Article Text

Abstract
Objectives: To extend our knowledge of how exposure to neurotoxic substances during working life affects cognitive functioning in the long term. Does long term occupational exposure to organic solvents lead to aggravated cognitive impairment later in life?
Methods: A follow up was conducted of floor layers exposed to solvents and their unexposed referents (carpenters) 18 years after the baseline assessment. The pattern of cognitive changes in the two groups was compared, with the same 10 neuropsychological tests from the test battery for investigating functional disorders (TUFF) that were used at baseline. The study included 41 floor layers and 40 carpenters. A medical examination focused on health at the present and during the past 18 years. An extensive exposure assessment made in the initial study included questionnaires, interviews, and measurements. Additional exposure during the follow up period was minor, as explored in interviews at follow up.
Results: The entire group of floor layers did not deteriorate significantly more over time than did the carpenters. However, among the oldest subjects (>60 years), only floor layers showed decline in visual memory. Moreover, the most highly exposed floor layers deteriorated significantly more than their referents in visual memory and perceptual speed, and they tended to display larger decrements in motor speed. Significant dose effect relations were found; higher cumulative exposure was associated with decrements in visual episodic memory, perceptual speed and attention, and visuospatial skill.
Conclusions: The hypothesis that floor layers would deteriorate more in cognitive performance than their unexposed referents over a period of 18 years was partly supported by the results of this study. The results are consistent with the view that the negative effects of exposure to solvents may interact with the normal aging process, primarily at heavy exposure.
- solvents
- cognitive
- long term follow up
- TUFF, test battery for investigating functional disorders
- CNS, central nervous system
- CEIs, cumulative exposure indices
- rp, Pearson product-moment correlation
- CTE, chronic toxic encephalopathy
Statistics from Altmetric.com
- TUFF, test battery for investigating functional disorders
- CNS, central nervous system
- CEIs, cumulative exposure indices
- rp, Pearson product-moment correlation
- CTE, chronic toxic encephalopathy
Many studies during the past decades have focused on adverse effects on the central nervous system (CNS) after long term exposure to organic solvents—for reviews, see Anger1 and Baker.2 Neuropsychiatric symptoms and cognitive deficits have been the main manifestations of adverse effects. It remains unclear, however, how exposure to neurotoxic substances during working life affects mental and cognitive functioning later in life. One possibility is that subclinical deficits during working life may become manifest later in life, when the reserve capacity of the brain is diminished and compensation for an acquired impairment may be reduced.3–6 If so, dysfunctions may appear earlier than normal as a result of the combination of an increased rate of neuronal loss caused by the neurotoxic exposure and the normal age related neuronal attrition.7
There are some indications in the scientific literature of delayed effects on the CNS after earlier neurotoxic exposure. Age related cognitive impairments were shown to be larger among workers exposed to lead and organic solvents than in controls, even after controlling for exposure time8; a more pronounced age related decline in nerve conduction velocities was found in workers with high past exposure to mercury than in their referents, especially in the oldest people (>69 years), although the exposure did not differ significantly between younger and older people—that is, an age-exposure interaction7—and postural tremor and impaired coordination were related to age and years since the start of exposure, but not to dose indices among workers earlier exposed to mercury.9
In a recent study, trail making test performance declined more markedly with increasing age in patients diagnosed with chronic toxic encephalopathy (CTE) than in patients with similar symptoms and exposure but no diagnosis of CTE, or in healthy participants.10 This result may reflect the fact that the older patients with CTE were more exposed than the younger ones, or may reflect an interaction between aging and exposure, where the neurotoxic effect is added to the normal aging process.
It is well known that aging has an influence on cognitive functioning, although there are large individual differences in the magnitude of the impairment.11 There is also variability in the age at which age related decline in cognitive test scores first become apparent.12 Tests assessing general knowledge (tests of vocabulary and comprehension) show relatively modest age related changes across adulthood, whereas performance tests, such as digit symbol and block design, as well as tasks assessing episodic memory typically show a robust and gradual decline from early to late adulthood.6,11,12
Until the beginning of the 1970s, floor layers were exposed to high concentrations of organic solvents through the use of alcohol based glues and contact adhesives. In a study of chronic and acute effects on the CNS in floor layers,13 only marginally lower performance in neuropsychological tests was found in those who had been exposed for a long time (>20 years), compared with controls (carpenters) matched for age and occupational experience. There was, however, a negative association between the exposure indices and performance in some tests among floor layers with long professional experience. Especially glues based on alcohol tended to have some negative effects on the CNS. An increased prevalence of neuropsychiatric symptoms was also found in all floor layers, but these may reflect acute effects on the CNS.
