Article Text

Abstract
Welder’s siderosis occurs as a consequence of the inhalation of iron dust. The iron overload of welder’s siderosis is usually considered to be confined to the lungs. Here we present three proven cases of welder’s siderosis associated with evidence of increased total systemic iron stores, as evidenced by increased serum ferritin levels. Multiple investigations including molecular genotyping for the common mutations found in genetic haemochromatosis failed to prove this was due to haemochromatosis, nor was there any evidence of any other recognised cause of systemic iron overload. Thus the systemic iron overload described seems likely to be due to either occupational exposure, an uncharacterised genetic haemochromatosis, or a combination of both.
- ferritin
- iron overload
- siderosis
Statistics from Altmetric.com
Pulmonary siderosis may occur as a consequence of the inhalation of iron dust. This can occur in a number of occupations including welding. Welder’s siderosis was first described in 19361 and occurs in about 7% of arc welders, the presence of radiological opacities being related to the duration of occupational exposure.2 The iron overload of occupational siderosis is usually considered to be confined to the lungs.3 Here we present three cases of welder’s siderosis associated with evidence of increased total systemic iron stores, as evidenced by increased serum ferritin levels and we discuss the possible causative mechanisms.
CASE 1
A 40 year old white welder was referred in 1985 because of an abnormal chest xray examination, performed during a self limiting chest infection. He was an ex-smoker of about 10 pack-years, drank about 8 units of alcohol per week, and was a welder. He had no family history of note and physical examination was unremarkable. The chest radiograph revealed fine mottling throughout both lung fields consistent with siderosis.
This man had worked as a welder for 20 years, being employed by a number of companies over that time period. He had done various types of welding but mainly metal arc welding. He had welded in a number of different environments, some of which were poorly ventilated, this being the case particularly in his earlier years of employment.
At the time of presentation his lung function showed normal spirometry, a total lung capacity (TLC) of 87% predicted, and a transfer factor for carbon monoxide of 86% predicted. He remained well until 1988, when he had an episode of haemoptysis. A bronchoscopy was done, which appeared endoscopically normal. Transbronchial biopsy specimens revealed rather fibrous alveolar tissue with profuse Perl’s positive haemosiderin granules within macrophages, suggesting pulmonary siderosis.
Further laboratory investigation revealed a normal full blood count, and renal and liver function tests, but an increased serum ferritin level of 1010 μg/l (normal 30–300). Serum iron was 27.1 μmol/l (range 13–32) and total iron binding capacity 51.8 μmol/l (45–70), giving a slightly increased serum transferrin saturation of 53% (normal 15–45%). Systemic iron overload was thus presumed and fortnightly venesection therapy was started, reducing to monthly after 18 months. In 1991, after three years of therapy, the ferritin level had returned to normal at 64 μg/l, so venesection was stopped. However, by this point the patient had developed obstructive lung function with a forced expiratory volume in 1 second (FEV1) of 65% predicted and an FEV1/FVC ratio of 61% with mild breathlessness for which he was treated with inhaled corticosteroids and β agonists.
He remained clinically stable under regular observation but in 1997, six years after stopping venesection, it was noted that his ferritin had risen to 673 μg/l. After resuming fortnightly venesection for six months, this reduced to normal at 121 μg/l. Venesection was then stopped again but ferritin rose to 301 μg/l a further 12 months later, so venesection was resumed in 1999 and continues to the present. To date this patient has had around 75 units of blood venesected but at no point has he become anaemic.
In 2000 the patient was referred for formal hepatological assessment. There remained no signs or symptoms of chronic liver disease and liver function tests were normal. Molecular genotyping revealed that the C282Y and H63D mutations were absent. Percutaneous liver biopsy was done and histology showed only mild steatosis with no evidence of iron deposition or other histological abnormalities. He remains well, with mild to moderate airflow obstruction, and continues to weld for a living. This patient has only one sibling, a sister, who attended for family screening but serum ferritin was within the low normal range.
CASE 2
A 37 year old white welder presented in 1985 because of an abnormal chest x ray examination, performed following a self limiting chest infection. He was a non-smoker and rarely drank alcohol, but had been a welder for 20 years; his work also included metal grinding. Like case 1, he had worked in a number of companies over the years and did mainly metal arc welding; also, his more recent employment was in a better ventilated environment then at the start of his time as a welder.
