure of individual susceptibility. Individuals who are able to cope with job strain may be less likely to develop stress symptoms. If so, the sensitivity to detect an effect of repetitive work on development of stress symptoms might be increased by restricting the analyses to the subset of participants with limited coping capability. However, data on coping abilities were not collected.
A low algometric pressure threshold was associated with an increased development of stress symptoms in longitudinal analyses. Since repetitive work could result in muscle tenderness and perhaps lowering of the algometric threshold, we repeated the main analyses without including this variable in the regression models. However, we obtained essentially the same relations between repetitive work and development of stress symptoms (data not shown).
Biological measures of stress would probably be needed to further investigate the extent to which work related factors are related to stress development. While earlier studies on links between job strain and stress hormones in urine and blood samples have been contradictory, recent studies in schoolteachers and students consistently indicate that job strain is associated with increased free cortisol concentrations in saliva early in the working day.29,30 Sluiter et al recently reported similar endocrine reactions in medical staff during and after treatment of patients in life threatening emergency situations.31
In conclusion, our findings do not indicate that objective measures of monotonous and repetitive work are associated with occurrence or development of stress symptoms, but small effects cannot be ruled out. Thus, the results do not support the hypothesis that regional pain in repetitive work is directly mediated by job related mental stress reactions. A major limitation to this interpretation is the lack of an externally validated instrument to measure stress reactions. Furthermore, the findings do not exclude the possible impact of psychosocial job stressors on pain reporting through other pathways bypassing stress symptoms.
Acknowledgments
The study was supported by grants from the Danish Medical Research Council and the Danish Work and Environment Fund. We are indebted to Kurt Rasmussen, Janus Kvamm, Birgit Juul Christensen, and Charlotte Brauer for their assistance in organising the study.