The present study is a longitudinal follow up of these floor layers and their controls. The aim of the study was to answer the following question. Does long term occupational exposure to organic solvents lead to aggravated cognitive impairment later in life, due to interactions with the normal age related loss of neuronal reserve capacity? More specifically, have floor layers with heavy exposure to solvent based glues before 1970 deteriorated more in their cognitive performance than their unexposed referents when re-examined 18 years later?
MATERIALS AND METHODS
Subjects
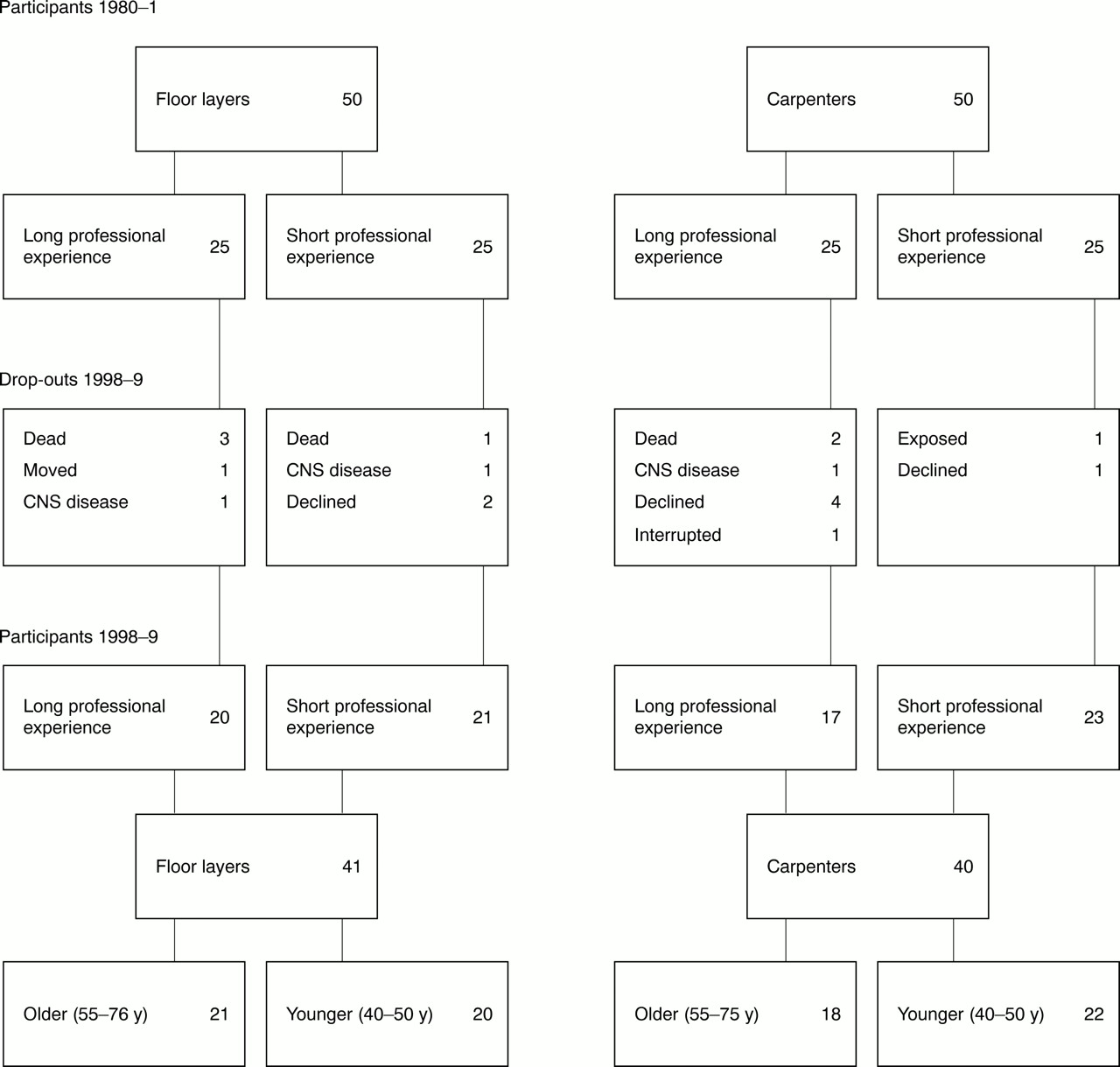
Fifty floor layers and 50 carpenters (referents), with similar age and occupational experience, participated in the study performed in 1980–1.13 Of these, 25 in each group had >20 years of occupational experience, and 25 had 5–10 years of occupational experience. All were men, active in their professions. The samples were randomly drawn from union registered floor layers and carpenters, who had responded to a questionnaire on professional experience and major work tasks. Details on selection and matching procedures are available elsewhere.13
In the present study, all subjects still alive and living in Sweden (45 floor layers and 48 carpenters) were approached with a letter inviting them to a follow up examination at the Department of Occupational and Environmental Medicine, Sahlgrenska University Hospital, Göteborg. Four floor layers and two carpenters had died and one floor layer had moved abroad. Those who did not answer the letter received a telephone call. Exclusion criteria were (a) present or past exposure to organic solvents in the reference group (to a greater extent than is usually found in carpenters), and (b) diseases that may markedly affect CNS functions—for example, cerebrovascular stroke with residual deficits, brain tumour, multiple sclerosis, Parkinson's disease, Alzheimer's disease, long term epileptic disease, and diagnosed chronic alcoholism.