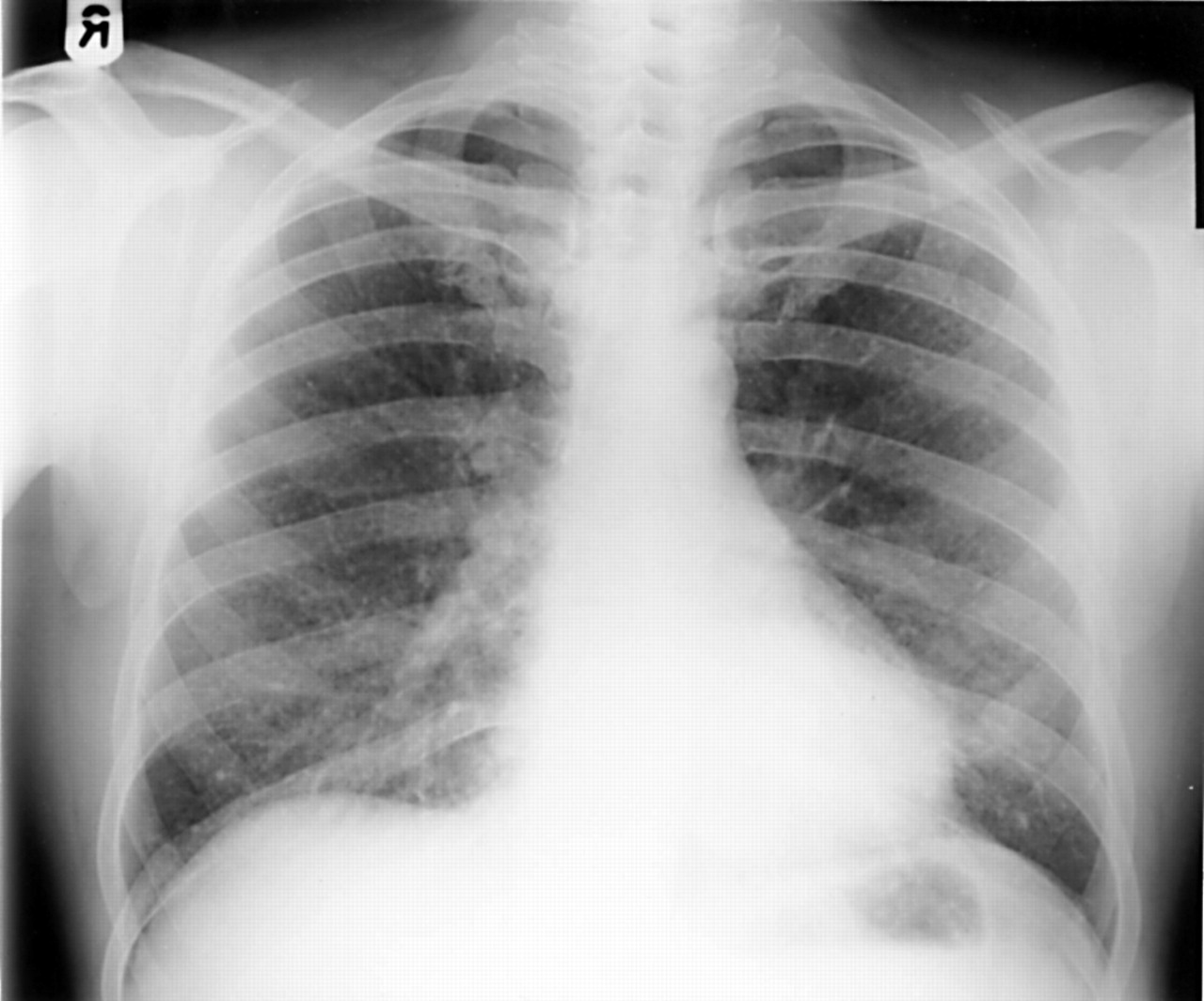
There was no family history of pulmonary or liver disease and examination revealed no abnormal physical signs. Chest xray and thorax computed tomography examination showed reticular shadowing and small opacities (figs 1 and 2). Lung function revealed normal spirometry and total lung capacity with a Kco of 78% predicted. Bronchoscopy appeared normal. Transbronchial biopsy specimens contained alveolar tissue with large amounts of haemosiderin laden macrophages within the pulmonary interstitium and to a lesser extent the alveolar spaces, with some interstitial fibrosis.