One carpenter was excluded because of exposure to organic solvents as a painter during 4 years of the follow up interval. Two floor layers and one carpenter were excluded because of CNS disease (stroke, brain tumour, and chronic alcoholism with signs of nerve damage). Two floor layers and five carpenters declined the invitation, claiming lack of interest or motivation. One carpenter interrupted the examination after receiving a message that a close friend had died, and he declined further participation in the study.
The present follow up study therefore includes 41 floor layers and 40 carpenters, 81% of the participants in the initial study. Figure 1 illustrates the selection and drop out of subjects.

{kind=link}
Participants and those who dropped out of the study. The numbers in the boxes refer to the number of people.
Occupational experience and age are closely related. However, one floor layer and one carpenter with short experience were older than the others in their subgroups. Because our main interest in the present follow up study concerned age related changes, we decided to use age rather than occupational experience as the basis for the subgroups, including the two people just mentioned in the older subgroups. The older age groups include people ≥55 years of age (mean 62) and the younger age groups include people of 40–50 (mean 44).
Exposure
Occupational hygienists made an extensive exposure assessment in the initial study,13 including questionnaires, interviews, old measurement data from various workplaces, and new measurements at four workplaces. Exposure indices were calculated from the quantities of alcohol based glues (ethanol or methanol) and contact adhesives used at work.
Floor layers with long professional experience had used large amounts of alcohol based glues (20–30 l/day), and contact adhesives (5–10 l/ day) containing 75% solvents (benzene, acetone, toluene, and xylene) during the 1950s and 1960s and partly during the 1970s. The younger floor layers had rarely or never used alcohol based glues; hence, their exposure to such glues was not explored. Water based glues (glues with water and ≤5% organic solvents) were introduced to the market during the 1970s. Ten years later, at the time of the initial study, the quantities of contact adhesives used had diminished markedly (less than 1 l/day) and measurements showed considerably lower exposures.13
In the present study, the exposure of each person since participation in the initial study was explored in interviews by the same senior occupational hygienists who performed the exposure assessment in the initial study. The interviews focused on the development of working conditions and chemical products, and on the use of contact adhesives.
At the beginning of the 1980s, efforts were made to reduce or abandon the amount of volatile solvents, such as toluene and xylene, used even in water based glues in small quantities (≤5%). Starting in the middle of the 1980s, these solvents were substituted by solvents with low volatility—such as butyldiglycol acetate. The general trend was to use the same type of glue for different floor materials, and the predominant glues were based on polyvinyl acetate and polyacrylates. Water based contact adhesives are today considered to be technically just as good as the solvent based adhesives. The new glues, together with new designs of floor wells, have therefore reduced the need for solvent based contact adhesives.
Thus, during the 18 years that have elapsed between the baseline and follow up studies, the exposure has continuously diminished. During this period, contact adhesives have been used only to some extent (<0.1 l/day) in bathrooms and laundries. Moreover, since the 1980s, floor layers generally use a half mask with a charcoal filter during these tasks. Therefore, the increase of exposure to contact adhesives since the initial study was negligible, and there had been no further exposure to alcohol based glues.
For this study, two cumulative exposure indices (CEIs) were used; the quantities of alcohol based glues, and contact adhesives used at work up to the time of the follow up (the sum of the number of litres/day used each year). The mean (SD) CEI for alcohol based glues was estimated to be 319 (170) for older floor layers, whereas younger floor layers, as mentioned already, were not exposed to this type of glue. The mean (SD) CEI for contact adhesives was estimated to be 65 (47) for older floor layers and 12 (SD 11) for younger floor layers.
The solvent exposure of the carpenters was also assessed but was found to be negligible compared with the floor layers, and the quantities and concentrations have no relevance for potential adverse health effects.