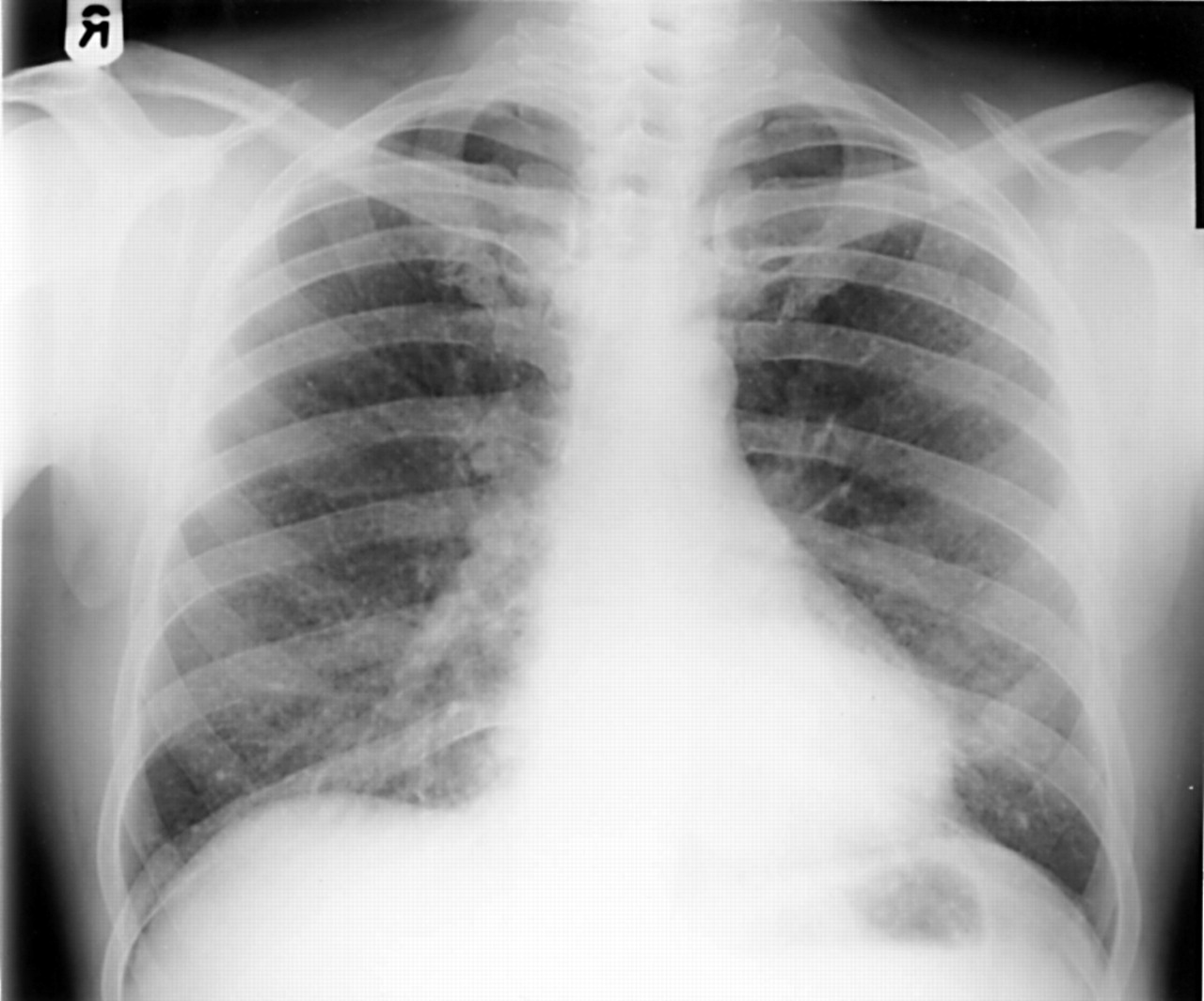
Postero-anterior chest radiograph of case 2, showing fine reticular shadowing and small opacities consistent with siderosis.