Most of the younger subjects were still occupationally active. Exceptions were one floor layer who was studying, two carpenters who were unemployed, and one carpenter granted early retirement. Among the older subjects seven floor layers and nine carpenters were occupationally active. One floor layer was unemployed, seven floor layers and seven carpenters were retired, and six floor layers and two carpenters were granted early retirement. Most of the occupationally active subjects were still active in their occupations as floor layers or carpenters. Exceptions were five floor layers (two older and three younger subjects) and one younger carpenter, who had changed occupations. None of these had work or a hobby that should affect their cognitive or motor function.
Medical history and examination
The medical follow up included an interview about health at present and during the past 18 years with emphasis on disorders of the CNS. A general medical and neurological examination was performed. All participants were seen by the same senior physician. Blood and urine samples were also analysed, screening for vitamin B12 deficiency, thyroid disease, diabetes, and markers for alcohol misuse.
As could be expected, in a group of men between 40 and 76 years of age, various medical conditions were found. Nine floor layers and nine carpenters had a history of cardiovascular disease. Four floor layers and one carpenter were diabetic, one of whom was detected by increased plasma glucose in the present study. Also, the following conditions that could possibly affect CNS function were found: one floor layer was suspected of having obstructive sleep apnoea syndrome, one had previously misused sleeping pills, and one had been diagnosed as having a chronic toxic encephalopathy caused by exposure to organic solvents. One carpenter was treated for vitamin B12 deficiency. Seven floor layers and three carpenters had a history of depression.
Six floor layers and four carpenters were current smokers, and 22 floor layers and 17 carpenters were ex-smokers. One floor layer but no carpenter reported a mean alcohol consumption above 400 g/week at which level mild neurocognitive deficits have been reported.14 Another floor layer had a temporary high alcohol consumption, as the examination had to take place during a 2 week leave from work abroad.
The physical examination showed that 12 floor layers and six carpenters had a systolic blood pressure above 160 mm Hg or a diastolic pressure above 95 mm Hg. Three floor layers versus none of the carpenters had clear signs of polyneuropathy (one diabetic and one with previous alcohol misuse). Four floor layers and two carpenters had postural tremor or intention tremor.
Blood chemistry showed increased liver enzymes in five floor layers and five carpenters, in most cases increased γ-glutamyl-tranferase. Thyroid hormone concentrations were all normal, as were plasma concentrations of methyl malonate.
Neuropsychological tests
We used the same 10 neuropsychological tests from the test battery for investigating functional disorders (TUFF)15 that were used in the initial study. These include the following functional domains: verbal understanding (synonyms), reasoning (figure classification), visuospatial skill (block design and unfolding), perceptual speed and accuracy (digit symbol, identical numbers, and dots), motor speed (bolt, two handed, and pins, one handed), and visual episodic memory (Benton visual retention test). Two aspects were evaluated on the dots test, namely dots-speed and dots-accuracy (number of missed or incorrect markings), and on the Benton visual retention test, namely Benton-correct (the number of correct reproductions) and Benton-error (the total number of errors).
Alternating between floor layers and carpenters, all subjects were examined by the same experienced test leader with tests presented in a standardised order. The test leader knew their occupation but not the degree of exposure. Visual acuity and colour vision were checked for each subject before the test session started. Reading glasses were used if needed.
Statistical methods
The test results were analysed with analyses of variance (ANOVAs) with repeated measures. For analyses of test results relative to exposure, multiple linear regression analyses were performed for all tests. The model included previous test results, age group, and cumulative exposure index. The reason for including previous test results was because our main interest was to compare the cognitive changes in floor layers and carpenters between baseline and follow up assessment. Age, being the most natural source of change, was included (two age groups) as the second covariate. The CEIs for alcohol based glues and contact adhesives were included one at a time or both together to explore their explanatory potential. The limit for significance was set to p<0.05. Correlations calculated refer to Pearson product-moment correlation (rp). All calculations were done with the SAS software package (SAS Institute, Cary, NC, USA).
RESULTS
Group mean test scores, stratified by age groups, are shown in table 1. The test results were analysed with 2 (exposure group: floor layers, carpenters) × 2 (age group: older (55–76), younger (40–50)) × 2 (time: baseline, follow up) mixed ANOVA with repeated measures on the last factor. The results of these analyses are indicated in table 2.
Test results (means (SD)) in referents (carpenters) and floor layers, younger and older subjects, at baseline and follow up
p Values of the ANOVA on the entire samples of floor layers and referents
As expected, deterioration in test performance from baseline to follow up, regardless of occupation (main effect of time), was found in tests of general intelligence (reasoning), visuospatial skill (block design), perceptual speed and attention (digit symbol, identical numbers, dots-speed), and motor speed (bolt). By contrast, vocabulary (synonyms) increased over time, mainly in the younger subjects.