Computed tomography of the thorax in case 2, showing fine reticular shadowing and multiple small opacities consistent with siderosis.
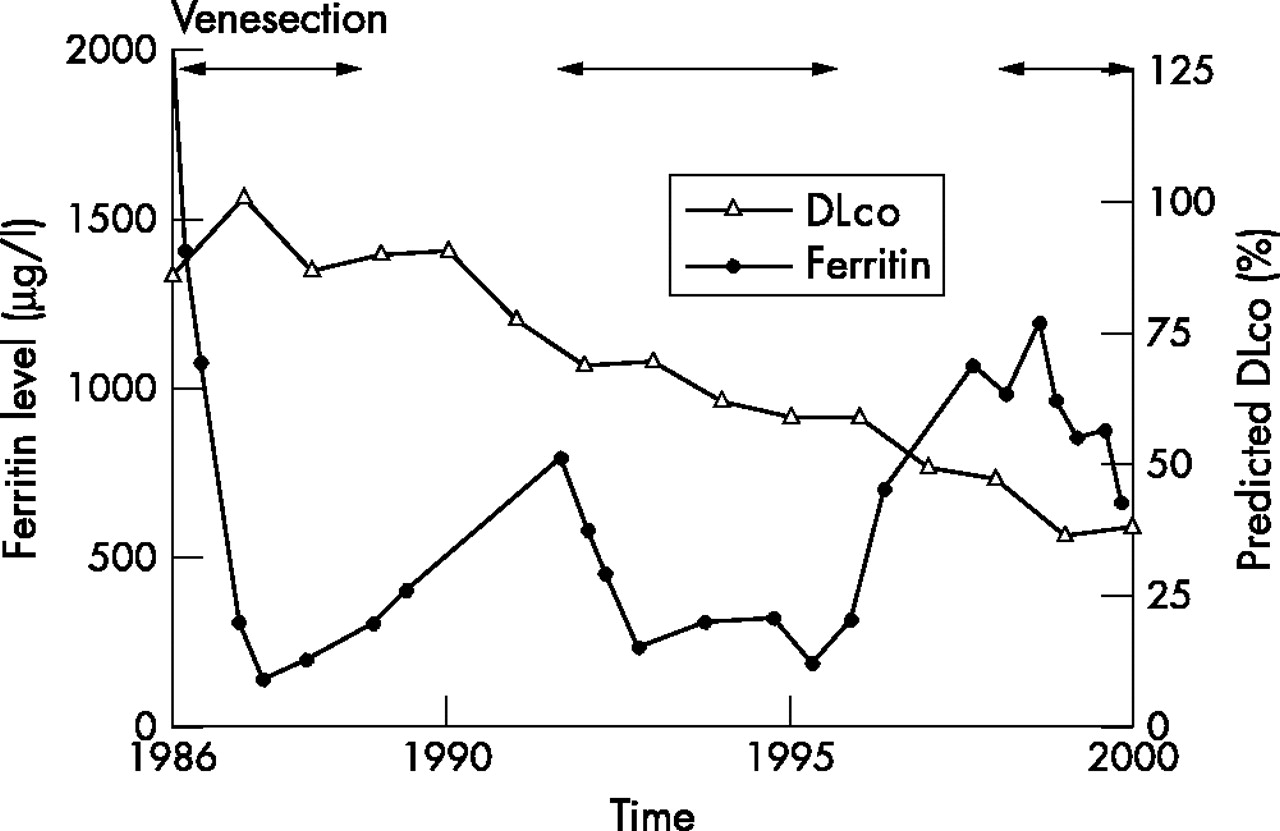
Further laboratory investigation revealed a normal full blood count, and renal and liver function tests, but serum ferritin was 2010 μg/l (range 16–330) (see fig 3). Serum iron was 20.7 μmol/l (range 13–32) and total iron binding capacity 52.5 μmol/l (45–70), giving a serum transferrin saturation of 39%. However, in view of the reproducibly increased ferritin levels, systemic iron overload was presumed and regular fortnightly venesection was commenced in 1986. The ferritin level fell slowly to within the normal range at 130 μg/l some 16 months later, at which point the frequency of venesection was reduced to monthly. Four years later in 1991 his ferritin was 296 μg/l and venesection was stopped. Throughout this period he remained well apart from an admission to hospital with mycoplasma pneumonia. At this stage he had mild airflow obstruction: FEV1 was 84% of predicted, FEV1/FVC ratio was 69.7%, and the mildly reduced DLco was 69% of predicted.