Another expected finding was that the older subjects (55–76 years of age) performed worse than the younger subjects (40–50 years of age), carpenters as well as floor layers (main effect of age group), in all tests but synonyms. In the initial study, this age related difference in performance was found in three tests only (digit symbol, bolt, reasoning). However, older floor layers did not perform worse than older carpenters—that is, age group did not interact with exposure group. By comparison with their performance at baseline, only the older subjects deteriorated on identical numbers, and a larger deterioration among older subjects than younger subjects was found on bolt (age group × time). In synonyms, younger subjects improved their performance more than the older ones.
Floor layers showed a significantly poorer performance than carpenters (main effect of exposure group) in one test only—namely, block design, assessing visuospatial skill. There was a slight tendency towards a more pronounced deterioration over time in floor layers than in carpenters (exposure group × time) on digit symbol, assessing perceptual speed.
A closer inspection of the data showed that the older floor layers displayed a more pronounced mean deterioration between baseline and follow up than any other subgroup in abstract visuospatial reasoning (unfolding) and in two handed motor speed performance (bolt). However, the within group variability was relatively large, which may explain the fact that these interactions did not reach significance. The only significant three way interaction (exposure group × time × age group) obtained was found for reasoning, where, contrary to our hypothesis, the older referents deteriorated more over time than any other subgroup.
As aging is closely related to increasing cumulative exposure, and as we found a greater influence on cognitive functioning with progressive age, we also made a separate analysis of the test results for the oldest subjects only (>60 years of age at follow up). These groups included 12 floor layers and 10 carpenters, and their group mean test scores are shown in table 3. The analysis showed some tendencies towards more pronounced decrements in floor layers. Only floor layers decreased their performance in Benton-correct, and the decrement over time was twice as high among the oldest floor layers as in the oldest carpenters in sustained attention (dots-speed), although these interactions did not reach significance, again due to large within group variability, especially on the dots-speed test.
Test results (mean (SD)) at baseline and follow up in the oldest subjects (>60 y at follow up), and in the most highly exposed floor layers (CEI ≥360 for alcohol based glues and CEI >50 for contact adhesives)
Test results related to exposure indices
Most highly exposed subjects
Analyses were made including only subjects with the highest cumulative exposure (CEI ≥360 for alcohol based glues (n=10) or CEI >50 relating to contact adhesives (n=10)). The overlap between the two groups was 50%. All of these subjects belonged to the older age group (range 55–76 years); thus, only the older carpenters (n=18) were used as referents. Group mean test scores are shown in table 3 (older carpenters in table 1).
At high exposure to alcohol based glues, floor layers performed worse than carpenters on block design (p<0.01) and marginally so on unfolding and Benton-error (p=0.07). They also showed larger decrements between baseline and follow up than their controls in identical numbers (p=0.03), Benton-correct ((p<0.01), and Benton-error (p=0.02), reflecting significant interactions between exposure group and time.
At high exposure to contact adhesives, floor layers again performed worse than carpenters on block design (p=0.04). Moreover, floor layers tended to deteriorate more from baseline to follow up (exposure group × time) than their controls in motor speed (bolt, p=0.09)).
Dose-effect relations
Within the exposed group, multiple linear regression analyses were performed for all tests to evaluate potential dose-effect relations. These analyses included previous test results, age group, and CEI (l/day×years) for alcohol based glues or contact adhesives. Only floor layers with more than 20 years in the profession at the time of the baseline assessment, and now belonging to the group of older floor layers (55–76 years) were included in the analyses, as only these subjects had been exposed to alcohol based glues. They were divided into two age groups, 55–60 years (n=9) and >60 years (n=12). The results of the regression analyses are displayed in table 4.
Results (p values) of the multiple regression analyses on the older floor layers (n=21); all associations reflect a negative effect of exposure on test results (the p values refer to the regression coefficients for the CEIs (left columns) or the interaction terms (right columns))
Alcohol based glues
Poorer test performance was significantly associated with higher CEI on dots-accuracy and the Benton visual retention test (correct and errors), and also, marginally, on synonyms, unfolding, dots-speed, and block design. In line with our hypothesis, the oldest subjects displayed a significantly more pronounced deterioration between baseline and follow up with increasing CEI (exposure × age group) in unfolding. There was also a tendency towards an interaction between exposure and age group for synonyms. However, higher exposure was associated with a decline in performance among subjects 55–60 years old, but not in the oldest group, contradicting the notion of a progressive deterioration with aging at higher CEI in this particular test.
Contact adhesives
For contact adhesives, inferior test performance was significantly associated with higher cumulative exposure on block design and identical numbers, and marginally in digit symbol, dots-speed, and Benton-correct. Thus, higher CEI was associated with a more pronounced deterioration over time, from baseline to follow up. The oldest subjects (>60 years) tended to deteriorate more with increasing exposure (exposure × age group) in digit symbol.
Models including both alcohol based glues and contact adhesives at the same time, yielded roughly the same results as models testing the exposure indices separately, although no effects of exposure were found for synonyms and unfolding. Block design was mainly affected by exposure to contact adhesives, which was not shown in the separate analyses. The correlation between the two exposure indices was 0.59 (rp).
Thus, clear dose related performance decrements over a lengthy period were shown. Higher cumulative exposure of alcohol based glues or contact adhesives was associated with deteriorations in tests assessing visual episodic memory, perceptual speed and attention, and visuospatial skill. Moreover, the deteriorations in a test of abstract visuospatial reasoning and a test of perceptual speed were most pronounced in the oldest subjects, which is in line with the hypothesis on a progressive deterioration with aging at higher CEI.
The decline in test performance associated with 20 years use of 20 l alcohol based glues/day (CEI of 400) was equivalent to 15%–25% decline in visuospatial tasks (unfolding and block design), and 15%–85% deterioration in the visual memory test (Benton-correct and Benton-error). Block design was more affected than unfolding, and Benton-error much more than Benton-correct. The magnitude of the performance deficits associated with exposure may also be compared with that occurring as part of the normal aging process. Calculations using the regression coefficients for age group and exposure showed that the point estimates of the performance decline seemed comparable with about 30 years of aging on visuospatial tasks and 15–45 years on the memory task. Performance deterioration associated with 20 years use of 5 l/day of contact adhesives (CEI of 100) was equivalent to about 25% decline in visuospatial skill (block design), corresponding to about 10 years of aging, and to about 10% decline in tests assessing perceptual speed and visual memory, corresponding to about 10 and 5 years of aging, respectively.
Test results after the exclusion of five subjects
The medical histories and examinations showed that three subjects (two floor layers, one carpenter) reported mild to moderate depressive symptoms with ongoing or recent medication with antidepressive drugs. One floor layer reported habitual high alcohol consumption (see above), and another floor layer was in the middle of an intermittent period of high alcohol consumption at the time of the examination. All five subjects belonged to the younger age groups. These conditions were not severe enough to meet our exclusion criteria, but, although unlikely, we could not rule out the possibility of a negative influence on the test results. Therefore, all analyses were repeated excluding these five subjects.
The results of the analyses of variance showed only minor changes and did not change the general direction of the original results. It may be noted, however, that the three way interaction between time, exposure group, and age group for reasoning was weakened (only borderline significant), due to the fact that the mean score in younger floor layers increased slightly. The results from the dose-effect analyses were not affected, as these included only the older age group. Thus, the pattern of results reported in this paper cannot be attributed to the performance of these five subjects.
DISCUSSION
The present study is a longitudinal 18 year follow up of a group of floor layers, previously heavily exposed to solvent based glues, and their controls (carpenters), assessing cognitive functioning and health. The additional exposure during the follow up period has been minor.
The hypothesis that floor layers would deteriorate more in cognitive performance over a period of 18 years than their unexposed referents received partial support from the results of this study. The group of floor layers tended to deteriorate more over time in perceptual speed than carpenters. Among the oldest subjects (>60 years), only floor layers decreased their performance in visual episodic memory, and the oldest floor layers also tended to deteriorate more in sustained attention. Moreover, the floor layers most highly exposed to alcohol based glues deteriorated significantly more over time in visual episodic memory and perceptual speed than their referents. High cumulative exposure to contact adhesives was associated with a tendency towards larger decrements in motor speed. Older floor layers also showed more pronounced decrements over time than any other subgroup in abstract visuospatial reasoning and motor speed, although within group variations were too large to give any significant interactions.
Dose-effect analyses within the exposed group showed stronger associations between exposure and cognitive performance. Higher cumulative exposure to solvents was significantly associated with decrements in tests assessing visual episodic memory, perceptual speed and attention, and visuospatial skill. The negative associations between exposure and performance were more pronounced at the follow up than at baseline,13 providing support for the hypothesis that neurotoxic effects may interact with the aging process. These decrements were associated with use of >10 l of alcohol based glue/day during 10–20 years or >5 l of contact adhesive/day during 5–10 years. Measurements in the early 1970s showed exposure concentrations in Swedish floor layers clearly above the occupational exposure limits at that time.13
To our knowledge, this is the first long term follow up study of a sample of workers exposed to solvents. Despite the lengthy follow up period of 18 years, we were able to re-examine 81% of the floor layers and their unexposed controls. Moreover, the exposure assessment in the initial study was extensive and individual exposure indices could be calculated for alcohol based glues and contact adhesives.