{kind=link}
{kind=link}
{kind=link}
Changes in serum ferritin and transfer factor for carbon monoxide (DLco) over time in case 2, showing that repetitive venesection decreased the serum ferritin but not the DLco. Serum ferritin then increased on each occasion when venesection was stopped.
Main message
-
These cases suggest the possibility that welder’s siderosis may cause total body iron overload.
After stopping venesection, his ferritin started to rise again; within eight months of stopping venesection it was 789 μg/l, so monthly venesection was started and continued till 1996 at which time his ferritin was 175 μg/l. A further trial without venesection between 1996 and 1998 again led to a rise in his serum ferritin to 1246 μg/l; venesection was again resumed, continuing up to the present.
In 2000 he was referred for formal hepatological assessment. There remained no signs of chronic liver disease; laboratory investigations revealed normal liver function tests and no evidence of diabetes mellitis or pituitary or testicular dysfunction. Molecular genotyping for the most common haemochromatosis genotypes (C282Y and H63D) showed that the C282Y mutation was absent but he was heterozygous for the H63D mutation. Percutaneous liver biopsy was performed; histology showed minimal haemosiderin restricted to Kupffer cells. There was no hepatocellular haemosiderin as found in primary haemochromatosis, and there were no other histological abnormalities. Quantitative iron measurement showed a hepatic iron index of 0.34 (normal <1.5).
To date this patient has had over 150 venesections from 1985 onwards, but has never been anaemic; his ferritin is now 450 μg/l. He continues in the same occupation as a welder. Over the years he has become slightly breathless and his DLco has declined to 36% of predicted, although he still only has mild airflow obstruction, with an FEV1/FVC ratio of 61%. This patient has only one sibling, a brother who attended for family screening and was found to have greatly increased serum ferritin (see case 3).
Policy implications
-
A larger study should look into this possibility in a more objective fashion.
CASE 3
This 61 year old man is the elder brother (by 6 years) of case 2 and is also a welder. He was found to have a serum ferritin level of 1695 μg/l when attending for family screening. Apart from a greater duration of exposure to welding fumes than his younger brother, his occupational history is more or less identical as they have worked in the same foundries throughout their working lives. At presentation he considered himself fit and well, with no symptoms to suggest respiratory or hepatic disease. He smoked less than a cigarette a day and drank 8 units of alcohol a week.
Physical examination was completely normal. Chest x ray examination revealed bilateral fine opacities, which were less marked than in the other cases; computed tomography of the thorax was also consistent with mild pulmonary siderosis. Further investigation revealed normal liver function tests and a normal ultrasound of the liver. Serum iron was 16.7 μmol/l (range 13–32) and total iron binding capacity 50.5 μmol/l (45–70), giving a serum transferrin saturation within normal limits at 33% (normal 15–45%). Molecular genotyping revealed that neither the C282Y nor the H63D mutations were present. Lung function revealed a TLC of 108% predicted and an FEV1 of 112% predicted with an FEV1/FVC ratio of 66%, suggesting mild airflow limitation. The DLco was minimally reduced at 79% predicted. A percutaneous liver biopsy revealed increased stainable iron, predominantly periportal in distribution, within both hepatocytes and Kupffer cells. However, there was minimal inflammation and no hepatic fibrosis or cirrhosis. The possible merits of venesection therapy were discussed with the patient but in view of the absence of any symptoms, signs, or laboratory evidence of significant liver or respiratory disease despite his relatively advanced age (at which point genetic haemochromatosis might have been expected to be more clinically manifest if present), he made an informed decision not to undergo venesection but instead to undergo intermittent serum ferritin monitoring only.