Previous follow up studies have focused on patients diagnosed with mild or moderate CTE, showing some normalisation of cerebral blood flow after the end of exposure,16 but mainly indicating persistent cognitive deficits as well as symptoms after follow up periods between 1 and 8 years.17–20
We found cognitive decline with increasing cumulative exposure to solvents in tests assessing visual episodic memory, perceptual speed and attention, and visuospatial skill. Note that adverse effects in neuropsychological tests assessing these functional areas typically characterise patients diagnosed with chronic toxic encephalopathy (CTE), and have often been reported in exposed workers in cross sectional studies since the 1970s.21–27
The finding of impaired performance in visuospatial skill in floor layers compared with their controls replicates the results from the baseline assessment of this sample.13 However, whereas this difference was found only in floor layers with long experience 18 years ago, the impairment now applied to the entire group of floor layers. Test performance related to the exposure indices gave similar negative associations as in the first study with reference to alcohol based glues (visual memory and visuospatial skill), whereas exposure to contact adhesives was negatively associated with additional tests compared with the initial study, and the functional domains affected (visuospatial skill, visual memory, and perceptual speed) were more similar to those associated with exposure to alcohol based glues.
Negative associations between exposure to contact adhesives and cognitive performance is in line with the general knowledge of the adverse health effects from substances included in contact adhesives, such as toluene, xylene, and ketones.13 The concentration of solvents is higher in contact adhesives (about 75%) than in alcohol based glues (about 20%). Contact adhesives were normally used in small rooms, such as bathrooms. On the other hand, alcohol based glues were applied on larger areas, which also resulted in high solvent concentrations in the air. Alcohol based glues contained ethanol and methanol. Separate calculations indicate that even at high air concentrations of ethanol, the uptake would be low. Methanol, being more toxic and taken up also through the skin,28 may be responsible for the associations found between impaired performance and exposure to alcohol based glues. Alternatively, the associations are due to contact adhesives, the use of which covaried with that of alcohol based glues. The relation between the two indices of exposure was relatively strong.
Significant relations between various exposure indices and cognitive performance have been reported in several studies. Bleecker et al reported significant associations between lifetime weighted average exposure to aliphatic and aromatic hydrocarbons in paint manufacturing workers and performance in tests assessing perceptual speed and attention, reaction time, and serial digit learning.29 In another study, poor results in tests of auditory memory and visual abstraction were significantly correlated with increasing exposure to industrial solvents in seamen on chemical tankers.30 In workers of various occupations exposed to solvents, significant dose-effect relations were found for symbol digit substitution in workers with more than 30 years of occupational exposure, and for paired associate learning after more than 10 years of occupational exposure.31 In a study of neuropsychiatric effects among house painters with previous long term heavy exposure to organic solvents,32 painters performed worse than carpenters in block design. Furthermore, the painters' performance in this test deteriorated with increasing cumulative exposure. The present results are in good agreement with these findings. Note, however, that other studies have failed to find significant correlations between various exposure indices and cognitive performance.23,33
The finding of generally declining performance in tests assessing reasoning, visuospatial skill, perceptual and motor speed, but not in vocabulary, is in accordance with previous findings of a robust and gradual age related decline in performance tests as opposed to a less pronounced decrement in verbal tests.6,12 In verbal tests, assumed to reflect crystallised intelligence, prior experience is crucial and the speed demands are limited. Requirements of speed and efficiency in finding solutions to novel problems characterise performance tests, considered to reflect more fluid aspects of intelligence. Thus, the higher performance for younger than for older subjects in all non-verbal tests in this study is in line with standard findings in publications on cognitive aging. It may be noted, however, that the age difference (younger v older subjects) was more pronounced at follow up than at baseline, where age differences were found only for three of the tests (reasoning, digit symbol, and bolt), suggesting that the negative effects of aging on fluid abilities increase from middle to late adulthood. In this study, age and exposure covary, but this fact was taken into consideration in the analyses.
Considering the validity of the present findings, the examinations and interviews at the follow up assessment were carried out in the same way as at baseline, including the same neuropsychological test battery. Exposure assessments and the medical examination were even performed by the same occupational hygienists and physician. The samples of floor layers and carpenters, although limited in numbers, were well matched on occupational experience and age from start, and they had almost identical mean scores of vocabulary in the initial study, indicating comparable primary intellectual levels. The participation rate in the present study was high (81%). Initially, the samples were randomly drawn from union registered floor layers and carpenters within a larger region. Thus, they may be regarded as highly representative for their occupational groups.
The repeated measures ANOVA requires that certain assumptions are met. As may be seen in table 1, the variances were similar across groups. Separate analyses also showed that the covariance over time was similar in floor layers and carpenters. Because many analyses were made (10 neuropsychological tests), some significant associations could be expected by chance. Therefore, taken alone, the overall associations between exposure group and performance (main effect in block design and interaction effect in reasoning) in table 2 should be interpreted with caution. However, when exposure indices were taken into account, the results clearly indicate impairment with increasing exposure across many domains, including visual episodic memory, perceptual speed and attention, and visuospatial skill (table 4). It is highly unlikely that these extended deficits reflect the number of comparisons made.
The persistence of inferior performance among floor layers compared with carpenters in block design, found both at baseline and follow up could reflect a primary difference between the groups, possibly due to selection. However, it is conceivable that visuospatial ability is requested and practised to a similar extent in both occupational groups—in floor layers for accurate planning and cutting of floor covers to fit in various floor spaces, and in carpenters for accurate manufacturing of details in accordance with drawings. Long term alcohol misuse has often been reported to negatively affect visuospatial ability.14,34 In this study, chronic alcoholism was among the exclusion criteria. Moreover, only one floor layer reported an average alcohol consumption above 400 g/week, at which level mild neurocognitive deficits have been reported,14 and another one had a temporary high alcohol consumption. Exclusion of these two floor layers did not alter the group difference found in block design. Also, there was a significant deterioration of block design performance with increasing cumulative exposure to contact adhesives and a tendency in the same direction for alcohol based glues. Thus, the deficit in visuospatial skill found among floor layers is more likely to be caused by the exposure to solvents.
Key messages
-
Cognitive decrements over an extended period (18 years) were found in a longitudinal study of floor layers previously exposed to solvent based glues.
-
Dose related deteriorations in test performance were found within domains of visual episodic memory, perceptual speed and sustained attention, and visuospatial skill.
-
The most highly exposed floor layers (high cumulative exposure) deteriorated more than their referents in visual episodic memory and perceptual speed.
-
The dose related decrements were sizable, resembling deficits resulting from 10 to 25 years of aging.
-
These results suggest that, despite the fact that the major exposure dates back 30 years, the negative effects of exposure may interact with the normal aging process, primarily in the most heavily exposed people.
Floor layers more often reported a history of depression, and some other health problems were also more common in floor layers than in carpenters. However, exclusion of subjects for whom we could not rule out the possibility of a negative influence on the test results did not alter the findings in this study. Moreover, as exposure to solvents may cause mood changes,35 the depressive symptoms found in floor layers in the present study as well as in the initial study,13 could in fact be initiated by the exposure.
In a long term perspective, exposure to solvent based glues seems to have a negative influence on cognitive functioning in the domains of visual episodic memory, perceptual speed and sustained attention, and visuospatial skill. Decrements over an extended time window (18 years) were found mainly with increasing cumulative exposure. The fact that the major exposure dates back 30 years is noteworthy. In general, then, the current results suggest that the negative effects of exposure may interact with the normal aging process, primarily in the most heavily exposed people.
These findings highlight the importance of continued efforts to reduce occupational exposure to organic solvents. Generally, the Scandinavian countries have been successful in those efforts, but in other countries exposure conditions may still be unacceptable.
Policy implications
-
Extensive individual exposure assessment, including quantitative indices, is important in research within this area to be able to recognise dose related decrements.
-
Including also workers no longer professionally active is important for two reasons; firstly, this approach will reduce the healthy worker effect; secondly, it will enhance the possibility of finding a potential interaction between an influence of neurotoxic exposure in the past and the process of aging.
-
In the clinical situation, the possibility of a causal relation between CNS dysfunction and earlier exposure to solvents should be considered although there may be a long latency between the end of exposure and the onset of the dysfunction, at least in the most heavily exposed people.
Acknowledgments
The study was approved by the committee of ethics of the Göteborg University. We thank Kerstin Ekberg for generously supplying data from the initial study, Gerd Granung and Birgitta Olofsson for assistance with blood and urine sampling, Annika Claesson and Kristina Wass for assistance with blood and urine sampling as well as data input, and Gunnel Garsell for administrative assistance. The Swedish Council for Work Life Research is gratefully acknowledged for financial support.