DISCUSSION
The possibility of systemic iron overload occurring with welder’s siderosis has not been described previously but seems plausible, and our case reports suggest this is worthy of further evaluation. Cases 1 and 2 had marked siderosis, while case 3 has mild siderosis; however, all subjects had very high ferritin levels in the absence of any readily identifiable cause. Ferritin is the principal iron storage protein and in the absence of systemic inflammatory disease is a sensitive indicator of total iron stores.4 As an inflammatory marker, ferritin has been shown to be raised in a variety of chronic lung diseases,5 although the increased levels found in our subjects were considerably higher than those normally encountered in inflammatory lung disease.4
In cases 1 and 2, the cumulative number of venesections amounted to over 75 and 150 units respectively, each unit being approximately 450 ml. In both subjects the mean haemoglobin during this period was 145 g/l; taking into account increased gastrointestinal absorption of iron, this would suggest that the work related contribution to the venesected iron was 12–17 g in case 1 and 24–34 g in case 2. This extensive use of venesection occurred without the development of anaemia and was typical of the venection requirements for clinically overt genetic haemochromatosis.6 Haemochromatosis is difficult to completely disprove in our cases, particularly in cases 1 and 2 where liver histology was not obtained until several years of regular venesection had been completed and where hepatic changes may thus have been modified by treatment. However, liver function tests were normal at presentation in all cases and transferrin saturations were below the normal values found in clinically evident haemochromatosis, where a transferrin saturation of 60% or more is found, even while ferritin levels remain only modestly increased.7 Furthermore the C282Y mutation is present in around 95% of white people with genetic haemochromatosis and is probably the most important genetic risk factor.8 Heterozygosity for the H63D mutation as found in case 2 is considered a weak risk factor for iron overload states unless coexisting with the C282Y mutation in the same individual.8 Finally, none of the subjects had any history of multiple blood transfusions, drank excessively, or had excessive iron ingestion and none had any laboratory evidence of thalassaemia or sideroblastic anaemia. Thus the systemic iron overload described seems likely to be due to either occupational exposure, an uncharacterised genetic haemochromatosis, or a combination of both; there is no recognised association between haemochromatosis and overt lung disease.
None of these subjects have had any measure of the magnitude of the iron levels in the air at their place of work, although this would be of interest to us. It would not answer the basic question posed here—that is, whether the cause of the total iron overload in these subjects is their occupation of welding. The information gathered using either personal or stationary sampling would also be limited, as it would only give information about their exposure now. It would not provide information about their exposure down the years, as all of these subjects have been welders for many years and in all cases the working environment, with regard to the level of ventilation and dustiness, has improved down the years.
Transferrin provides the main means of iron transport, absorbing iron from macrophages of the spleen, bone marrow, and liver and also from epithelial cells of the liver (hepatocytes) and duodenal mucosa. In the lungs of subjects with siderosis such as those we have described, numerous intra-alveolar macrophages containing iron are seen in the lymphatic channels.9 In the cases reported here we speculate that systemic absorption of iron has occurred via lung macrophages. It is possible that genetic predisposition other than classical haemochromatosis may have contributed to excessive systemic iron absorption.
Welder’s siderosis was originally thought not to be associated with respiratory symptoms,10 but this may not be the case.11 The symptoms and lung function deficit found in welder’ siderosis are however mainly produced by other constituents of welding fumes, rather than just the iron. The lung function abnormalities and symptoms found in our patients are therefore most likely to be mainly due to these other constituents. There was evidence of fibrosis in cases 1 and 2, and this is likely to be due to concomitant silicosis, as many subjects with welder’s siderosis are also exposed to silica dust. The subject in case 1 also smoked, having given up three years before presentation, having consumed approximately 10 pack-years previously; although his total cigarette consumption was low and he only developed airflow obstruction some years after stopping smoking, it is still possible that smoking may have played a part in his subsequent development of airflow obstruction. Further supportive evidence in these cases would require follow up once these subjects have retired, as all of the cases wish to continue in their welding occupations at present. However, study of other welders with and without siderosis may help to elucidate the relation between occupational iron exposure and total body iron stores.